
Del(5q) and inv(3) in myelodysplastic syndrome:A rare case report
2022-06-23 02:07:00HaiPingLiangXingChunLuoYaLiZhangBeiLiu
World Journal of Clinical Cases 2022年11期
lNTRODUCTlON
Myelodysplastic syndrome (MDS) is defined as a typical heterogeneous group of clonal haematopoietic disorders characterized by dysplastic and ineffective haematopoiesis, and approximately 30% of patients progress to acute myeloid leukaemia (AML)[1,2]. The incidence of MDS is associated with age,especially in people 60 years older, and males are more susceptible than females[3]. MDS patients generally have poor outcomes, with a median overall survival of 5 years[2].According to the International Prognostic Scoring System (IPSS) and revised International Prognostic Scoring System (IPSS-R),cytogenetic abnormalities, especially certain unbalanced abnormalities, have a profound impact on the prognosis of MDS patients[4]. Unbalanced chromosomal abnormalities caused by partial acquisition or deletion of chromosomes are common in MDS[5]. These abnormalities often occur during tumorigenesis and play a crucial role in MDS progression.
Here, we report a case of an MDS patient with clonal progression from del(5q) to inv(3) and del(5q),who was treated with azacitidine after lenalidomide resistance. Furthermore, we will summarize the genetic abnormalities and treatment strategies to add a corresponding contribution to the treatment and prognosis of these patients.
CASE PRESENTATlON
Chief complaints
In September 2020, a 66-year-old woman was admitted to our hospital for progressive chest tightness and shortness of breath.
History of present illness
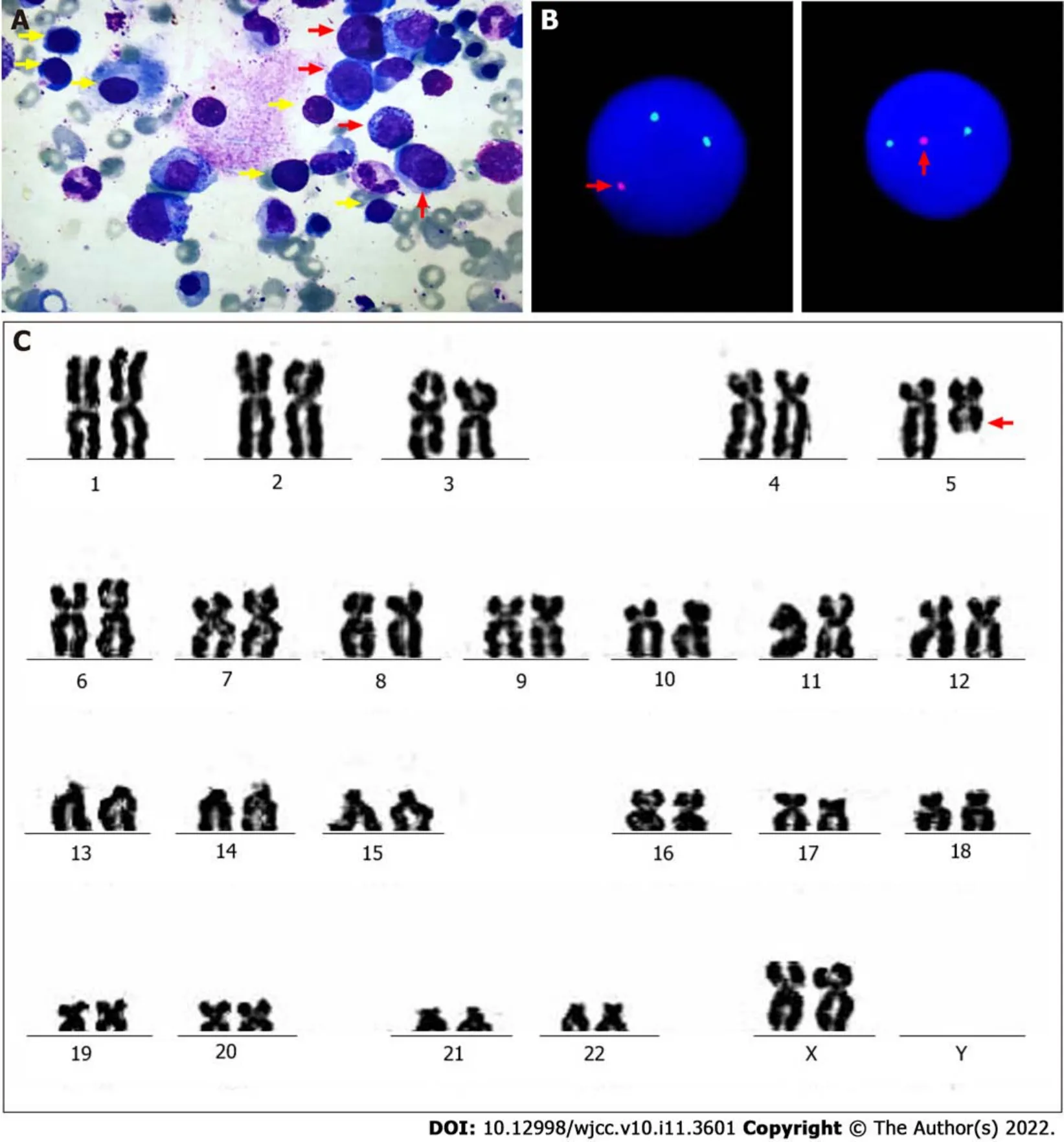
One year prior, the patient had been admitted to the hospital with severe anaemia and thrombocytosis.Physical examination showed that the patient had an anaemic appearance. The results of peripheral blood examination were as follows:red blood cell (RBC) count, 1.0 × 10/L; platelet (PLT) count, 409 ×10/L; haemoglobin (HB), 36 g/L; creatinine, 0.55 mg/dL; and lactate dehydrogenase (LDH), 418 U/L.Bone marrow trephine biopsy revealed more than 10% abnormal megakaryocytes (single round nuclei and cytosolic lobulated micronuclei) (Figure 1A). Fluorescence in situ hybridization (FISH) indicated deletion of the(5q31) gene (Figure 1B). Furthermore, the karyotype was described as 46, XX,del(5)(q13q31) by G band staining (Figure 1C). Based on clinical manifestations and laboratory tests, the patient was diagnosed with low-risk MDS (low risk, IPSS-R = 2.5). The endothelial activation and stress index (EASIX) was 0.56. EASIX is an independent prognostic factor for lower-risk MDS patents that was calculated by the following formula:LDH (U/L) × creatinine (mg/dL)/PLT (nL)[6]. The patient was advised to be treated with lenalidomide. The dosing schedule was 10 mg/d or 21 d in a 28-d cycle. After three cycles of treatment, peripheral blood examination showed HB 97 g/L and PLT 341 × 10/L.
History of past illness
The patient was previously healthy. There was no disease history in other systems.
You are my destined29 husband, and, beloved by me, and endowed with every kind of riches and power, you shall spend the remainder of your life in peace and happiness
Personal and family history
No contributory personal history or similar family history.
On the second last day of the tour we were making our way to Calais and the ferryboat that would take us back across the English Channel, on to London and finally the airport. Throughout the war memorial that the people of France erected4 to the Canadian soldiers who fought so bravely here the trip as we rode along in the coach our wonderful French guide provided a colourful and interesting commentary to give us a better understanding of what we were seeing out the window.
Physical examination
Lenalidomide therapy is initially recommended based on age, general conditions, and cytogenetic abnormalities. Since 2005, the Food and Drug Administration of the United States has approved the use of lenalidomide for the treatment of transfusion-dependent low-risk MDS with or without del(5q), and it has been indicated that lenalidomide could reduce transfusion requirements and reverse cytogenetic abnormalities[12]. Lenalidomide is the first and only treatment for cytogenetically defined subsets of MDS disease, especially MDS with del(5q). However, not all patients achieve a long-term response. It was reported that approximately half of patients with del(5q) lost response or progression after 2-3 years of treatment[13]. Indeed, lenalidomide resistance has become a common event in the treatment of MDS.
Laboratory examinations
The results of the peripheral blood examination were as follows:RBC, 2.27 × 10/L; WBC, 1.93 × 10/L;PLT, 114 × 10/L; and HB, 58 g/L.
Further diagnostic work-up
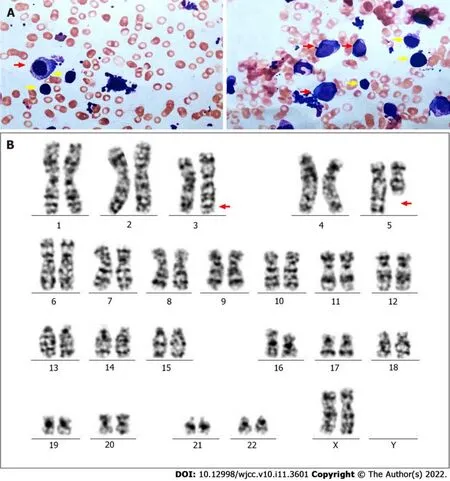
Bone marrow aspirate smears showed hypercellularity with marked myeloid and erythroid hypoplasia and a blast cell count of 16% (Figure 2A). Another karyotype examination revealed 46, XX,inv(3)(q21q26), and del(5)(q13q31) (Figure 2B). qRT–PCR showed that the EVI1 expression level was 90.63%, which was classified as high expression.
When I was a sophomore8, I wrote an article about myself for the school newspaper, and people started asking me what my disability was like. They told me I was brave for having gone through the 15 surgeries I needed to help correct my condition. I never heard anyone say anything mean, and it felt good to help people get to know me better.
FlNAL DlAGNOSlS
According to the IPSS-R, the patient's diagnosis was revised to high-risk MDS (very high risk, IPSS-R =7.5).
TREATMENT
Mr. Coyote was getting very old and had to be more careful for his own safety. He had been walking for hours and hours through a beautiful valley when he came upon a large tree. Mr. Coyote was very tired and wanted to rest but he also needed to be safe. He kindly1 asked the tree, Please open up so I can rest safely in your care .
OUTCOME AND FOLLOW-UP
Then they came to a stream of rushing water; but the little man drew out a wand and touched the waves, whereupon the waters parted and stood still, and the two crossed the river with dry feet
DlSCUSSlON
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Combining bone marrow cytogenetics, the percentage of bone marrow blasts and cytopenia, our patient was classified as low risk according to the IPSS-R at primary diagnosis. In recent years,cardiovascular disease has been considered to be the second most common cause of death among patients with low-risk MDS after haematological complications[11]. Therefore, we used EASIX to assess the patient’s cardiovascular risk, which was 0.56[6]. Because the patient had no previous history of cardiovascular disease and the cardiovascular examination results were negative at admission, we alleviated the patient's cardiovascular disease concerns. Considering the IPSS-R and EASIX, we preliminarily evaluated the patient had a good prognosis.
Out Goldilocks jumped;21 and whether she broke her neck in the fall; or ran into the wood and was lost there; or found her way out of the wood, and was taken up by the constable11 and sent to the House of Correction for a vagrant12 as she was,22 I cannot tell
We continued to treat the patient with lenalidomide. In less than one treatment cycle, the patient rapidly developed resistance to the drug. Subsequently, we tried azacitidine as a treatment and administered 75 mg/m/d intravenously for 7 consecutive days every 28 d. After two courses, haematology showed HB 70 g/L and PLT 56 × 10/L. After the fourth cycle, peripheral blood examination revealed HB 40 g/L and PLT 14 × 10/L. Bone morrow aspirate smears revealed that nucleated cells accounted for 6% of the cell population. A mutation of thegene [NM 015338:c.4232_4233delinsA(p. W1411*) exon 12]with a variant allele frequency of 33.1% was detected. Subsequently, her medical condition gradually deteriorated. In view of the present situation, we recommended HSCT.
Physical examination showed that the patient had a moderate anaemic appearance. Her vital signs were stable, with no other positive findings.
The condition of our patient worsened again after a short period of time, and we considered HSCT.At present, for both low-risk and high-risk MDS patients, HSCT is still the only curative treatment[19].Patients under 65 years of age and suitable healthy elderly patients should be strongly recommended for HSCT with a suitable donor with the same human leukocyte antigen[20]. Among high-risk MDS patients undergoing HSCT, 40-50% of patients have achieved a prolonged disease-free survival and have improved over the years[21]. However, the optimal timing of HSCT and the specific chemical regimen before HSCT treatment is still a controversial issue. It is generally believed that an increase in the percentage of bone marrow blasts, especially if it is greater than 10%, is associated with a higher risk of recurrence[22]. In addition, the existence of poor prognostic mutations, especially mutations in TP53,ASXL1 and RUNX1, should be considered for the use of HSCT to reduce the risk of recurrence[23].However, in our case, when we recommended that the patient undergo HSCT, the patient rejected the recommendation for unknown reasons. Subsequently, the patient chose to leave the hospital voluntarily, and we learned during follow-up that the patient died of serious infection after four months.
After the lenalidomide treatment failed, inv(3) with EVI1 overexpression and ASXL1 mutations occurred in the patient. Based on clinical assessments and laboratory examination, the patient's diagnosis was revised to high-risk MDS. We then tried to treat the patient with azacytidine, which is a demethylation drug. Demethylation drugs mainly include azacitidine and decitabine, both of which can inhibit DNA methylation by binding to DNA. Interestingly, azacitidine also binds to RNA to inhibit RNA synthesis and protein metabolism[16]. Sallman[16] reported a study about the response to azacitidine in del(5q) MDS patients after lenalidomide resistance. Among 18 del(5q) MDS patients treated with azacytidine, the overall response rate was 56%, including a complete response rate of 5.6%,a marrow complete response rate of 11.1%, and a haematological improvement rate of 38.9%.Azacitidine had the same effect in del(5q) and non-del(5q) patients[17]. In the study by Wanquet[18], 157 AML/MDS patients with chromosome 3q abnormalities and 27 patients with isolated EVI1 overexpression were treated with azacitidine. The overall response rate was 50%, including a complete remission rate of 29%, and the median overall survival time was 10.6 mo. AML/MDS with 3q abnormalities has a special response to azacitidine, and azacitidine is an appropriate choice before the patient receives allohaematopoietic stem cell transplantation[18]. To date, there have been a few reports on the treatment of MDS with decitabine[3]. Therefore, we believe that azacitidine is a reasonable option for the treatment of MDS after the failure of lenalidomide. Our patient experienced a short-term improvement after 2 courses of azacitidine treatment.
What! cried the Princess, do you think I am come to beg of you? I don t know about that, answered she; but at any rate you don t seem to have come to bring me anything
In our case, lenalidomide treatment initially showed a good response in the patient, but the patient rapidly developed drug resistance after the first remission. Based on the available data, we found that the occurrence of primary resistance to lenalidomide in MDS is mainly related to TP53 mutations. We reviewed the role of TP53 mutations and abnormal p53 pathway activation in myeloid malignant tumours. In del (5q) patients who had a high mutation rate of TP53, the cytogenetic complete remission rate was less than 12% after treatment with lenalidomide[7]. Therefore, it is plausible that there is a high correlation between TP53 mutations and lenalidomide resistance. In addition, lenalidomide upregulates RUNX1 expression in a CRBN- and TP53 -dependent manner in del (5q) MDS, and RUNX1 induces megakaryocyte differentiation and apoptosis assisted by GATA2. As a result, lenalidomide resistance occurs when RUNX1 is mutated or downregulated[14]. The secondary or acquired resistance to lenalidomide is associated with the overexpression of PP2A. The overexpression of PP2A leads to the degradation of p53 in red blood cell precursors and the instability of β-catenin, which is more conducive to the evolution of del(5q) clones[15]. However, TP53 and RUNX1 mutations were not detected in our case. The acquired resistance of our patients to lenalidomide may be related to PP2A abnormalities, but further sufficient data is required for further exploration.
CONCLUSlON
In summary, we report a rare case of MDS with clonal evolution from del(5) to inv(3). Although lenalidomide and azacitidine provided temporary remission to the patient, the patient inevitably has a poor prognosis. The complex and heterogeneous pathophysiology of MDS is still the main reason for the limited effectiveness of current treatments; thus, emerging therapeutic strategies are still urgently needed.
The patient was discharged and wilfully refused HSCT. After four months, the patient died of the infection.
Liang HP designed the study and wrote the manuscript; Luo XC collected and analyzed the data; Zhang YL prepared figures; Liu B was in charge of patient treatment and designed the paper; all authors read and approved the final manuscript.
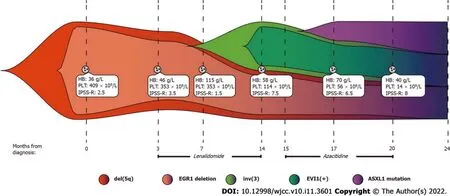
We report a rare case of MDS with clonal evolution from del(5q) to inv(3) (Figure 3). MDS with del(5q),also known as 5q-syndrome, is a specific type of MDS that has a better prognosis than other subtypes of MDS. The median expected survival time of this syndrome is approximately 58 mo[7]. Deletion of chromosome arm 5q results in the deletion of genes located on this chromosome, including SPARC,EGR1, CTNNA1, APC and NPM1[8]. Based on this, we used LSI EGR1 and D5S23 and a D5S721 dual colour probe to detect del(5q). MDS with inv(3)/t(3) is considered to be a rare event (< 1%); it is an invasive disease with a high risk of developing AML. Furthermore, high expression of EVI1 was observed with chromosome 3 abnormalities in our case. EVI1 is an oncogenic transcriptional regulator that may be involved in the proliferation and maintenance of haematopoietic stem cells, and its abnormally high expression often promotes disease progression[9]. In addition, ASXL1 mutations that frequently occur in MDS were detected in our case and predict an adverse outcome[10]. Therefore, the patient in our report contained "dominant" karyotypes [del(5q)], "inferior" karyotypes [inv(3)] and harmful ASXL1 mutations. However, the prognostic tendency of these patients remains elusive.
Look, she said softly, her eyes directing me to a spot on the floor beside the dresser. To my amazement19, there, as if it had never been removed, stood the old pickle jar, the bottom already covered with coins.
The authors declare that they have no conflict of interest.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
China
Hai-Ping Liang 0000-0001-7537-278X; Xing-Chun Luo 0000-0002-4576-9011; Ya-Li Zhang 0000-0002-4176-9129; Bei Liu 0000-0003-4331-2138.
Gong ZM
A
Gong ZM
 World Journal of Clinical Cases2022年11期
World Journal of Clinical Cases2022年11期
- World Journal of Clinical Cases的其它文章
- Pleomorphic adenoma of the left lacrimal gland recurred and transformed into myoepithelial carcinoma after multiple operations:A case report
- Thyrotoxicosis after a massive levothyroxine ingestion:A case report
- Contrast-enhanced ultrasound manifestations of synchronous combined hepatocellular-cholangiocarcinoma and hepatocellular carcinoma:A case report
- Papillary thyroid microcarcinoma with contralateral lymphatic skip metastasis and breast cancer:A case report
- Ultrasound-guided local ethanol injection for fertility-preserving cervical pregnancy accompanied by fetal heartbeat:Two case reports
- Successful apatinib treatment for advanced clear cell renal carcinoma as a first-line palliative treatment:A case report