
Successful management of depression skull fracture in a boy with dog bite injury: A case report
2022-10-17 12:28:40AbdulkerimGokogluHasanTahsinGozdasSelimeOzenSonayGokoglu
Journal of Acute Disease 2022年5期
Abdulkerim Gokoglu, Hasan Tahsin Gozdas, Selime Ozen, Sonay Gokoglu
1Department of Neurosurgery, Private System Hospital, Kayseri, Turkey
2Department of Infectious Diseases and Clinical Microbiology, Abant Izzet Baysal University Faculty of Medicine, Bolu, Turkey
3Department of Pediatrics, Dr. Behcet Uz Children’s Disease and Pediatric Surgery Training and Research Hospital, ?zmir, Turkey
4Department of Pediatrics, Private Huma Hospital, Kayseri, Turkey
ABSTRACT Rationale: There are many cases of daily reported dog bite injuries around the world. However, craniofacial fractures owing to dog bites are quite rare. They are frequently seen in the pediatric age group.Here, we report the successful management of a pediatric patient with depression skull fracture due to a dog bite injury.Patient’s concerns: A 3-year-old boy was admitted to the emergency department with a complicated skull fracture due to a dog bite injury. In physical examination, the patient was neurologically intact. He had hemorrhagic scalp wounds. Cerebrospinal fluid was leaking on the right temporal and frontal sides.Diagnosis: Cranial computed tomography revealed pneumocephalus,brain edema, and compound fracture associated with right frontal concussion.Intervention: After decompressive craniectomy, duraplasty was performed by placing a galea graft. Depressed fractures were removed and subdural bleeding control was provided.Outcomes: Perioperative and postoperative periods were uneventful.Lessons: Emergency medicine physicians should control possible underlying fracture lines in pediatric head trauma caused by dog bites.
KEYWORDS: Craniocerebral trauma; Dog bite; Skull fracture;Pediatric patient; Cranial computed tomography; Cerebrospinal fluid leakage
1. Introduction
Dog bites are significant health problems. In dog bite injuries,many sequellae ranging from minor trauma to mortality may be encountered. In the United States of America, more than four million cases of dog bites are reported annually. Cranial fractures due to dog bites are very rare. They may present as skull fractures or craniofacial fractures. Although skull fractures are usually associated with facial soft tissue injuries, accompanying facial bone fractures are rarely seen. Children are the most affected age group from dog bite injuries. Many facial fractures from dog bites were reported in children under 16 years of age.
Dog bites may result in bone fractures, extremity loss, meningitis,brain abscess, and systemic infections including pneumonia and endocarditis[1]. Among these morbidities, cranial fractures are especially significant as they can cause neurovascular complications which usually require surgical repair[2].
Serious injuries are usually seen in the facial region whereas accompanying fractures are rarely seen which constitute less than 5%of the cases. Besides, clinicians should be alert to scalp lacerations,because the underlying fracture line can be subtle[3].
Here, we report a child with hemorrhagic scalp wounds after a dog bite. Cerebrospinal fluid (CSF) leakage was observed on the right side. So, a skull fracture was suspected and it was confirmed with cranial computed tomography (CT). Successful management of this case was afforded with surgical intervention and antimicrobial therapy.
2. Case report
Informed written consent was obtained from the patient’s parents for this case report, and this study was approved by the Ethical Committee of Kastamonu State Hospital.
A 3-year-old boy was brought to the emergency department by his parents because of a cranial dog bite injury. His past medical history and family history were unremarkable. Physical examination revealed the following: body temperature: 36.7 ℃; heart rate: 116 beats per minute; blood pressure: 80/50 mmHg. The patient was neurologically intact. He had hemorrhagic scalp wounds and CSF was leaking on the right temporal and frontal sides. Laboratory values were as follows: White blood cell: 11.3×103/μL (normal: 4×103/μL-10.5×103/μL); hemoglobin: 10.5 g/dL (normal: 12-17.5 g/dL); C-reactive protein: 0.90 mg/L (normal: 0-5 mg/L); erythrocyte sedimentation rate: 24/h (normal: 0/h-20/h). Cranial CT showed pneumocephalus, brain edema, and compound fracture associated with right frontal concussion (Figure 1). Rabies and tetanus prophylaxis were administered to the patient. Due to CSF leakage on the scalp, the patient underwent emergency surgery.
Besides complicated depression fracture, dural and brain laceration, brain edema, and pneumocephalus were detected. After decompressive craniectomy, duraplasty was performed by placing a galea graft. Depressed fractures were removed and subdural bleeding control was provided. Perioperative and postoperative periods were uneventful. There was no blood transfusion requirement.Postoperatively, the patient was followed in the intensive care unit for two days. Perioperative images of the patient and postoperative CT images are shown in Figure 2. Intravenous cefotaxime 4×750 mg, vancomycine 4×240 mg and metronidazole 4×125 mg were given to the patient for 10 d. Thereafter, the patient recovered completely without any complications. He was discharged with a recommendation of outpatient control. There was no sequellae or neurological deficit at postoperative first and third-month controls.
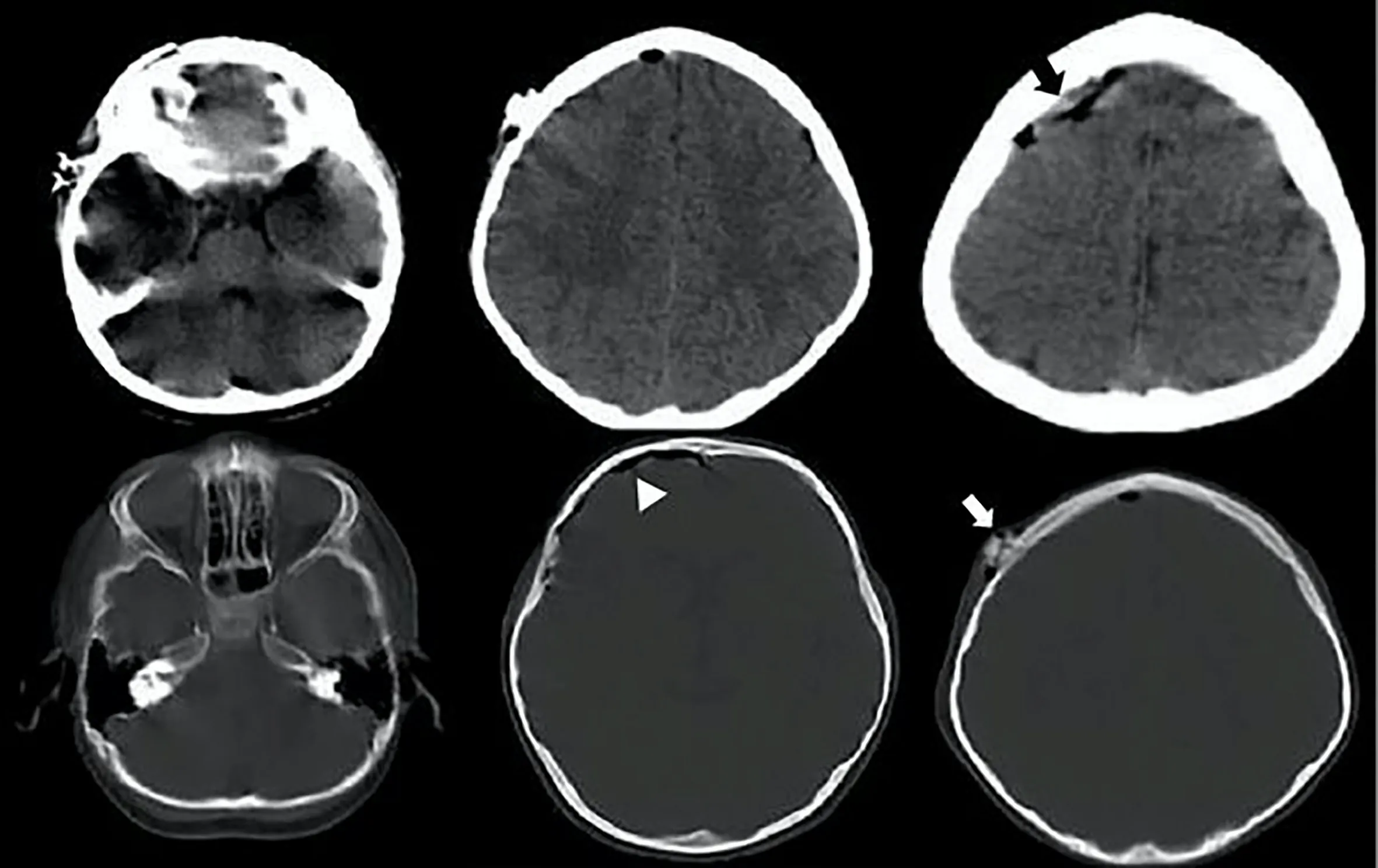
Figure 1. Pre operative cranial CT imaging of a 3-year-old boy revealed right frontal concussion (black arrow), pneumocephalus (white triangle), and underlying calvarial depression fracture (white arrow).
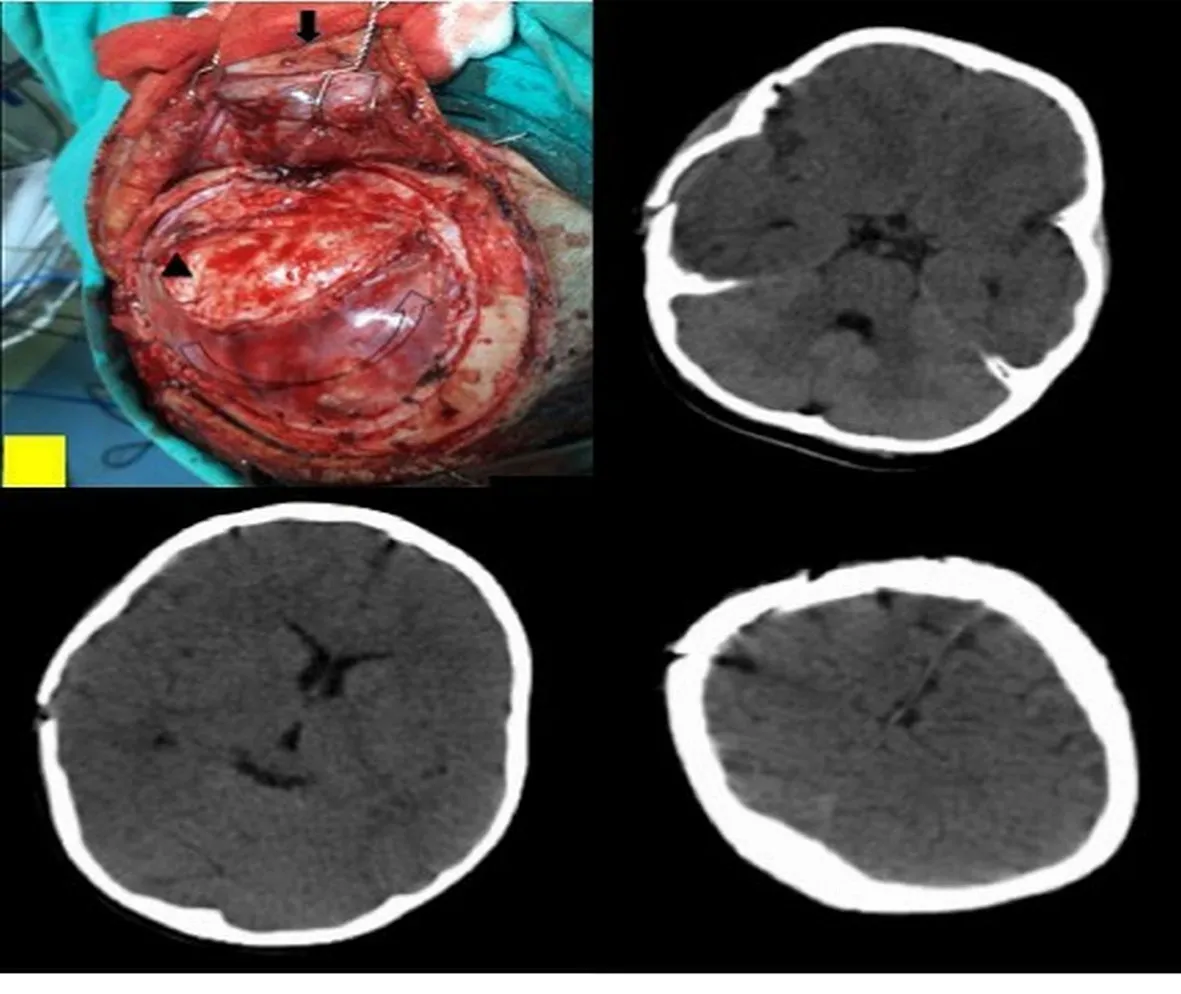
Figure 2. Per operative dog bite wound penetrating intracranial compartment through scalp (black arrow), dural laceration (black triangle), and galeal duraplasty(curved arrow) and post operative CT images.
3. Discussion
Dog bites may cause puncture wounds, skin and soft tissue lacerations, scalp injury, bone fractures, extremity loss, neurovascular injury, systemic infections, and even death. Although craniocerebral injuries owing to dog bites are rare, they can cause life-threatening conditions. So, they must be evaluated carefully.
Mortality can be seen as a result of bleeding or infection. Ruszinet al. reported an old woman who presented with extensive facial trauma after a dog bite and died from bleeding probably due to underlying warfarin therapy[4].
Cranial soft tissue injuries may be complicated with facial nerve injury, lacrimal duct injury, ptosis due to levator transection, bleeding requiring blood transfusion, and facial fractures. So, dog bites should be carefully examined in the pediatric age group in the presence of orbital, nasal, and jaw fractures[3].
Pinckneyet al. reported two dog bite cases. One of them was an 8-month-old girl with a head and neck injury. She had multiple lacerations on the scalp and left side of the neck. She also had a right parietal depression fracture. Also, numerous depression fragments at the right parietal and left occipital bone and a linear right parietal fracture were detected in cranial CT. Severe blood loss occurred preoperatively, and newly developed right subdural and bilateral intracerebral bleeding was detected by cranial CT. The patient was lost due to bleeding. The second case was a 4-month-old boy. He had lacerations on the calvarium, left neck, left eyelid, and right ear.Multiple depression skull fractures at the right frontal and parietal bone were detected by plain radiographs. Depressed fragments were removed with bleeding control. At follow-up, bone fractures were healed but persistent nerve palsies developed[5].
Steinboket al. described three pediatric cases with central nervous system injury due to dog bites. Two infants suffered from compound depression fracture as a result of head injury. In the older child,spinal cord injury occurred due to a tiger bite, and their two cases developed Pasteurella meningitis[6].
Kleinet al. described a case of perforating skull injury due to a dog bite who developed a Pasteurella multocida brain abscess[7].Similarly, Suttonet al. defined a case of brain abscess after a dog bite[8]. Santana-Monteroet al. described a cerebellar abscess in a 2-year-old girl due to a dog bite. They obtained a satisfactory outcome with neurosurgical intervention and antimicrobial treatment[1].
In the article by Weiet al. they reported that among a total of 1 201 pediatric cases with facial injuries due to dog bites, 17 cases developed facial fractures (1.4%). Of these 17 patients, 14 patients needed surgical repair. They underscored that facial fractures associated with dog bite injuries are rare, but they usually necessitate surgical intervention. The authors also highlighted that facial dog bite injuries must be evaluated for soft tissue injuries and underlying possible fractures[2].
Along with soft tissue injuries, dog bites rarely cause depression or skull fractures. There are a limited number of cases of depressed skull fracture due to dog bites in the literature[4.9.10]. Burnset al. described a depressed skull fracture in a 20-month-old girl after a dog bite. She had multiple puncture wounds on the neck and lacerations on the left ear and right occipital scalp. Intravenous antibiotic treatment was started on the patient. Cranial CT showed that a depressed fracture in occipital bone intruded into the cerebellum. Bone fragments were removed with surgical intervention; the wound was debrided, dural layer and scalp lacerations were closed. Antibiotic treatment was given to cover meningitis, and postoperative healing was uneventful.They emphasized that detailed examination under general anesthesia and sometimes radiological investigation was essential because lacerations can mask bone fractures[9].
Iannelliet al. described bilateral skull and brain injury in an infantdue to a dog bite. They mentioned that scalp injuries can penetrate intracranial compartments even if they seem to be small and limited in size and appearance. They underscored that this condition may be missed at first observation[10].
Occult cranial fractures may not be apparent at first examination due to the displacement of the scalp. Scalp lacerations should be carefully examined against the possibility of occult cranial fracture and underlying brain injury. Craniocerebral injuries should be explored, depressed cranial fractures should be irrigated, debrided,and elevated, and dural tears should be repaired. Appropriate antimicrobial treatment should be given to prevent meningitis and associated sequellae[9]. Patients should be evaluated for rabies and tetanus prophylaxis.
Our pediatric case suffered from cranial dog bite injury. He was conscious and his general status was good. However, after careful examination of the injury site in the emergency department, CSF leakage drew attention. Thereafter, cranial CT showed a fracture line. Not only surgical repair but also antimicrobial therapy provided successful resuscitation of our patient.
Scalp and soft tissue injuries must be carefully examined especially in the pediatric population. Penetration to intracranial compartments due to dog bites’ scalp injuries have been reported even if they seem to be small and limited in size and/or appearance which this condition may be missed at first observation. Clinicians should be alert for subtle underlying fracture lines. Emergency medicine physicians should carefully examine cranial dog bite injuries against the possibility of CSF leakage and underlying head fractures, especially in the pediatric population. Cranial CT may reveal underlying subtle fractures. Multidisciplinary approaches play important role in reducing morbidity and mortality.
Conflict of interest statement
The authors report no conflict of interest.
Funding
This study received no extramural funding.
Authors’contributions
A.G., H.T.G., S.O., and S.G. designed, performed literature search,and wrote the manuscript. All authors provided feedback and reviewed the entire article.
 Journal of Acute Disease2022年5期
Journal of Acute Disease2022年5期
- Journal of Acute Disease的其它文章
- Congestive heart failure masquerading as acute abdomen: A case report
- Symmetrical peripheral gangrene triggered by Escherichia coli sepsis
- COVID-19 presentation as acute pancreatitis: A case report
- Effect of pH, lactate, electrolyte, and strong ion difference variability on prediction of intensive care unit mortality: A retrospective study
- Effectiveness of ChAdOx1 nCoV-19 coronavius vaccine in preventing severe disease and mortality during the second wave of pandemic: A case-case analysis from a tertiary care center in South India
- Comparative efficacy of ketamine, lidocaine, acetaminophen, and dexmedetomidine combined with morphine patient-controlled analgesia in treating opium-addicted patients undergoing tibia fracture surgery: A randomized clinical trial