
Ewing sarcoma of the ileum with wide multiorgan metastases:A case report and review of literature
2022-08-19 05:32:22AiWenGuoYiShaLiuHangLiYiYuanSiXunLi
lNTRODUCTlON
Ewing sarcoma (ES) of the bone represents the second most common primary malignant tumor of bone in children and adolescents,exceeded in prevalence only by osteosarcoma[1].Osseous ES,together with extraosseous Ewing’s sarcoma (EOES),primitive neuroectodermal tumor,and Askin’s tumor are members of the Ewing sarcoma family of tumors[1,2].The treatment of EOES patients includes chemotherapy,radiation therapy,and surgery.To date,the 5-year survival rate of EOES is relatively high (65%-75%)[3].The outcome for metastatic patients is usually poor (< 30%),despite the use of surgery,chemo- and/or radiotherapy.EOES is rarer than ES of the bone.The prevalence of EOES is generally accepted to be between 15% and 20% of that of ES of the bone[2].The most common sites of EOES are the paravertebral region,lower extremities,chest wall and retroperitoneum[4].To our knowledge,EOES originating in the ileum is not common,with only nearly 30 cases reported worldwide.However,there were few reports regarding EOES of the ileum with multiorgan metastases at the time of diagnosis[5-7].In this paper,we present a case with an initial diagnosis of gastrointestinal stromal tumor (GIST),but histopathology indicated EOES with widespread multiorgan metastases.
CASE PRESENTATlON
Chief complaints
A 53-year-old man suffered from right lower quadrant abdominal pain for 2 wk.
While I was touched by the boy s persistence5, I was equally touched by the manner in which he ran. With each attempt, he looked so confident...so natural. No signs of fear, nervousness, or of being discouraged — as if he didn t give a care about the world around him.
History of present illness
The patient experienced right lower quadrant abdominal pain for 2 wk,accompanied by acid reflux,belching,and emesis (an oral discharge without digested food and hematemesis),but denied having fevers,night sweats,unintentional weight loss,and blood in the stool.
History of past illness
The patient had a medical history free of previous diseases.
61.Forgave them:Although Cinderella rarely metes98 out punishment upon her sisters in most versions of the tale, other forces often punish her stepfamily for her. In the Grimm s Aschenputtel, birds come and peck out their eyes when they attend Cinderella s church wedding. Return to place in story.
Personal and family history
The patient denied that the family had any genetic diseases.There was no similar disease in the family.
Physical examination
On physical examination,the patient’s abdomen was soft with tenderness on the right side abdominal without rebound tenderness or muscle guarding,and normal bowel sounds were present.In palpation,a mass with unclear boundary was identified in the right lower abdomen,measuring 4 cm × 6 cm approximately,and the mass can be mobile.
Laboratory examinations
After admission,laboratory investigations showed slightly increased levels of monocytes (0.987 × 10
/L;normal range: 0.10–0.60 × 10
/L),decreased eosinophil rate (0.1%; normal range: 0.4%-8%),decreased hemoglobin levels (119 g/L; normal range: 130-175 g/L),and prealbumin levels (14.9 mg/dL; normal range: 16-45 mg/dL),and increased platelet count (418 × 10
/L; normal range: 85-303 × 10
/L).All serum tumor marker levels were normal.
The youngest, however, said, Dear father, that must be a good man to have helped you out of your trouble, so if you have promised him a bride for doing it, your promise must be kept
Imaging examinations
The imaging characteristics of the small intestinal ES are nonspecific as well.The major differential diagnosis for small intestinal ES includes GIST,lymphoma,adenocarcinoma,neuroendocrine neoplasm and metastatic lesions.GISTs are the most common mesenchymal tumors in the gastrointestinal tract and typically present as submucosal tumors of the gastrointestinal wall,occasionally accompanied by mucosal ulcers and tumor rupture[33].GISTs occurring in the small intestinal characteristically have hemorrhage,necrosis,or cyst formation that appears as focal areas of low attenuation on computed tomographic images,and may present with cavity and fistula formation[34].Moreover,GISTs rarely exhibit regional lymph node metastasis,unlike the mass presenting with multiple regional lymph node metastases in our patient.Intestinal lymphoma classically presents with a thickened wall and paradoxical dilatation but no obstruction,potentially with lymphadenopathy,splenomegaly[35].And it often shows mild enhancement and the presence of vessel floating signs.In addition,lymphoma rarely presents with multiorgan metastases[36].Intestinal adenocarcinoma typically shows irregular or annular thickening of the intestinal wall resulting in luminal narrowing,which may result in intestinal obstruction.Small intestinal neuroendocrine neoplasms may have mural transgression with the invasion of the serosa and mesentery and may conglomerate into spiculated masses with frequent calcification and surrounding lymphadenopathy[37,38].Tumor metastasis to the small intestine is extremely rare,and few reports indicate in the literature[39].
MULTlDlSClPLlNARY EXPERT CONSULTATlON
All authors report no relevant conflict of interest for this article.
FlNAL DlAGNOSlS
ES most commonly arises from bone but can develop in extraskeletal sites.In contrast,half or more of primary adult cases are EOES[4].ES exhibits the highest incidence in older adolescents,with patients aged over 40 years experiencing extraskeletal tumors,metastatic spread at the time of diagnosis,and shorter survival than younger patients.It shows aggressive clinical behavior with a high rate of local recurrence and distant metastasis[8].Approximately 15%-46% of patients will demonstrate metastatic disease at presentation,reducing 5-year survival from approximately 35%-71% to a dismal 0-34%[9].
TREATMENT
After multidisciplinary consultation,the physicians recommended 5 cycles of neoadjuvant chemotherapy with vincristine,ifosfamide,and doxorubicin for the patient,which could reduce the size of the primary tumor and metastases.However,the patient refused this treatment strategy.The patient was given fluid rehydration (0.9% sodium chloride solution,5% glucose sodium chloride injection),nutritional support (Compound amino acid injection,20% medium and long chain fat emulsion injection and ω-3 fish oil fat emulsion injection) and intravenous injection of parecoxib sodium 40 mg to relieve the pain.
If I do it for you how will you ever learn to do it yourself? I said. Suddenly, I was back at that general store where I had learned the hard way to tally12 up my bill along with the cashier. Had I ever been overcharged since?
OUTCOME AND FOLLOW-UP
One month later,the patient could not eat and received symptomatic nutritional support (Compound amino acid injection,20% medium and long chain fat emulsion injection and ω-3 fish oil fat emulsion injection) and analgesic treatment (intravenous injection of parecoxib sodium 40 mg).Despite the medical advice,the patient refused to receive any systemic treatment.The patient chose to be transferred to hospice care ward and died of multiple organ failure caused by widespread multiorgan metastases 2-mo later.
DlSCUSSlON
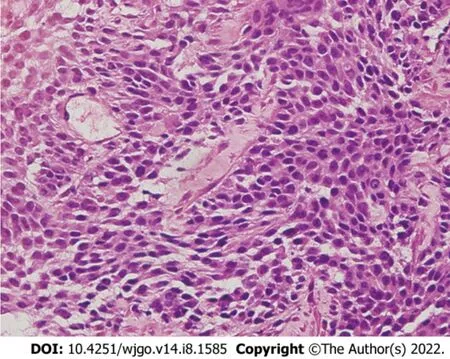
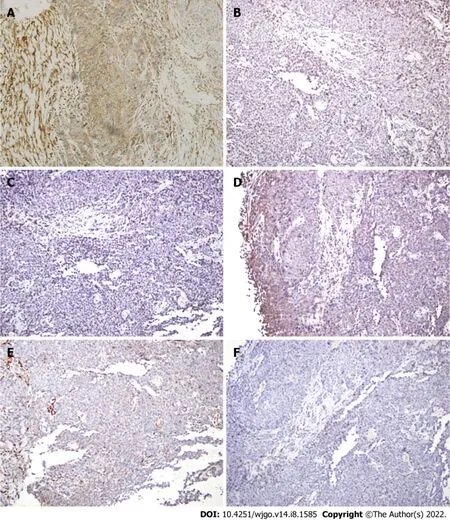
To make the diagnosis,transabdominal ultrasound guided needle biopsy was performed with the consent of the patient.The biopsy was performed as an outpatient procedure under local anesthesia.Histopathology of the small intestinal tumor is composed of heteromorphic cells,and distributed in the shape of a sheet nest with round or oval cells and visible nucleoli (Figure 3).Tumor cells showed positive immunoreactivity for CD99,NKX2.2,S100,Syn and Ki-67,and the Ki-67 Level was greater than 60%.The results were negative for CK,CgA,CK5/6,P63,CK7,CAM5.2,CK20,CD56,CD117 and alphainhibin (Figure 4).Therefore,the histopathologic findings were consistent with EOES.Although without molecular biological examination,after multidisciplinary consultation,the clinician concluded the diagnosis was primary small intestinal ES because of the positive immunoreactivity for NKX2.2,FLI-1 and CD99 combined with morphological characteristics.
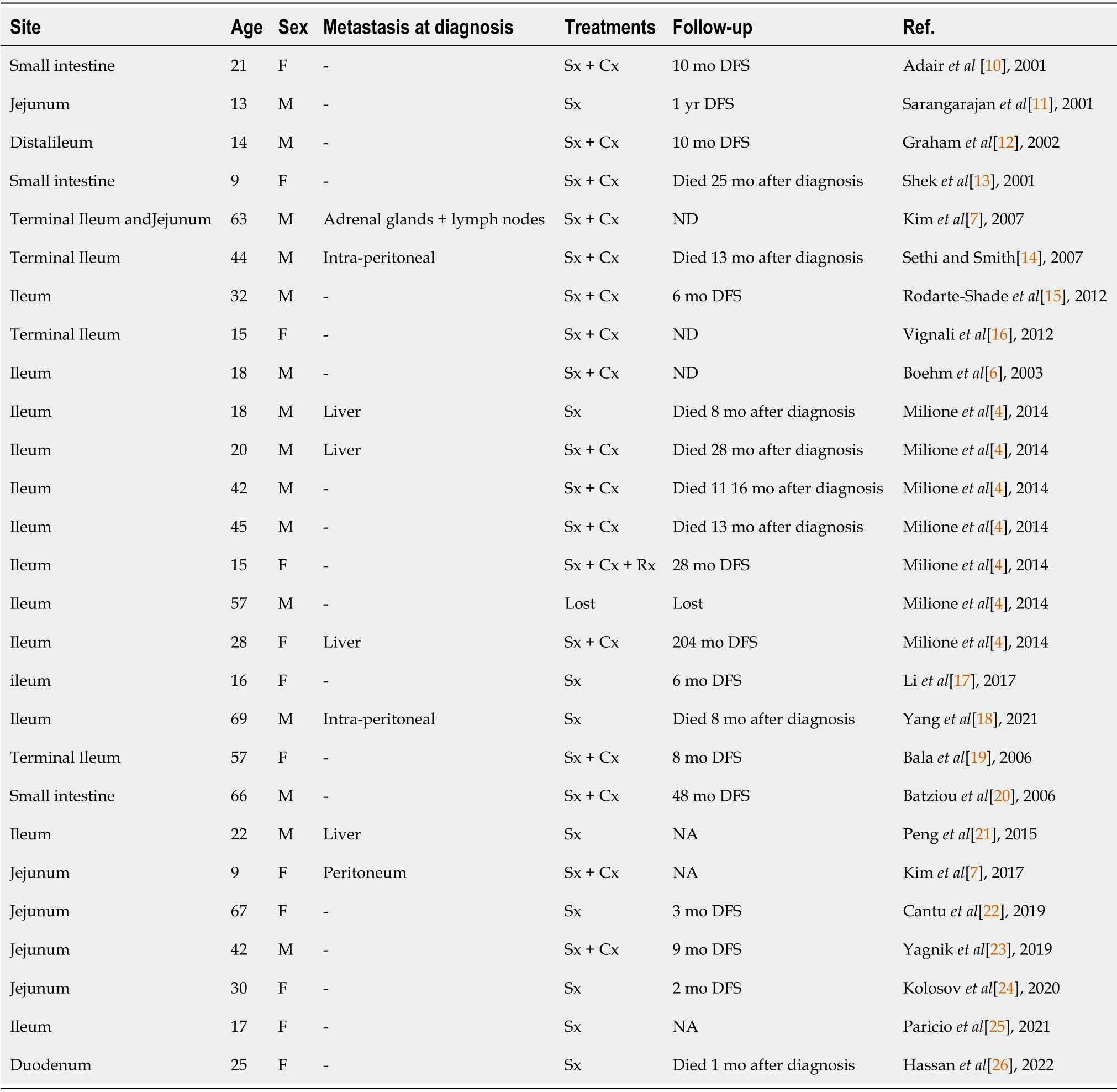
We have summarized all previous publications of small intestinal ES/PNET in Table 1[10-26].The patient gender ratio (female/male) was 12/15.The ages ranged from 9 to 69 years,and 60% of patients with small intestinal ES were younger than 30 years.The most common sites in patients with metastatic disease are the liver and peritoneum.Adrenal metastases have rarely been described[7].Seven patients had metastases to the liver and peritoneum solitarily.Only one patient had metastases to the adrenal gland and peritoneum at the time of diagnosis.Patients of more than 40 years of age or with metastatic spread at the time of diagnosis have shorter survival than younger patients.The form of distant metastasis included seeding,blood and lymphatic vessel metastasis.The mechanism of distant metastasis from the ES in the ileum to other organs could be explained for two reasons.First,hematogenous metastasis may occur because the tumor cells penetrate and spread from the vessels in the ileum.Second,there are abundant lymphatic networks in the submucosal layer of the ileum,and the lymphatics intermittently pierce the muscularis propria and drain into regional lymph nodes in the peritoneum.The tumor cells penetrate and spread from lymphatics to regional lymph nodes or evendistal lymph nodes.
The most frequently presenting symptom is a rapidly growing mass with local pain.However,the accompanying symptoms depend largely on the sarcoma site[27].Our patient complained of right lower quadrant pain accompanied by acid reflux,belching,and emesis.CT showed a large,sharply delineated mass of relatively lower or equal density to that of the adjacent muscle.After enhancement,the mass showed heterogenetic enhancement with intratumor necrosis and calcification.Calcification is seen in 25%-30% of previous cases[1].This patient had metastases of the bilateral adrenal gland,liver,pancreas and lung and multiple regional lymph node metastases.These findings represent necrotic changes common in both EOES and its metastases,which reflect the disease’s aggressive nature[2].
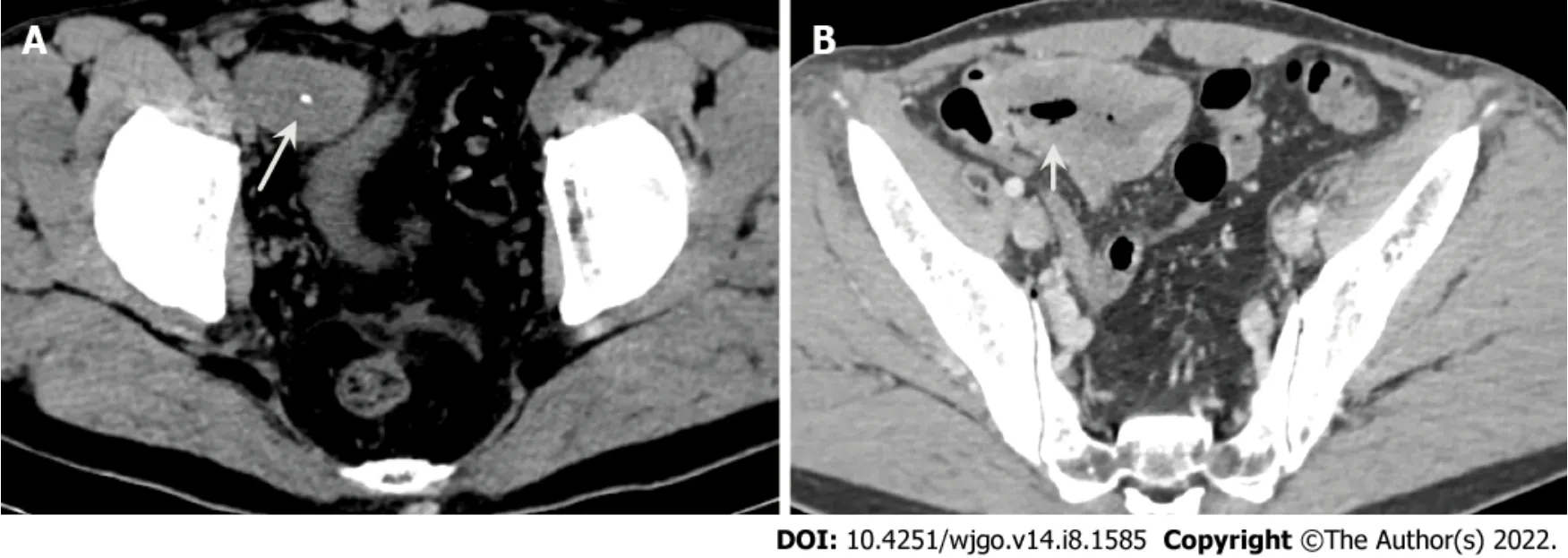
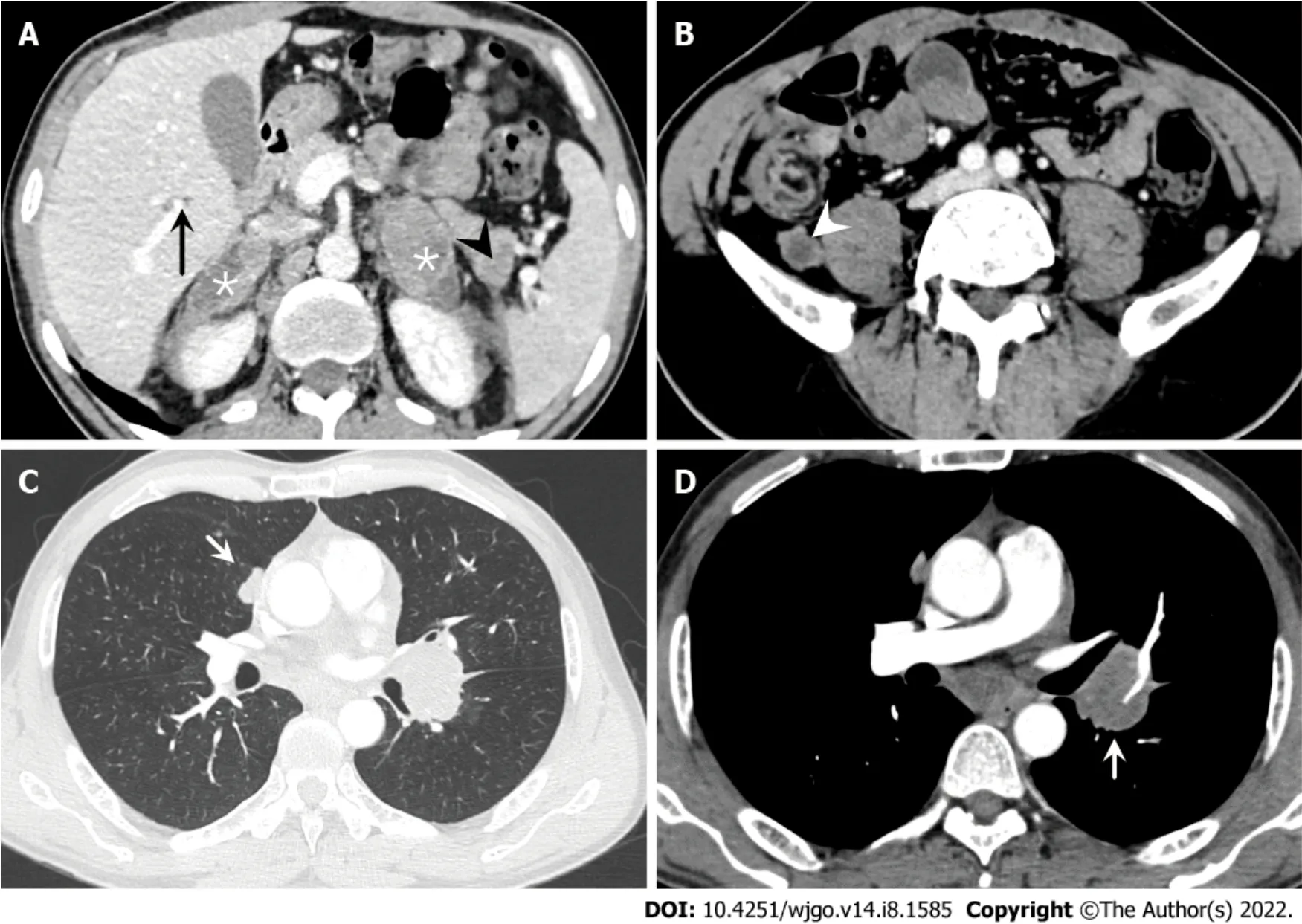
Contrast-enhanced computed tomography (CT) of the abdomen showed an 8.1 cm × 4.0 cm mass in the right iliac fossa area,which interacted with the small intestinal lumen.The mass was heterogenetic,and areas of low attenuation and high attenuation were observed,likely corresponding to areas of necrosis and calcification (Figure 1).In addition,multiple metastatic lesions were observed on the bilateral adrenal gland,lung,liver and pancreas,and several enlarged lymph nodes were seen in the retroperitoneal and mediastinum areas,with the largest exhibiting a diameter of 2.3 cm (Figure 2).
Neoadjuvant chemotherapy was initially used to eliminate micrometastases and reduce the size of the primary tumor[40].ES is quite radiosensitive,and some researchers have emphasized the important role of preoperative radiotherapy for successful local treatment in spinal ES[41].However,improvements in surgical technique and the risks associated with radiation (secondary malignancies) have reduced the reliance on radiation[42].Surgery alone does not appear to be effective for metastatic ES due to technical difficulties related to surgery and a low survival rate.This case will contribute to understanding the prognosis and determination of optimal management because small bowel ES is extremely rare and difficult to cure.
CONCLUSlON
In conclusion,EOES originating in the ileum with widespread multiorgan metastases is rare and easily misdiagnosed.When a small intestinal mass accompanied by calcification and wide multiorgan metastases is seen on CT,a suspicion of EOES should not be overlooked.Together with previous reports,this case has expanded knowledge about the spectrum of tumors in the small intestine.
The good-natured fiddler bent13 down to pick it up, but in the twinkling of an eye the little man had jumped on to his back, and beat him till he was black and blue all over his head and body
Touched by her story, the minister insisted that she take the cloth. She thought about it for a moment but said no, she didn’t need it any longer, and it did look pretty hanging behind the altar. Then she said good-bye and left.
As he turned a corner the little hare cut off both his ears, so that they should not know him, and pretended to be working at a grindstone which lay there
For differentiation of Ewing sarcoma from the other small round cell tumors,molecular detection of specific fusion genes is recommended,which accepted as the gold standard method for diagnosing Ewing sarcoma[17].However,this patient did not do this due to a small tissue sample size.Immunohistochemistry has emerged as a compelling alternative.NKX2.2,CD99 and FLI-1 are good immunohistochemical markers for ES.NKX2.2 was shown to be a valuable immunohistochemical marker for ES in the differential diagnosis of small round cell tumors,which has been identified as an important target of EWS-FLI-1[28,29].A few number of non-Ewing tumors can be positive for NKX2.2,such as synovial sarcomas,mesenchymal chondrosarcomas,and malignant melanomas.Nuclear spindling and TLE1 immunoreactivity favor synovial sarcomas[30].NKX2.2-positive synovial sarcoma exhibited weak focal staining compared to diffuse labeling of ES.Mesenchymal chondrosarcomas could be excluded based on histology and immunohistochemical data[31].Malignant melanomas could be excluded because the tumor did not express specific melanoma markers (
,HMB45 and Melan A)[32].According to the exclusive diagnosis,the present case was ultimately diagnosed as synchronous ES.
Li H and Guo AW were responsible for the coordination of the project and contributed to the study design; Li H,Guo AW,Yuan Y and Liu YS collected,analyzed the data and edited the manuscript.Yuan Y and Li SX followed up the patient; Yuan Y and Li H supervised the study and reviewed this manuscript; All authors have read and approved the final manuscript.
The patient involved in this study gave his written consent authorizing use and disclosure of his protected health information.
From the contrast-enhanced CT of the abdomen and chest,multidisciplinary consultation determined that malignant GISTs with widespread multiorgan metastases were first considered.The patient could not receive surgical treatment because of widespread multiorgan metastases.Therefore,adjuvant chemotherapy was recommended.
Thanks to the families,friends and colleagues who support our work.
The authors have read the CARE Checklis (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Don t you know, young lady,” he said harshly2, “when you give someone a present there s supposed to be something inside the package! The little girl looked up at him with tears rolling from her eyes and said: Daddy, it s not empty
China
Ai-Wen Guo 0000-0002-2488-7609; Yi-Sha Liu 0000-0002-8769-1734; Hang Li 0000-0003-2920-0025; Yi Yuan 0000-0001-8058-8534; Si-Xun Li 0000-0001-7514-2992.
Who are you? said Browny, starting up in great fright, for though the voice sounded gentle, he felt sure it was a feigned13 voice, and he feared it was the fox.
Wu YXJ
A
Wu YXJ
1 Murphey MD,Senchak LT,Mambalam PK,Logie CI,Klassen-Fischer MK,Kransdorf MJ.From the radiologic pathology archives: ewing sarcoma family of tumors: radiologic-pathologic correlation.
2013; 33: 803-831 [PMID:23674776 DOI: 10.1148/rg.333135005]
2 Javery O,Krajewski K,O'Regan K,Kis B,Giardino A,Jagannathan J,Ramaiya NH.A to Z of extraskeletal Ewing sarcoma family of tumors in adults: imaging features of primary disease,metastatic patterns,and treatment responses.
2011; 197: W1015-W1022 [PMID: 22109315 DOI: 10.2214/AJR.11.6667]
3 Galyfos G,Karantzikos GA,Kavouras N,Sianou A,Palogos K,Filis K.Extraosseous Ewing Sarcoma: Diagnosis,Prognosis and Optimal Management.
2016; 78: 49-53 [PMID: 27186040 DOI: 10.1007/s12262-015-1399-0]
4 Milione M,Gasparini P,Sozzi G,Mazzaferro V,Ferrari A,Casali PG,Perrone F,Tamborini E,Pellegrinelli A,Gherardi G,Arrigoni G,Collini P,Testi A,De Paoli E,Aiello A,Pilotti S,Pelosi G.Ewing sarcoma of the small bowel: a study of seven cases,including one with the uncommonly reported EWSR1-FEV translocation.
2014; 64: 1014-1026 [PMID: 24898918 DOI: 10.1111/his.12350]
5 El Weshi A,Allam A,Ajarim D,Al Dayel F,Pant R,Bazarbashi S,Memon M.Extraskeletal Ewing's sarcoma family of tumours in adults: analysis of 57 patients from a single institution.
2010; 22: 374-381 [PMID:20466282 DOI: 10.1016/j.clon.2010.02.010]
6 Boehm R,Till H,Landes J,Schmid I,Joppich I.Ileoileal intussusception caused by a Ewing sarcoma tumour.An unusual case report.
2003; 13: 272-275 [PMID: 13680499 DOI: 10.1055/s-2003-42234]
7 Kim DW,Chang HJ,Jeong JY,Lim SB,Lee JS,Hong EK,Lee GK,Choi HS,Jeong SY,Park JG.Ewing's sarcoma/primitive neuroectodermal tumor (ES/PNET) of the small bowel: a rare cause of intestinal obstruction.
2007; 22: 1137-1138 [PMID: 16683104 DOI: 10.1007/s00384-006-0142-5]
8 Worch J,Ranft A,DuBois SG,Paulussen M,Juergens H,Dirksen U.Age dependency of primary tumor sites and metastases in patients with Ewing sarcoma.
2018; 65: e27251 [PMID: 29856530 DOI:10.1002/pbc.27251]
9 Esiashvili N,Goodman M,Marcus RB Jr.Changes in incidence and survival of Ewing sarcoma patients over the past 3 decades: Surveillance Epidemiology and End Results data.
2008; 30: 425-430 [PMID: 18525458 DOI: 10.1097/MPH.0b013e31816e22f3]
10 Adair A,Harris SA,Coppen MJ,Hurley PR.Extraskeletal Ewings sarcoma of the small bowel: case report and literature review.
2001; 46: 372-374 [PMID: 11768578 DOI: 10.1016/S1072-7515(01)01094-8]
11 Sarangarajan R,Hill DA,Humphrey PA,Hitchcock MG,Dehner LP,Pfeifer JD.Primitive neuroectodermal tumors of the biliary and gastrointestinal tracts: clinicopathologic and molecular diagnostic study of two cases.
2001;4: 185-191 [PMID: 11178636 DOI: 10.1007/s100240010141]
12 Graham DK,Stork LC,Wei Q,Ingram JD,Karrer FM,Mierau GW,Lovell MA.Molecular genetic analysis of a small bowel primitive neuroectodermal tumor.
2002; 5: 86-90 [PMID: 11815873 DOI:10.1007/s10024-001-0192-1]
13 Shek TWH,Chan GCF,Khong PL,Chung LP,Cheung ANY.Ewing Sarcoma of the Small Intestine.
2001; 23: 530-532 [PMID: 11878783 DOI: 10.1097/00043426-200111000-00013]
14 Sethi B,Smith GT.Primary primitive neuroectodermal tumour arising in the small bowel.
2007; 50: 665-666 [PMID: 17394505 DOI: 10.1111/j.1365-2559.2007.02631.x]
15 Rodarte-Shade M,Palomo-Hoil R,Vazquez J,Ancer A,Vilches N,Flores-Gutierrez JP,Sierra M,Garza-Serna U.Primitive Neuroectodermal Tumor (PNET) of the Small Bowel in a Young Adult with Lower Gastrointestinal Bleeding.
2012; 43: S243-S245 [PMID: 22760712 DOI: 10.1007/s12029-012-9409-y]
16 Vignali M,Zacchè MM,Messori P,Natale A,Busacca M.Ewing's sarcoma of the small intestine misdiagnosed as a voluminous pedunculated uterine leiomyoma.
2012; 162: 234-235 [PMID: 22410473 DOI: 10.1016/j.ejogrb.2012.02.009]
17 Li T,Zhang F,Cao Y,Ning S,Bi Y,Xue W,Ren L.Primary Ewing's sarcoma/primitive neuroectodermal tumor of the ileum: case report of a 16-year-old Chinese female and literature review.
2017; 12: 37 [PMID: 28472972 DOI: 10.1186/s13000-017-0626-3]
18 Yang J,Wei H,Lin Y,Lin N,Wu S,Yu X.Challenges of Diagnosing Primary Ewing's Sarcoma in the Small Intestine of the Elderly: A Case Report.
2021; 11: 565196 [PMID: 34307115 DOI: 10.3389/fonc.2021.565196]
19 Bala M,Maly A,Remo N,Gimmon Z,Almogy G.Peripheral primitive neuroectodermal tumor of bowel mesentery in adults.
8: 515-516 [PMID: 16889176]
20 Batziou C,Stathopoulos GP,Petraki K,Papadimitriou C,Rigatos SK,Kondopodis E,Stathopoulos J,Batzios S.Primitive neurectodermal tumors: a case of extraosseous Ewing's sarcoma of the small intestine and review of the literature.
2006; 11: 519-522 [PMID: 17309187]
21 Peng L,Yang L,Wu N,Wu BO.Primary primitive neuroectodermal tumor arising in the mesentery and ileocecum: A report of three cases and review of the literature.
9:1299-1303 [PMID: 25780425 DOI: 10.3892/etm.2015.2242]
22 Cantu C,Bressler E,Dermawan J,Paral K.Extraskeletal Ewing Sarcoma of the Jejunum: A Case Report.
2019;23: 255 [PMID: 31314729 DOI: 10.7812/TPP/18-255]
23 Yagnik VD,Dawka S.Extraskeletal Ewing's sarcoma/peripheral primitive neuroectodermal tumor of the small bowel presenting with gastrointestinal perforation.
2019; 12: 279-285 [PMID: 31417299 DOI:10.2147/ceg.s203697]
24 Kolosov A,Dulskas A,Pauza K,Selichova V,Seinin D,Stratilatovas E.Primary Ewing's sarcoma in a small intestine - a case report and review of the literature.
2020; 20: 113 [PMID: 32450834 DOI: 10.1186/s12893-020-00774-z]
25 Paricio JJ,Ruiz Martín J,Sánchez Díaz E.Primary Ewing's sarcoma of the small intestine.
2021;113: 680 [PMID: 33486963 DOI: 10.17235/reed.2021.7735/2020]
26 Hassan R,Meng LV,Ngee KT,I-Vern L,Sankaran P,Hean LC,Euxian L,Mohamad H,Dusa NM,Subramaniam M.Extraskeletal Ewing sarcoma of the duodenum presenting as duodenojejunal intussusception.
2022; 399: 1265[PMID: 35339226 DOI: 10.1016/s0140-6736(22)00361-0]
27 Applebaum MA,Goldsby R,Neuhaus J,DuBois SG.Clinical features and outcomes in patients with Ewing sarcoma and regional lymph node involvement.
2012; 59: 617-620 [PMID: 22184129 DOI: 10.1002/pbc.24053]
28 Smith R,Owen LA,Trem DJ,Wong JS,Whangbo JS,Golub TR,Lessnick SL.Expression profiling of EWS/FLI identifies NKX2.2 as a critical target gene in Ewing's sarcoma.
2006; 9: 405-416 [PMID: 16697960 DOI:10.1016/j.ccr.2006.04.004]
29 Yoshida A,Sekine S,Tsuta K,Fukayama M,Furuta K,Tsuda H.NKX2.2 is a useful immunohistochemical marker for Ewing sarcoma.
2012; 36: 993-999 [PMID: 22446943 DOI: 10.1097/PAS.0b013e31824ee43c]
30 Terry J,Saito T,Subramanian S,Ruttan C,Antonescu CR,Goldblum JR,Downs-Kelly E,Corless CL,Rubin BP,van de Rijn M,Ladanyi M,Nielsen TO.TLE1 as a diagnostic immunohistochemical marker for synovial sarcoma emerging from gene expression profiling studies.
2007; 31: 240-246 [PMID: 17255769 DOI:10.1097/01.pas.0000213330.71745.39]
31 Owen LA,Kowalewski AA,Lessnick SL.EWS/FLI mediates transcriptional repression
NKX2.2 during oncogenic transformation in Ewing's sarcoma.
2008; 3: e1965 [PMID: 18414662 DOI: 10.1371/journal.pone.0001965]
32 Wehrli BM,Huang W,De Crombrugghe B,Ayala AG,Czerniak B.Sox9,a master regulator of chondrogenesis,distinguishes mesenchymal chondrosarcoma from other small blue round cell tumors.
2003; 34: 263-269[PMID: 12673561 DOI: 10.1053/hupa.2003.41]
33 Yamamoto H,Oda Y.Gastrointestinal stromal tumor: recent advances in pathology and genetics.
2015; 65: 9-18 [PMID: 25414046 DOI: 10.1111/pin.12230]
34 Levy AD,Remotti HE,Thompson WM,Sobin LH,Miettinen M.Gastrointestinal stromal tumors: radiologic features with pathologic correlation.
2003; 23: 283-304 [PMID: 12640147 DOI: 10.1148/rg.232025146]
35 Hayashi D,Devenney-Cakir B,Lee JC,Kim SH,Cheng J,Goldfeder S,Choi BI,Guermazi A.Mucosa-associated lymphoid tissue lymphoma: multimodality imaging and histopathologic correlation.
2010; 195:W105-W117 [PMID: 20651169 DOI: 10.2214/AJR.09.4105]
36 Mendelson RM,Fermoyle S.Primary gastrointestinal lymphomas: a radiological-pathological review.Part 1: Stomach,oesophagus and colon.
2005; 49: 353-364 [PMID: 16174173 DOI: 10.1111/j.1440-1673.2005.01457.x]
37 Salyers WJ,Vega KJ,Munoz JC,Trotman BW,Tanev SS.Neuroendocrine tumors of the gastrointestinal tract: Case reports and literature review.
2014; 6: 301-310 [PMID: 25132927 DOI:10.4251/wjgo.v6.i8.301]
38 Malla S,Kumar P,Madhusudhan KS.Radiology of the neuroendocrine neoplasms of the gastrointestinal tract: a comprehensive review.
2021; 46: 919-935 [PMID: 32960304 DOI: 10.1007/s00261-020-02773-3]
39 Yuan Y,Pu H,Pang MH,Liu YS,Li H.Thymic carcinoma metastasize to the small intestine: a case report.
2020; 20: 358 [PMID: 33115438 DOI: 10.1186/s12876-020-01505-7]
40 DuBois SG,Krailo MD,Gebhardt MC,Donaldson SS,Marcus KJ,Dormans J,Shamberger RC,Sailer S,Nicholas RW,Healey JH,Tarbell NJ,Randall RL,Devidas M,Meyer JS,Granowetter L,Womer RB,Bernstein M,Marina N,Grier HE.Comparative evaluation of local control strategies in localized Ewing sarcoma of bone: a report from the Children's Oncology Group.
2015; 121: 467-475 [PMID: 25251206 DOI: 10.1002/cncr.29065]
41 Vogin G,Helfre S,Glorion C,Mosseri V,Mascard E,Oberlin O,Gaspar N.Local control and sequelae in localised Ewing tumours of the spine: a French retrospective study.
2013; 49: 1314-1323 [PMID: 23402991 DOI:10.1016/j.ejca.2012.12.005]
42 Dunst J,Schuck A.Role of radiotherapy in Ewing tumors.
2004; 42: 465-470 [PMID: 15049022 DOI: 10.1002/pbc.10446]
 World Journal of Gastrointestinal Oncology2022年8期
World Journal of Gastrointestinal Oncology2022年8期
- World Journal of Gastrointestinal Oncology的其它文章
- Colitis and colorectal tumors should be further explored and differentiated
- Exosomes:Promising biomarkers and targets for cancer
- Acute or chronic inflammation role in gastrointestinal oncology
- RASSF1A methylation as a biomarker for detection of colorectal cancer and hepatocellular carcinoma
- Evaluation of the diagnostic value of serum-based proteomics for colorectal cancer
- Duodenal-type follicular lymphoma more than 10 years after treatment intervention:A retrospective single-center analysis