
lmmunotherapy in biliary tract cancers:Current evidence and future perspectives
2022-08-19 05:32:00PedroLuizSerranoUsonJuniorRaphaelLCAraujo
lNTRODUCTlON
More than 905677 new cases of hepatobiliary cancer were estimated worldwide including hepatocellular carcinoma (HCC) in 2020.In addition,more than 115949 new cases of gallbladder cancer (GC) were reported in the same period[1].In the United States,the incidence of patients diagnosed with liver and intra-hepatic tumors was estimated to be 42810 cases in 2020.Additionally,around 11980 patients were diagnosed with gallbladder and other biliary cancers[2,3].The overall survival remains dismal with less than 10% of patients diagnosed with cholangiocarcinoma surviving 5 years after diagnosis[4,5].Biliary tract cancers (BTC) comprise of a set of malignant tumors that can arise from any part of the bile ducts.BTC can be divided in intra-hepatic cholangiocarcinoma (ICC),peri-hilar cholangiocarcinoma,extrahepatic cholangiocarcinoma (EHC) and GC.
In the last few years,several advances have been made in the management of BTC particularly in relation to ICC.Furthermore,the personalized medicine aligned with new molecules have brought about new hope for patients with advanced disease.For patients with tumors harboring isocitrate dehydrogenase 1 (IDH-1) mutations,reported in about 25% of ICC,the IDH-1 mutant inhibitor ivosidenib was evaluated in a randomized phase 3 trial including patients with disease in progress after at least one previous treatment.Ivosidenib delayed progression of the disease compared to placebo[6,7].For tumors harboring fibroblast growth factor receptor 2 (FGFR2) fusions,United States Food and Drug Administration (FDA) has just approved the inhibitor pemigatinib that showed an objective response rate of 36% in a single arm cohort of 107 patients whom disease had progressed from previous chemotherapy treatment and of these patients,3 patients had a complete response[8].Multiple other FGFR inhibitors are under development and new agents will be incorporated into the landscape in the next few years[9,10].
The birth of Tommy, a healthy, beautiful son, was an event for celebration, and as time went by, it seemed as though every day brought another reason to celebrate the gift of Tommy’s life. He was sweet, thoughtful, fun-loving and a joy to be around.
It never entered the fox s head that even foxes can be outwitted, so after a bit he consented to go with her; but he hadn t gone far before the cunning girl seized a stick, and gave him such a blow with it on the head, that he dropped down dead on the spot
Biliary cancers are desmoplastic tumors with an immunoresistant tumor microenvironment[4,11].The liver has a great capacity of immunotolerance related to a continuous exposure to antigens derived from intestinal flora and a large population of macrophages.This microenvironment actively contributes to the limited effect of checkpoint inhibitors in these tumors[4,12].Hepatobiliary cancers have unique characteristics and components related to immune evasion.Tumor-associated macrophages were associated with higher tumor recurrence in a retrospective analysis in a small group of surgically resected hilar cholangiocarcinoma specimens which also showed a worse overall survival[13].However,more precise and comprehensive evaluation of cellular components,including myeloid-derived suppressor cells and natural-killer cells,are necessary to drive conclusions of the impact of targeting to these cells in biliary cancers[4].Immune checkpoint inhibitors (ICI),particularly anti-programmed cell death protein-1/programmed death ligand-1 (PD1/PD-L1) and anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA4) antibodies have shown excellent results in HCC[14,15].For this reason,most of the recent clinical trials in biliary cancers have been conducted with single ICI or combinations[16,17].More recently,durvalumab also was evaluated along with chemotherapy and exhibited exciting results in a randomized phase 3 trial in advanced biliary cancers[18,19].The aim of this review is to cover the main studies of immunotherapy in biliary cancers,biomarkers of efficacy,future combinations and strategies in advanced-stage disease.
TUMOR-AGNOSTlC BlOMARKERS
Microsatellite instability high
Another strategy to enhance anti-PD1/PD-L1 efficacy is combination with CTLA-4 inhibitors.This strategy has proposed that these combinations can enhance the activity and infiltration of cytotoxic T cells in tumor microenvironment in BTC[4].Nivolumab plus ipilimumab was evaluated in a group of 39 metastatic BTC patients included in the CA 209-538 clinical trial for rare cancers.The primary endpoint was clinical benefit rate,exploratory endpoints included correlation of efficacy with biomarkers including PD-L1 expression and TMB.A total of thirty-three patients (85%) received at least one prior line of systemic treatment (0-2 Lines).The ORR was 24% and the clinical benefit rate was 45%.Responses were observed in all subgroups of BTC.The median OS and PFS were 6.1 and 3.1 mo,respectively.The other twenty-two (56%) patients experienced an immune–related adverse event of grade ≥ 3 AE were observed in 8 (20%) patients[40].
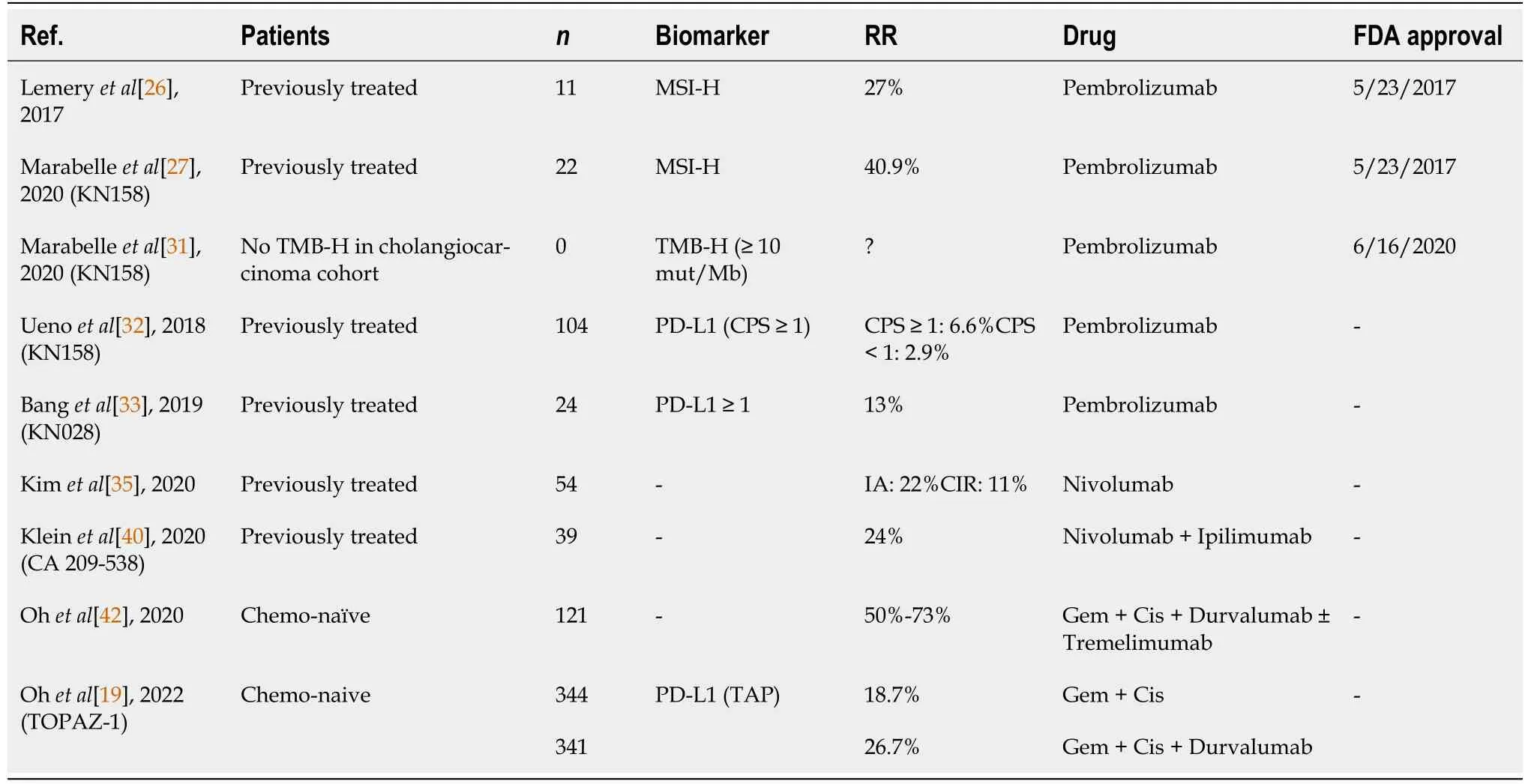
In BTC,the efficacy of pembrolizumab in MSI-H was evaluated in different cohorts.In one study including 11 patients with advanced BTC MSI-H,the response rate (RR) was 27% (3/11) with response duration ranging between 11.6 to 19.6 mo[26].Data from microsatellite instability in high BTC patients treated with the Keynote-158 with pembrolizumab showed better response rates.In a cohort of 22 patients,the objective response rate (ORR) was 40.9% (20.7-63.6) with a complete response in 2 patients.The median progression-free survival (PFS) was 4.2 mo with a median overall survival (OS) of 24.3 mo;however,the median duration of response was not reached[27].A report of 4 BTC MSI-H patients was also included in a cohort of solid tumors treated with pembrolizumab.Of these patients,one had a complete response and the remaining three had stable disease[28].Based on this evidence,immunotherapy should be considered for the treatment of advanced BTC patients with the microsatellite instability high phenotype.All of these studies included patients previously exposed to chemotherapy regimens and evaluation of ICI in previous lines of systemic treatment in MSI-H BTC should be prospectively evaluated.Currently,pembrolizumab is approved by the FDA to treat MSI-H BTC in cases that progressed following prior treatment and those with no satisfactory alternative treatment options.
Tumor mutational burden high
Tumor mutational burden (TMB) is a biomarker that measures and quantifies the total mutation load in tumors.In biliary tract cancers,the TMB was evaluated retrospectively in a group of 156 patients.Of these,133 tumoral tissues were assessed for the TMB with next-generating sequencing.Forty-eight cases were GC,58 were ICC and 50 were EHC.The mean TMB value was high among patients with GC,followed by EHC and ICC [7.1
5.5
3.9 mutations/megabase (muts/Mb),
< 0.05].The proportion of the TMB high (TMB-H),is defined in the study as 9.0 muts/Mb and was higher in GC than in ICC and EHC[29].In another cohort including 803 BTC patients,160 patients were evaluated with wholeexome sequencing and 643 patients with hybrid capture–based comprehensive genomic profiling.The mean TMB was 3.0 (IQR: 0.8-6.1) mut/Mb.In this cohort,4 of 6 patients with MSI-H phenotype had a response to the disease after immunotherapy of the PD1 inhibitor[30].
Returning outside he climbed down the cliff to the stream below. At the bottom there was plenty of water but nothing with which to carry it. Then he spied a chipped cup some knight had tossed from above. Carefully picking it from the sand he filled it as best as he could and climbed back up.
lMMUNE CHECKPOlNT lNHlBlTORS CLlNlCAL TRlALS
Equivalent results were obtained in another single center cohort including 40 patients.In this prospective cohort pembrolizumab was evaluated in advanced PD-L1 ≥ 1% BTC patients who radiologically progressed after receiving first-line gemcitabine plus cisplatin.In the study,47.5% of the patients included had ECOG performance status ≥ 2.The ORR by Response Evaluation Criteria in Solid Tumor(RECIST) v1.1 was 10% and by immune-modified RECIST was 12.5%,and the median OS was 4.3 mo(3.5-5.1).OS did not statistically differ between groups in different biomarker analyses,including CPS or tumor proportion score[34].Anti-PD-1 nivolumab was evaluated in a multi-site phase II study including 54 advanced BTC patients whose disease progressed while undergoing treatment with at least 1 Line but no more than 3 Lines of systemic therapy.Central independent review RR was 11% (5/46),and investigator-assessed (IA) review response rate was 22% (10/46).Among the intention-to-treat population,median PFS was 3.68 mo (2.3-5.69) and median OS was 14.24 mo (5.98 to not reached).In this study,samples with 1% or more tumor cells for PD-L1 and any tumor infiltrating lymphocytes(TILs) for PD-1 exhibiting membranous staining were considered biomarker positive.PD-L1 expression was associated with prolonged PFS (
< 0.001).The PD-1 expression on TILs in this study had no correlation with clinical outcomes[35].Although some responses were seen in these studies,immunotherapy with anti-PD-1 alone in unselected biomarker patients did not show great efficacy.
lMMUNE CHECKPOlNT lNHlBlTORS COMBlNED WlTH CHEMOTHERAPY
Combination of chemotherapy with ICI in BTCs are the subject of study.A phase II study conducted in China evaluated the anti-PD-1 camrelizumab with FOLFOX4 (fluorouracil plus oxaliplatin) in 47 chemotherapy na?ve advanced BTC patients.In 43 patients available for RR analysis,the confirmed response was achieved in 7%,with a disease control rate of 67.4%.Median PFS and OS were not reached.A Grade ≥ 3 AE occurred in 57.4% of the patients,the most commonly occurring AE was hematological count decreases[36].Another study conducted in China evaluated the addition of anti-PD-1 antibodies to nab-paclitaxel and S1 in 32 patients with advanced BTC who were treated with anti-PD-1 inhibitors (pembrolizumab,nivolumab,sintilimab or toripalimab) plus nab-paclitaxel and S1,and in 26 patients who were treated with the combination chemotherapy alone.ORR were higher in the PD-1 inhibitors combination group (25%) compared with chemotherapy alone (15.3%).The median PFS was 5.4 mo in the group treated with anti-PD-1 compared to 2.82 mo in the group with chemotherapy alone (
= 0.01).The median OS is not mature[37].
“Watch it , squirt.” The boy yelled2 as he dodged3 around the little third-grader. Then, with a smirk4 on his face, the boy took hold of his right leg and mimicked5 the way Amy limped6 when she walked.
Based on the results of the TOPAZ-1 trial,upfront combination of chemotherapy with durvalumab could be considered a standard of care however some concerns need to be further evaluated.First,it is clear that based on the curves of overall survival they began to separate around 6 mo.We need to consider that after 6 mo,the control arm is placebo not chemotherapy,the HR was 0.91 for up to 6 mo and 0.74 thereafter.We don’t know if continuing chemotherapy with the same regimen or a maintenance strategy would affect the results of the study.Second,more than half of patients included in the study had intrahepatic cholangiocarcinoma and more than half had a PD-L1 score TAP (tumor are positivity) above 1.It is unclear if the study would have different results with more patients with PD-L1 score 0 or other underrepresented sites including extrahepatic cholangiocarcinoma or gallbladder.Third,in the subgroup analysis it seems that Asian patients derived more benefit from the combination than non-Asian patients.Asian patients comprised half of the patients included in the study.Lastly,no molecular analysis was presented,nether evaluation of underlying liver diseases including viralhepatitis or NASH[19].This question opens up future strategies of research to improve the care and understanding of immunotherapy in advanced biliary cancer patients.
The TOPAZ-1 trial is a randomized phase 3 trial that evaluated the combination of durvalumab,an anti-PD-L1,with chemotherapy against chemotherapy alone in advanced BTC.The study presented at the 2022 ASCO Gastrointestinal Cancers Symposium met its primary endpoint by improving OS in this subgroup of patients.Median OS was 12.8 mo with the combination
11.6 mo with gemcitabine and cisplatin alone (HR 0.8,
= 0.021).Furthermore,the addition of durvalumab to gemcitabine and cisplatin also improved PFS,7.2 mo
5.7 mo (HR 0.75,
= 0.001) and tumor responses,26.7%
18.7%[19].
lMMUNE CHECKPOlNT lNHlBlTORS COMBlNATlONS
Microsatellite-instability is a phenotype presented in cells with defective mismatch repair genes that result in a hypermutation state and the prevalence of microsatellite instability is high (MSI-H) in biliary tract cancers (BTC) ranging between 5%-10%[20].The MSI-H phenotype can be a germline (Lynch syndrome) or somatic[21,22].Multiples studies have evaluated the effect of ICI in patients harboring MSI-H tumors.Recently,a randomized phase III trial demonstrated better outcomes in MSI-H metastatic colorectal cancer treated with upfront front-line therapy with pembrolizumab compared with the standard chemotherapy regimen[23].Pembrolizumab is an anti PD-1 antibody.PD-1 is a cell surface protein presented in most activated T cells.When PD-L1 bound to the PD-1,this binding facilitates apoptosis and dysfunction of activated T cells and mediates an immune suppressive microenvironment[24,25].Therefore,binding PD-1 with an antibody may promote functional enhancement of activated T cells repairing anti-tumor immunity[24].
As the sun rose over the horizon, I went out to enjoy the beauty of the grassland1 scenery,. On the way, I saw a pair of red flowers blooming. They had flat petals2 and were incredibly full of smiling beauty. Those independent flowers seemed very vibrant. Gazing at the flowers made me think of many things.
When Roger Maris came to the New York Yankees from the Kansas City Athletics1 in 1960, I was eleven. I had been burned in a fire in August, so I was laid up for a while and followed baseball even more closely. I remember a headline that said Roger Maris rejuvenates2 the Yankees. I had never heard the word before, but it made me think this Roger Maris was someone special.
The combination was further evaluated in a multi-institutional phase 2 trial with patients who had advanced BTC but without previous systemic therapy.Patients were distributed into two groups of treatment,the arm A was treated with gemcitabine,cisplatin and nivolumab and patients received this combination every 3 wk for 6 mo,followed by nivolumab monotherapy that patients received every 2 wk for a total duration of 2 years.The arm B consisted of nivolumab given for patients every 2 wk and ipilimumab every 6 wk for 2 years in case of no disease progression.The primary endpoint was a PFS rate at 6 mo,and of all the patients,35 were treated in arm A and 36 patients treated in arm B.Progression-free survival rate at 6 mo was 70% in arm A and 18.6% in arm B.In addition,the observed PFS rates at 6 mo were insufficient to reject the null hypothesis in both arms[41].
In another phase II study,combination of durvalumab,an anti-PD-L1 antibody,with tremelimumab,an anti-CTLA-4 antibody,with chemotherapy were evaluated in 121 chemotherapy na?ve metastatic BTC patients[42].In this study,patients were allocated in three groups of treatment.The first group,biomarker cohort (BMC) in which thirty patients were treated with cisplatin and gemcitabine for one cycle,following the next cycles with gemcitabine plus cisplatin,and durvalumab plus tremelimumab every 3 wk until the disease progression.The second group,three combo cohort (3C),a total of 45 patients were treated with gemcitabine,cisplatin and durvalumab.The latter group,in the four-combo cohort (4C) including 46 patients,were treated with all the four drugs,chemotherapy with gemcitabine and cisplatin plus durvalumab and tremelimumab until disease progression or unacceptable toxicity.Overall,the addition of immunotherapy associated with chemotherapy on the first-line therapy was well tolerated and demonstrated to be a promising activity.The ORR was 50% (32.1-67.9) in the BMC group,73.4% (60.5-86.3) in the 3C group and 73.3% (60.4-86.2) in the 4C group.In addition,the DCR ranged between 96.7%-100%.The median PFS was 13 mo in the BMC group,11 mo in the 3C group and 11.9 mo in the 4C group.Median OS in the 4C group was 20.7 mo,18.1 mo in the 3C group,and 15 mo in the BMC group.PD-L1 analysis before treatment did not show any association with PFS or OS.Interestingly,in the BMC group,a trend in higher PFS was observed after gemcitabine and cisplatin first cycle,in patients whose tumor had high expression of PD-L1 compared with patients with lower PD-L1.The main studies described are included on Table 1.
lMMUNE CHECKPOlNT lNHlBlTORS COMBlNED WlTH ANTlANGlOGENlCS
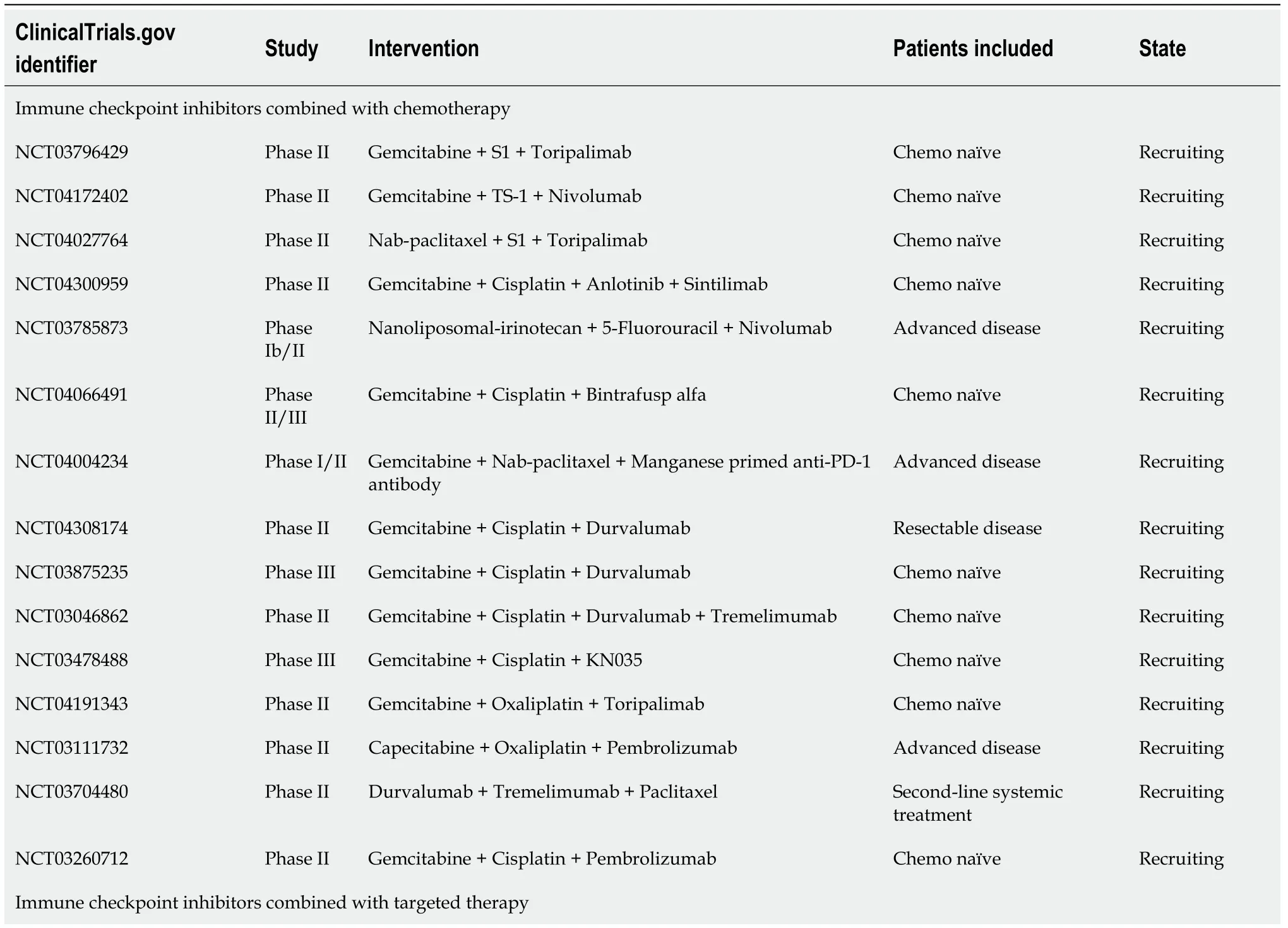
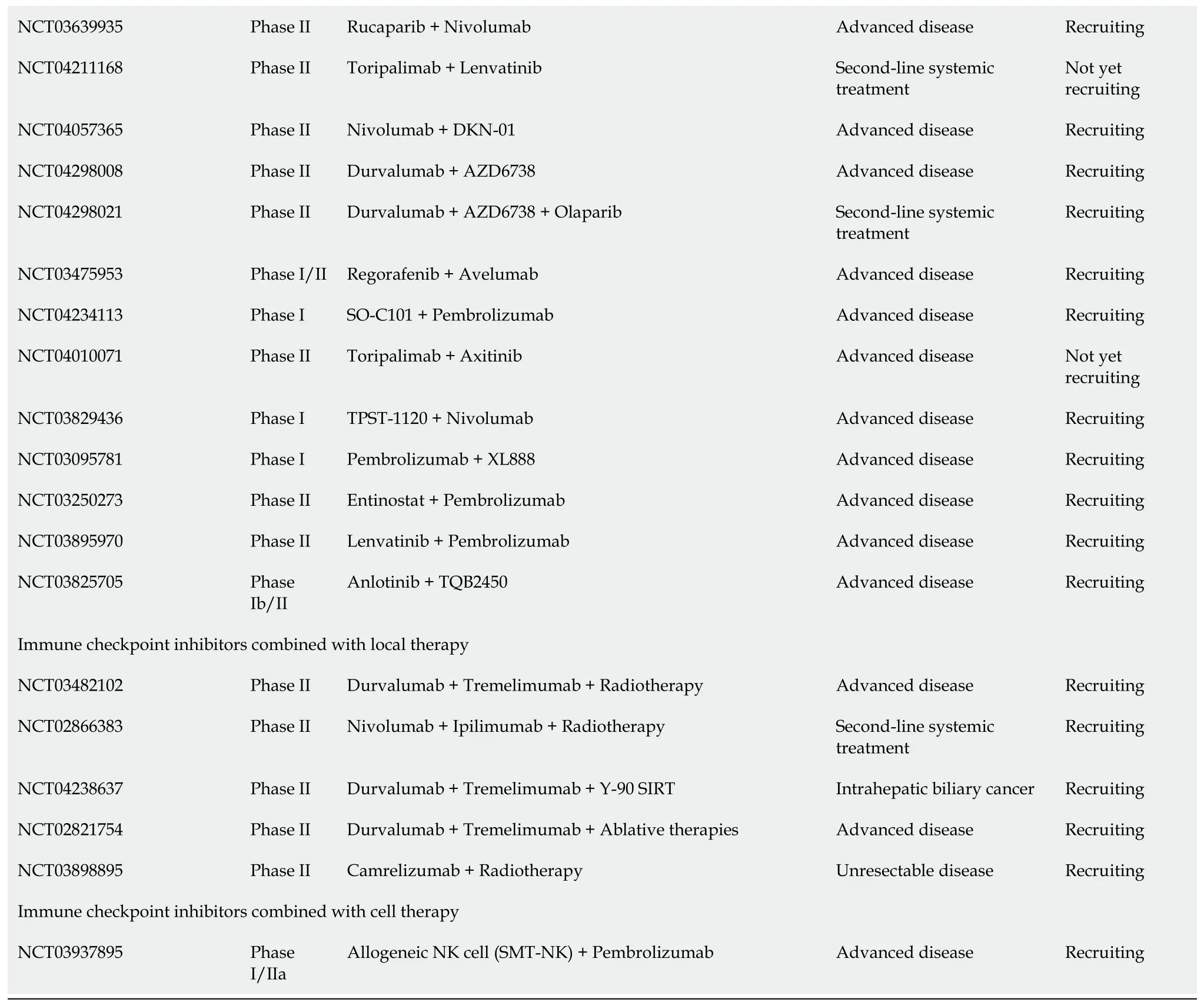
Most of the recruiting studies in advanced BTC tend to combine ICI with chemotherapy in first-line systemic treatment or later lines.This combination has additional effects in enhancing ICI efficacy,as previously discussed[40,19].Local ablative therapies and liver directed therapies are also strategies focused in enhancing neoantigens presentation and/or developing abscopal effect[45,46].The main ongoing recruiting studies with different strategies and combinations with ICI are summarized in Table 2.In October 2021,interim analysis of the randomized phase III study TOPAZ-1,evaluated cisplatin,gemcitabine and durvalumab,against standard-of-care chemotherapy,and demonstrated a significant OS benefit as a 1st-line treatment for patients with advanced biliary tract cancer[47].Recently,a final report confirmed that the addition of durvalumab to cisplatin and gemcitabine improved progression-free survival and overall survival compared to chemotherapy alone with no safety concerns.
FUTURE DlRECTlONS
Combination with antiangiogenics can enhance the immunotherapy effect,contributing to cytotoxic effect of lymphocytes on the tumor microenvironment.After promising results in HCC,studies combining these agents are another option for refractory patients.In a non-randomized phase II study,31 patients with chemotherapy refractory BTC were treated with Lenvatinib,a tyrosine kinase inhibitor(TKI) with antiangiogenics properties,associated with pembrolizumab[43].The combination showed an ORR of 10% (2-26).These patients had a median PFS of 6.1 mo and a median OS of 8.6 mo.The most frequent treatment-related AEs,as expected,included hypertension and immune mediated adverse events[43].Similar results were observed with the combination of regorafenib,another TKI,with anti-PD-L1 avelumab[44].In this phase II study,34 heavily pretreated patients with advanced BTC were treated.Four (13.8%) achieved partial response.Hypertension and fatigue were the most common grade 3/4 AE.
Multiple mechanisms related to the synergism between chemotherapy and immunotherapy have been established.Chemotherapy can induce PD-L1 expression in cancer cells,facilitates infiltration of cytotoxic T cells in the tumor microenvironment and increases neoantigens and antigen-presenting cells.All of these effects can enhance the PD-1 inhibition[38].Further evaluation of this synergism,preliminary safety and efficacy results of toripalimab and gemcitabine plus S-1 were presented[39].In this phase II study,34 patients were treated with the combination.Overall RR was 20.6% with a disease control rate (DCR) of 85.3%.In this study,patients with a mutation on TP53 or ATM had shorter PFS than the wild type[39].
47. Fattened so slowly: Trickery is one of the most popular methods for dealing115 with the evil in fairy tales. This implies that the trickster has experienced and accepted evil within him or her self, allowing insight into the strategy of the adversary116 (Jacoby 1992).Return to place in story.
As to the Gray Wolf, he spent one day, he spent two days, he spent three days in Tsar Afron s Palace, all the while having the shape of the beautiful Tsarevna, while the Tsar made preparations for a splendid bridal. On the fourth day he asked the Tsar s permission to go for a walk on the open steppe.
In Keynote-158,a phase II basket study of pembrolizumab monotherapy for patients with advanced solid tumors,the relationship between activity of pembrolizumab and TMB was an exploratory endpoint.TMB-H was considered ≥ 10 mut/Mb.In the study,790 patients had evaluable TMB included for efficacy analysis and 102 patients (13%) were TMB-H.The ORR observed was 29% (21-39) for TMBH and 6% (5-8) for TMB-low.In addition,median duration of response in months was not reached for TMB-H and was 33 mo in TMB-low.The median OS for TMB-H and low was 11.7 mo (9.1-19.1) and 12.8 mo (11.1-14.1),respectively[31].Based on these results,on June 16
,2020,the FDA approved pembrolizumab for the treatment of adult and pediatric patients with unresectable or metastatic TMB-H (≥ 10 mut/Mb) solid tumors that showed progression following the prior treatment and for those who have no satisfactory alternative treatment options.Despite being an important approval and option in the management of patients with advanced BTC,no BTC patients were evaluated in the TMB-H cohort.With the approval and clinical utilization in practice,future cohorts will bring insights about response rate and efficacy for this group of patients.
CONCLUSlON
Immune checkpoint agnostic approvals for advanced-stage cancer with biomarkers such as MSI-H and TMB-H are important treatment options for patients with advanced BTC who currently have limited options for treatment of refractory disease.Drug combinations such as anti-PD-1/PD-L1 with anti-CTLA-4 and/or chemotherapy have the potential to establish the standard of care for these patients and benefit a larger proportion of individuals if adopted in earlier lines of systemic treatment,however,more studies are necessary to better identify subgroups of patients that will most benefit from these strategies and treatments.
ICI were first evaluated in metastatic BTC patients whose disease had progressed on chemotherapy and the pembrolizumab was evaluated in two cohorts[32,33].In the Keynote-028 PD-L1–positivity(membranous PD-L1 expression in ≥ 1% of tumor and associated inflammatory cells or positive staining in stroma) was required for eligibility and at the median follow-up time of 6.5 mo,the ORR was 13% in 23 patients.The median OS was 6.2 mo (3.8-10.3) with a 12-mo OS rate of 27.6%.The grade ≥ 3 adverse events (AE) occurred in 16.7% of the patients[33].In the Keynote-158,a total of 104 patients with advanced BTC whose disease progressed on any lines of systemic treatment were treated with pembrolizumab.In that study,PD-L1 positivity was not mandatory and 61 patients had PD-L1 combined positive scores (CPS) ≥ 1.The overall RR was 5.8% (2.1-12.1) with six partial responses.Among patients with tumors with PD-L1 CPS ≥ 1 (
= 61) the ORR was 6.6% (1.8-15.9) and in patients with tumors with PD-L1 CPS < 1 (
= 34),the ORR was 2.9% (0.1-15.3).The median OS was compared in patients with PDL1 CPS ≥ 1
< 1,7.2 mo (5.3-11.0)
9.6 mo (5.4-12.8),respectively.Overall,13% of patients had a Grade ≥ 3 AE[32].
Araujo RLC and Uson Junior PLS performed the literature review,collected all the data and wrote the manuscript; All authors have read and approved the final manuscript.
All the authors report no relevant conflicts of interest for this article.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Brazil
Pedro Luiz Serrano Uson Junior 0000-0001-6122-1374; Raphael LC Araujo 0000-0002-7834-5944.
Gong ZM
Filipodia
Gong ZM
1 Sung H,Ferlay J,Siegel RL,Laversanne M,Soerjomataram I,Jemal A,Bray F.Global Cancer Statistics 2020:GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries.
2021;71: 209-249 [PMID: 33538338 DOI: 10.3322/caac.21660]
2 NCCN.Hepatobiliary Cancers,NCCN guidelines version 2.2021.[Accessed 1 May 2021] Available from:https://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf
3 Siegel RL,Miller KD,Jemal A.Cancer statistics,2020.
2020; 70: 7-30 [PMID: 31912902 DOI:10.3322/caac.21590]
4 Arora M,Bogenberger JM,Abdelrahman A,Leiting JL,Chen X,Egan JB,Kasimsetty A,Lenkiewicz E,Malasi S,Uson PLS,Nagalo BM,Zhou Y,Salomao MA,Kosiorek HE,Braggio E,Barrett MT,Truty MJ,Borad MJ.Evaluation of NUC-1031: a first-in-class ProTide in biliary tract cancer.
2020; 85: 1063-1078 [PMID: 32440762 DOI: 10.1007/s00280-020-04079-z]
5 Uson Junior PLS,Bogenberger J,Borad MJ.Advances in the treatment of biliary tract cancers.
2020; 36: 85-89 [PMID: 31972599 DOI: 10.1097/MOG.0000000000000606]
6 Lowery MA,Abou-Alfa GK,Burris HA,Janku F,Shroff RT,Cleary GM,Azad NS,Goyal L,Maher EA,Gore L,Hollebecque A,Beeram M,Trent JC,Jiang L,Ishii Y,Auer J,Gliser C,Agresta SV,Pandya SS,Zhu A.Phase 1 study of AG-120,an IDH1 mutant enzyme inhibitor: results from the cholangiocarcinoma dose escalation and expansion cohorts.
2017; 35: 4015 [DOI: 10.1200/JCO.2017.35.15_suppl.4015]
7 Abou-Alfa GK,Macarulla T,Javle MM,Kelley RK,Lubner SJ,Adeva J,Cleary JM,Catenacci DV,Borad MJ,Bridgewater J,Harris WP,Murphy AG,Oh DY,Whisenant J,Lowery MA,Goyal L,Shroff RT,El-Khoueiry AB,Fan B,Wu B,Chamberlain CX,Jiang L,Gliser C,Pandya SS,Valle JW,Zhu AX.Ivosidenib in IDH1-mutant,chemotherapyrefractory cholangiocarcinoma (ClarIDHy): a multicentre,randomised,double-blind,placebo-controlled,phase 3 study.
2020; 21: 796-807 [PMID: 32416072 DOI: 10.1016/S1470-2045(20)30157-1]
8 Abou-Alfa GK,Sahai V,Hollebecque A,Vaccaro G,Melisi D,Al-Rajabi R,Paulson AS,Borad MJ,Gallinson D,Murphy AG,Oh DY,Dotan E,Catenacci DV,Van Cutsem E,Ji T,Lihou CF,Zhen H,Féliz L,Vogel A.Pemigatinib for previously treated,locally advanced or metastatic cholangiocarcinoma: a multicentre,open-label,phase 2 study.
2020;21: 671-684 [PMID: 32203698 DOI: 10.1016/S1470-2045(20)30109-1]
9 Ahn DH,Uson Junior PLS,Masci P,Kosiorek H,Halfdanarson TR,Mody K,Babiker H,DeLeon T,Sonbol MB,Gores G,Smoot R,Bekaii-Saab T,Mahipal A,Mansfield A,Tran NH,Hubbard JM,Borad MJ.A pilot study of Pan-FGFR inhibitor ponatinib in patients with FGFR-altered advanced cholangiocarcinoma.
2022; 40: 134-141 [PMID:34463891 DOI: 10.1007/s10637-021-01170-x]
10 Zugman M,Botrus G,Pestana RC,Uson Junior PLS.Precision Medicine Targeting
Genomic Alterations in Advanced Cholangiocarcinoma: Current State and Future Perspectives.
2022; 12: 860453 [PMID: 35444941 DOI: 10.3389/fonc.2022.860453]
11 Razumilava N,Gores GJ.Cholangiocarcinoma.
2014; 383: 2168-2179 [PMID: 24581682 DOI:10.1016/S0140-6736(13)61903-0]
12 Havel JJ,Chowell D,Chan TA.The evolving landscape of biomarkers for checkpoint inhibitor immunotherapy.
2019; 19: 133-150 [PMID: 30755690 DOI: 10.1038/s41568-019-0116-x]
13 Atanasov G,Hau HM,Dietel C,Benzing C,Krenzien F,Brandl A,Wiltberger G,Matia I,Prager I,Schierle K,Robson SC,Reutzel-Selke A,Pratschke J,Schmelzle M,Jonas S.Prognostic significance of macrophage invasion in hilar cholangiocarcinoma.
2015; 15: 790 [PMID: 26497197 DOI: 10.1186/s12885-015-1795-7]
14 Finn RS,Qin S,Ikeda M,Galle PR,Ducreux M,Kim TY,Kudo M,Breder V,Merle P,Kaseb AO,Li D,Verret W,Xu DZ,Hernandez S,Liu J,Huang C,Mulla S,Wang Y,Lim HY,Zhu AX,Cheng AL; IMbrave150 Investigators.Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma.
2020; 382: 1894-1905 [PMID:32402160 DOI: 10.1056/NEJMoa1915745]
15 Yau T,Kang YK,Kim TY,El-Khoueiry AB,Santoro A,Sangro B,Melero I,Kudo M,Hou MM,Matilla A,Tovoli F,Knox JJ,He AR,El-Rayes BF,Acosta-Rivera M,Neely J,Shen Y,Baccan C,Dela Cruz CM,Hsu C.Nivolumab (NIVO) +ipilimumab (IPI) combination therapy in patients (pts) with advanced hepatocellular carcinoma (aHCC): Results from CheckMate 040.
2019; 37: 4012-4012 [DOI: 10.1200/JCO.2019.37.15_suppl.4012]
16 Rizzo A,Ricci AD,Brandi G.Recent advances of immunotherapy for biliary tract cancer.
2021; 15: 527-536 [PMID: 33215952 DOI: 10.1080/17474124.2021.1853527]
17 Ricci AD,Rizzo A,Brandi G.Immunotherapy in Biliary Tract Cancer: Worthy of a Second Look.
2020;27: 1073274820948047 [PMID: 32806956 DOI: 10.1177/1073274820948047]
18 Rizzo A,Ricci AD,Brandi G.Durvalumab: an investigational anti-PD-L1 antibody for the treatment of biliary tract cancer.
2021; 30: 343-350 [PMID: 33645367 DOI: 10.1080/13543784.2021.1897102]
19 Oh DY,He AR,Qin S,Chen LT,Okusaka T,Vogel A,Kim JW,Suksombooncharoen T,Lee MA,Kitano M,Burris III HA,Bouattour M,Tanasanvimon S,Zaucha R,Avallone A,Cundom J,Rokutanda N,Xiong J,Cohen G,Valle JW.A phase 3 randomized,double-blind,placebo-controlled study of durvalumab in combination with gemcitabine plus cisplatin(GemCis) in patients (pts) with advanced biliary tract cancer (BTC): TOPAZ-1.
2022; 40: 378 [DOI:10.1200/JCO.2022.40.4_suppl.378]
20 Silva VW,Askan G,Daniel TD,Lowery M,Klimstra DS,Abou-Alfa GK,Shia J.Biliary carcinomas: pathology and the role of DNA mismatch repair deficiency.
2016; 5: 62 [PMID: 27829276 DOI: 10.21037/cco.2016.10.04]
21 Cortes-Ciriano I,Lee S,Park WY,Kim TM,Park PJ.A molecular portrait of microsatellite instability across multiple cancers.
2017; 8: 15180 [PMID: 28585546 DOI: 10.1038/ncomms15180]
22 Bogenberger JM,DeLeon TT,Arora M,Ahn DH,Borad MJ.Emerging role of precision medicine in biliary tract cancers.
2018; 2: 21 [PMID: 30302397 DOI: 10.1038/s41698-018-0064-z]
23 André T,Shiu KK,Kim TW,Jensen BV,Jensen LH,Punt C,Smith D,Garcia-Carbonero R,Benavides M,Gibbs P,de la Fouchardiere C,Rivera F,Elez E,Bendell J,Le DT,Yoshino T,Van Cutsem E,Yang P,Farooqui MZH,Marinello P,Diaz LA Jr; KEYNOTE-177 Investigators.Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer.
2020; 383: 2207-2218 [PMID: 33264544 DOI: 10.1056/NEJMoa2017699]
24 Chen L,Han X.Anti-PD-1/PD-L1 therapy of human cancer: past,present,and future.
2015; 125: 3384-3391[PMID: 26325035 DOI: 10.1172/JCI80011]
25 Oliveira AF,Bretes L,Furtado I.Review of PD-1/PD-L1 Inhibitors in Metastatic dMMR/MSI-H Colorectal Cancer.
2019; 9: 396 [PMID: 31139574 DOI: 10.3389/fonc.2019.00396]
26 Lemery S,Keegan P,Pazdur R.First FDA Approval Agnostic of Cancer Site - When a Biomarker Defines the Indication.
2017; 377: 1409-1412 [PMID: 29020592 DOI: 10.1056/NEJMp1709968]
27 Marabelle A,Le DT,Ascierto PA,Di Giacomo AM,De Jesus-Acosta A,Delord JP,Geva R,Gottfried M,Penel N,Hansen AR,Piha-Paul SA,Doi T,Gao B,Chung HC,Lopez-Martin J,Bang YJ,Frommer RS,Shah M,Ghori R,Joe AK,Pruitt SK,Diaz LA Jr.Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results From the Phase II KEYNOTE-158 Study.
2020; 38: 1-10 [PMID: 31682550 DOI: 10.3410/f.736855157.793571317]
28 Le DT,Durham JN,Smith KN,Wang H,Bartlett BR,Aulakh LK,Lu S,Kemberling H,Wilt C,Luber BS,Wong F,Azad NS,Rucki AA,Laheru D,Donehower R,Zaheer A,Fisher GA,Crocenzi TS,Lee JJ,Greten TF,Duffy AG,Ciombor KK,Eyring AD,Lam BH,Joe A,Kang SP,Holdhoff M,Danilova L,Cope L,Meyer C,Zhou S,Goldberg RM,Armstrong DK,Bever KM,Fader AN,Taube J,Housseau F,Spetzler D,Xiao N,Pardoll DM,Papadopoulos N,Kinzler KW,Eshleman JR,Vogelstein B,Anders RA,Diaz LA Jr.Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade.
2017; 357: 409-413 [PMID: 28596308 DOI: 10.1126/science.aan6733]
29 Yi B,Liu L,Song J,Huang Y,Zhang M,Chen R,Xia X,Jiang X.Mutational landscape and tumor mutation burden (TMB)feature of biliary cancer.
2020; 38: e16670 [DOI: 10.1200/JCO.2020.38.15_suppl.e16670]
30 Lin J,Yang X,Cao Y,Li G,Zhao S,Shi J,Pan J,Hu K,Zhao L,Guan M,Sang X,Javle MM,Wang K,Wang X,Zhao HT.Genomics and translational precision oncology for 803 patients with biliary tract cancer.
2020; 38: 4589[DOI: 10.1200/JCO.2020.38.15_suppl.4589]
31 Marabelle A,Fakih M,Lopez J,Shah M,Shapira-Frommer R,Nakagawa K,Chung HC,Kindler HL,Lopez-Martin JA,Miller WH Jr,Italiano A,Kao S,Piha-Paul SA,Delord JP,McWilliams RR,Fabrizio DA,Aurora-Garg D,Xu L,Jin F,Norwood K,Bang YJ.Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort,open-label,phase 2 KEYNOTE-158 study.
2020; 21: 1353-1365 [PMID: 32919526 DOI: 10.1016/S1470-2045(20)30445-9]
32 Ueno M,Chung HC,Nagrial A,Marabelle A,Kelley RK,Xu L,Mahoney J,Pruitt SK,Oh DY.625PD Pembrolizumab for advanced biliary adenocarcinoma: Results from the multicohort,phase II KEYNOTE-158 study.
2018; 29:mdy282-009 [DOI: 10.1093/annonc/mdy282.009]
33 Bang YJ,Ueno M,Malka D,Chung HC,Nagrial A,Kelley RK,Piha-Paul SA,Ros W,Italiano A,Nakagawa K,Rugo HS,De Braud FG,Varga AI,Hansen AR,Gao C,Krishnan S,Norwood K,Doi T.Pembrolizumab (pembro) for advanced biliary adenocarcinoma: Results from the KEYNOTE-028 (KN028) and KEYNOTE-158 (KN158) basket studies.
2019; 37: 4079 [DOI: 10.1200/JCO.2019.37.15_suppl.4079]
34 Kang J,Jeong JH,Hwang HS,Lee SS,Park DH,Oh DW,Song TJ,Kim KH,Hwang S,Hwang DW,Kim SC,Park JH,Hong SM,Kim KP,Ryoo BY,Yoo C.Efficacy and Safety of Pembrolizumab in Patients with Refractory Advanced Biliary Tract Cancer: Tumor Proportion Score as a Potential Biomarker for Response.
2020; 52: 594-603 [PMID:32019287 DOI: 10.4143/crt.2019.493]
35 Kim RD,Chung V,Alese OB,El-Rayes BF,Li D,Al-Toubah TE,Schell MJ,Zhou JM,Mahipal A,Kim BH,Kim DW.A Phase 2 Multi-institutional Study of Nivolumab for Patients With Advanced Refractory Biliary Tract Cancer.
2020; 6: 888-894 [PMID: 32352498 DOI: 10.1001/jamaoncol.2020.0930]
36 Qin S,Chen Z,Liu Y,Xiong J,Ren Z,Meng Z,Gu S,Wang L,Zou J.A phase II study of anti-PD-1 antibody camrelizumab plus FOLFOX4 or GEMOX systemic chemotherapy as first-line therapy for advanced hepatocellular carcinoma or biliary tract cancer.
2019; 37: 4074 [DOI: 10.1200/JCO.2019.37.15_suppl.4074]
37 Gou M,Liu TE,Yan H,Si H,Wang Z,Qian N,Dai G.Pd-1 inhibitors plus nab-paclitaxel with S1 (AS) as first line in patients with advanced biliary tract cancer.
2020; 38: e15195 [DOI: 10.1200/JCO.2020.38.15_suppl.e15195]
38 Bailly C,Thuru X,Quesnel B.Combined cytotoxic chemotherapy and immunotherapy of cancer: modern times.
2020; 2: zcaa002 [PMID: 34316682 DOI: 10.1093/narcan/zcaa002]
39 Liu T,Li W,Yu Y,Guo X,Xu X,Wang Y,Li Q,Cui Y,Liu H,Zhang S,Wang F,Yao M,Zhang L.53P Toripalimab with chemotherapy as first-line treatment for advanced biliary tract tumors: A preliminary analysis of safety and efficacy of an open-label phase II clinical study.
2020; 31: S261 [DOI: 10.1016/j.annonc.2020.08.031]
40 Klein O,Kee D,Nagrial A,Markman B,Underhill C,Michael M,Lum C,Behren A,Palmer J,Tebbutt N,Carlino M,Cebon J.Combination immunotherapy with ipilimumab and nivolumab in patients with advanced biliary tract cancers.
2020; 38: 4588 [DOI: 10.1200/JCO.2020.38.15_suppl.4588]
41 Sahai V,Griffith KA,Beg MS,Shaib WL,Mahalingam D,Zhen DB,Deming DA,Dey S,Mendiratta-Lala M,Zalupski M.A multicenter randomized phase II study of nivolumab in combination with gemcitabine/cisplatin or ipilimumab as firstline therapy for patients with advanced unresectable biliary tract cancer (BilT-01).
2020; 38: 4582 [DOI:10.1200/JCO.2020.38.15_suppl.4582]
42 Oh DY,Lee KH,Lee DW,Kim TY,Bang JH,Nam AR,Lee Y,Zhang Q,Rebelatto M,Li W,Kim JW.Phase II study assessing tolerability,efficacy,and biomarkers for durvalumab (D)±tremelimumab (T) and gemcitabine/cisplatin (GemCis)in chemo-na?ve advanced biliary tract cancer (aBTC).
2020; 38: 4520 [DOI:10.1200/JCO.2020.38.15_suppl.4520]
43 Villanueva L,Lwin Z,Chung HC,Gomez-Roca C,Longo F,Yanez E,Senellart H,Doherty M,García-Corbacho J,Hendifar AE,Maurice-Dror C,Gill SS,Kim TW,Heudobler D,Penel N,Ghori R,Kubiak P,Jin F,Norwood KG,Graham D.Lenvatinib plus pembrolizumab for patients with previously treated biliary tract cancers in the multicohort phase II LEAP-005 study.
2021; 39: 321 [DOI: 10.1200/JCO.2021.39.3_suppl.321]
44 Cousin S,Bellera CA,Guégan JP,Mazard T,Gomez-Roca CA,Metges JP,Cantarel C,Adenis A,Korakis I,Poureau P,Spalato-Ceruso M,Bourcier K,Kind M,Soubeyran I,Bessede A,Italiano A.Regomune: A phase II study of regorafenib+avelumab in solid tumors-Results of the biliary tract cancer (BTC) cohort.
2021; 39: 4096 [DOI:10.1200/JCO.2021.39.15_suppl.4096]
45 Shi L,Chen L,Wu C,Zhu Y,Xu B,Zheng X,Sun M,Wen W,Dai X,Yang M,Lv Q,Lu B,Jiang J.PD-1 Blockade Boosts Radiofrequency Ablation-Elicited Adaptive Immune Responses against Tumor.
2016; 22: 1173-1184 [PMID: 26933175 DOI: 10.1158/1078-0432.CCR-15-1352]
46 Wehrenberg-Klee E,Goyal L,Dugan M,Zhu AX,Ganguli S.Y-90 Radioembolization Combined with a PD-1 Inhibitor for Advanced Hepatocellular Carcinoma.
2018; 41: 1799-1802 [PMID: 29845347 DOI:10.1007/s00270-018-1993-1]
47 AstraZeneca.Imfinzi plus chemotherapy significantly improved overall survival in 1st-line advanced biliary tract cancer in TOPAZ-1 Phase III trial at interim analysis.2021.[Accessed on November 23,2021] Available from:https://www.astrazeneca.com/media-centre/press-releases/2021/imfinzi-improved-survival-in-biliary-tract-cancer.html
 World Journal of Gastrointestinal Oncology2022年8期
World Journal of Gastrointestinal Oncology2022年8期
- World Journal of Gastrointestinal Oncology的其它文章
- Colitis and colorectal tumors should be further explored and differentiated
- Exosomes:Promising biomarkers and targets for cancer
- Acute or chronic inflammation role in gastrointestinal oncology
- Ewing sarcoma of the ileum with wide multiorgan metastases:A case report and review of literature
- RASSF1A methylation as a biomarker for detection of colorectal cancer and hepatocellular carcinoma
- Evaluation of the diagnostic value of serum-based proteomics for colorectal cancer