
Unilateral adrenal tuberculosis whose computed tomography imaging characteristics mimic a malignant tumor:A case report
2022-06-22 11:27:34HuiLiuTianJiaoTangZhenMeiAnYeRongYu
World Journal of Clinical Cases 2022年17期
lNTRODUCTlON
Tuberculosis(TB)is known to present with varied clinical features,but involvement of the adrenal glands in TB is rare[1].Isolated adrenal TB accounts for under 2% of adrenal incidentalomas[2],while 75%-100% of patients with adrenal TB have bilateral involvement[3-5].As a result,unilateral adrenal TB is considered a rare clinical entity.The computed tomography(CT)imaging characteristics of adrenal TB are significantly different from those of primary tumors,such as small size,low attenuation in the center,and peripheral rim enhancement[3,6,7].Herein,we report an unusual case of unilateral adrenal TB whose imaging characteristics were extremely atypical and suggested a high likelihood of a malignant tumor.Fine-needle aspiration biopsy(FNAB)was used to confirm TB,and prolonged anti-TB treatment was given to stabilize her condition.
CASE PRESENTATlON
Chief complaints
A 42-year-old female was admitted to our department after presenting with a half-year history of osphyalgia.
History of present illness
A 42-year-old female had low back pain for a half year,which was exaggerated when taking a deep breath or lying flat and relieved when standing.She denied frequent micturition,painful urination,fever,hematuria,or pyuria.
The old woman followed the goat into the cave and then, what should she see but the animal giving her milk to a little boy-baby, whilst on the ground near by lay the sad remains25 of the baby s dead mother! Wondering and frightened, the old woman thought at last that this little baby might be a son to her in her old age, and that he would grow up and in time to come be her comfort and support
History of past illness
The patient had a remote history of hypertension.She had been diagnosed with pulmonary and cerebral TB four months before presentation,and she had started a regimen of anti-TB drugs(isoniazid 0.3 g QD,rifampicin 0.45 g QD,ethambutol 0.75 g QD,and ofloxacin 0.5 g QD)upon diagnosis.
Personal and family history
Yu YR and An ZM contributed to the conceptualization;Liu H and Tang TJ collected the information;Liu H wrote the original draft;Yu YR reviewed and edited the manuscript;all authors issued final approval for the version to be submitted.
Physical examination
1.An old queen: We find few widowed queens and good mothers alive in romantic fairy tales. Although she is alive in the tale, her ability to protect her daughter ends as soon as the daughter leaves the kingdom to be married. In essence, the mother is dead as soon as her daughter departs to begin her adult existence.Return to place in story.
Laboratory examinations
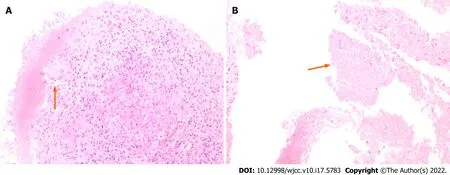
Laboratory tests yielded the following results: plasma total cortisol(8 am),594.6 nmol/L(reference,147.3-609.3 nmol/L);adrenocorticotropic hormone,48.30 ng/L(reference,5.0-78 ng/L);and aldosterone/renin ratio,16.92 ng/dL per ng/mL/h.No abnormalities were observed in the blood and urine catecholamines.Routine blood tests,routine urine tests,and biochemical tests were roughly in the normal range.CT-guided Fine needle aspiration biopsy(FNAB)of the right adrenal gland was performed,and pathological examination detected granulomas and necrosis(Figure 1A and B).
I didn t understand the words, nor did most of us. For we were not the German Afrikakorps but the British Eighth Army---the Desert Rats. Yet we were captivated by this mysterious voice that somehow reached deep into our thoughts and memories.
Imaging examinations
Patients with adrenal TB are usually treated with standard quadruple antitubercular treatment(such as isoniazid,rifampicin,pyrazinamide,and ethambutol)[18-20]for nearly 12 mo or longer.Adverse reactions to anti-TB drugs and their interactions with corticosteroids that are administered for replacement therapy remain challenging[21,22].Firstly,rifampicin increases cortisol catabolism while isoniazid produces increased levels of cortisol
an opposite effect on the enzyme activity 6-Bhydroxylase;secondly,hepatitis,induced by isoniazid and worsened by rifampicin,leads to failure of 11-B-oxo-reductase,which converts cortisone to cortisol;and finally,tuberculous Addison’s disease might require increased amounts of hydrocortisone due to rifampicin administration[23].Up to 70% of patients with active TB have subclinical adrenal insufficiency[24].Anti-TB treatment might cause adrenal crisis[18],and patients should be closely monitored when starting this treatment.Most of the cases demonstrated a good response to anti-TB treatment.Early diagnosis and no delay in treatment initiation contributed to minimizing the high mortality rate[22,25].Addison’s disease usually occurs when more than 90% of adrenal tissue has been destroyed[26].Only a few patients with tuberculous Addison's disease showed recovery of adrenal function[27].
FlNAL DlAGNOSlS
Unilateral adrenal tuberculosis.
TREATMENT
Treatment with 4 anti-TB drugs was continued.
OUTCOME AND FOLLOW-UP
The authors declare that they have no conflict of interest.
They asked him how he had managed to get out of the river, to which he replied: Get along with you--you are no better than silly donkeys without any sense; if you had only drowned me in deeper water I would have returned with three times as many sheep
DlSCUSSlON
Extrapulmonary TB constitutes about 15%-20% of all TB patients[8].The most frequent sites of extrapulmonary TB include the lymph nodes(19%),pleural cavity(7%),gastrointestinal tract(4%),bone(6%),central nervous system(3%),and genitourinary system(1%)[9].Of the 370 reports of extrapulmonary TB in a systematic review spanning 10 years[1],only one case was shown to involve the adrenal gland,which demonstrated adrenal TB as a rare clinical entity.Bilateral involvement usually occurs because of hematogenous and lymph spread from the site of the primary mycobacterial infection to both adrenal glands,which are equally susceptible[10].In our case,adrenal TB(lesions of 1.5 cm to 5 cm)was aggravated while the anti-TB regimen was continued.It is necessary to distinguish adrenal masses from adrenal tumors.Adrenal incidentalomas,adenomas,metastases,adrenocortical carcinomas,myelolipomas,and pheochromocytomas accounted for 41%,19%,10%,9%,and 8%,respectively.The etiologies of these partly depend on the size,such that larger tumors are more likely to be malignant.Adrenal carcinomas and metastases comprise 25% and 18% of lesions and are larger than 6 cm,while adenomas account for only 18%[11].For tumors smaller than 4 cm,adrenal carcinomas comprise 2% and adenomas comprise 65%[11].Untreated TB lesions were smaller than primary tumors(2.8 cm ± 1.3 cm
3.5 cm ± 2.4 cm)[6],while the diameters of benign,malignant pheochromocytoma and adrenocortical carcinoma were 5.7 cm ± 2.3 cm,8.3 cm ± 4.1 cm[12]and 11 cm ± 4 cm[13],respectively.It is difficult to provide evidence with regard to TB based on size(6.0 cm × 4.5 cm)in this case.The CT value,attenuation measurement,and reduced central area(7 ± 4 HU)compared to the peripheral area(32 ± 14 HU)were observed between unenhanced and contrast-enhanced scans in adrenal TB[3].This characteristic of central necrosis surrounded by fibrous and granulomatous inflammatory tissue is much less common in primary adrenal tumors[6],owing to sufficient blood supply in the central area.Pheochromocytoma always has a high enhancement of > 110 HU in the arterial phase[14],while adrenocortical carcinoma is less likely to show an enhancement of >100 HU.In the present case,evidence from images could not rule out a malignant tumor in the adrenal gland.In addition,calcification preferentially occurred in the later stages of adrenal TB than in adrenal tumors(59%
8%),which helped with a proper diagnosis[6].
Then Trusty John was quite delighted, and brought her to the ship; and the King, when he beheld19 her, saw that she was even more beautiful than her picture, and thought every moment that his heart would burst
In addition to the ineffectiveness of FNAB in distinguishing adrenal adenoma from adenocarcinoma[11],it is considered advantageous due to its ease,cost-effectiveness,reduced time consumption,low complication rates,and high accuracy[15-17].It is often used for suspected nonfunctional and nonneoplastic adrenal gland lesions,but not employed for pheochromocytomas[11,17]due to the risk of hemodynamic instability.In the present case,blood pressure was well controlled and had no abnormalities in blood and urine catecholamines,indicating a lower possibility of pheochromocytoma.Therefore,FNAB was performed to obtain histological evidence,which subsequently provides clear evidence regarding targeted therapy.
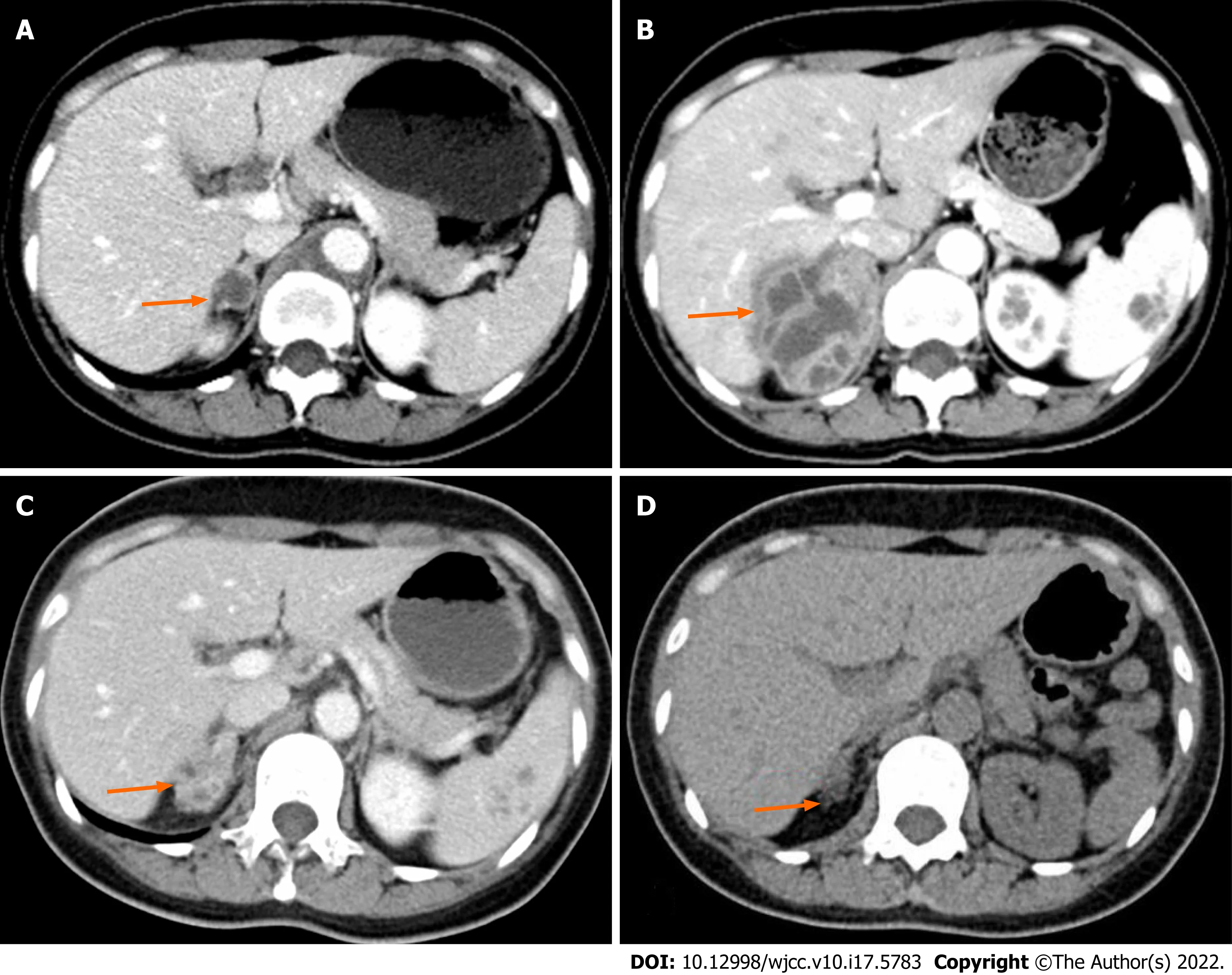
Four months prior to presentation,the patient had undergone an abdominal CT scan,which revealed a 1.5 cm isointense mass in the right adrenal gland(Figure 2A).On presentation to our department,she underwent another abdominal CT scan,which revealed a 6.0 cm × 4.5 cm irregular mass with uneven density in the right adrenal gland,while the left adrenal gland was normal(Figure 2B).
CONCLUSlON
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Physical examination showed nothing special despite percussive pain in the right kidney area.
FOOTNOTES
Her personal and family history were insignificant.
Unilateral adrenal tuberculous infection,although rare,should be considered in patients with unilateral adrenal mass but without Cushing syndrome,primary aldosteronism,or pheochromocytoma.FNAB assists in diagnosing TB,and early initiation and longer duration of anti-TB therapy are crucial to treating patients with unilateral adrenal tuberculous infection.
The patient’s low back pain was relieved,and abdominal CT(Figure 2C)demonstrated a significant reduction of the mass in the right adrenal gland(2.7 cm × 2.4 cm)after 15 mo of anti-TB therapy.Three years later,abdominal CT(Figure 2D)showed a slight enlargement of the right adrenal gland.
This year my youngest son will be a senior in high school. He, too, has now announced that he is too old for notes. But like his older brother and sister before him, he will receive those notes till the day he graduates-and in whatever lunches I pack for him afterwards.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Before this, while he was staying down there, she had told him that she was a daughter of the same troll whom the youth served, and he had shut her up there to keep her away from everyone
China
Hui Liu 0000-0002-9352-3358;Tian-Jiao Tang 0000-0002-4817-2907;Zhen-Mei An 0000-0003-1435-8209;Ye-Rong Yu 0000-0003-0103-0087.
Xing YX
A
Xing YX
1 Edlin GP.Active tuberculosis unrecognised until necropsy.
1978;1: 650-652[PMID: 76179 DOI: 10.1016/s0140-6736(78)91149-2]
2 Lam KY,Lo CY.A critical examination of adrenal tuberculosis and a 28-year autopsy experience of active tuberculosis.
2001;54: 633-639[PMID: 11380494 DOI: 10.1046/j.1365-2265.2001.01266.x]
3 Ma ES,Yang ZG,Li Y,Guo YK,Deng YP,Zhang XC.Tuberculous Addison's disease: morphological and quantitative evaluation with multidetector-row CT.
2007;62: 352-358[PMID: 17466476 DOI: 10.1016/j.ejrad.2006.12.012]
4 Gupta P,Bhalla A,Sharma R.Bilateral adrenal lesions.
2012;56: 636-645[PMID: 23210583 DOI: 10.1111/j.1754-9485.2012.02435.x]
5 Guo YK,Yang ZG,Li Y,Ma ES,Deng YP,Min PQ,Yin LL,Hu J,Zhang XC,Chen TW.Addison's disease due to adrenal tuberculosis: contrast-enhanced CT features and clinical duration correlation.
2007;62: 126-131[PMID: 17182208 DOI: 10.1016/j.ejrad.2006.11.025]
6 Yang ZG,Guo YK,Li Y,Min PQ,Yu JQ,Ma ES.Differentiation between tuberculosis and primary tumors in the adrenal gland: evaluation with contrast-enhanced CT.
2006;16: 2031-2036[PMID: 16435135 DOI: 10.1007/s00330-005-0096-y]
7 Alshahrani MA,Bin Saeedan M,Alkhunaizan T,Aljohani IM,Azzumeea FM.Bilateral adrenal abnormalities: imaging review of different entities.
2019;44: 154-179[PMID: 29938331 DOI: 10.1007/s00261-018-1670-5]
8 Sharma SK,Mohan A,Kohli M.Extrapulmonary tuberculosis.
2021;15: 931-948[PMID: 33966561 DOI: 10.1080/17476348.2021.1927718]
9 Houston A,Macallan DC.Extrapulmonary tuberculosis.
2014;42: 18-22
10 Kissane,John M.Anderson's Pathology.1985
11 Aron D,Terzolo M,Cawood TJ.Adrenal incidentalomas.
2012;26: 69-82[PMID: 22305453 DOI: 10.1016/j.beem.2011.06.012]
12 Khadilkar K,Sarathi V,Kasaliwal R,Pandit R,Goroshi M,Malhotra G,Dalvi A,Bakshi G,Bhansali A,Rajput R,Shivane V,Lila A,Bandgar T,Shah NS.Predictors of malignancy in patients with pheochromocytomas/paragangliomas: Asian Indian experience.
2016;5: 89-97[PMID: 27852633 DOI: 10.1530/EC-16-0086]
13 Zhang HM,Perrier ND,Grubbs EG,Sircar K,Ye ZX,Lee JE,Ng CS.CT features and quantification of the characteristics of adrenocortical carcinomas on unenhanced and contrast-enhanced studies.
2012;67: 38-46[PMID: 21783181 DOI: 10.1016/j.crad.2011.03.023]
14 Northcutt BG,Raman SP,Long C,Oshmyansky AR,Siegelman SS,Fishman EK,Johnson PT.MDCT of adrenal masses: Can dual-phase enhancement patterns be used to differentiate adenoma and pheochromocytoma?
2013;201: 834-839[PMID: 24059372 DOI: 10.2214/AJR.12.9753]
15 Patel S,Jinjuvadia R,Devara A,Naylor PH,Anees M,Jinjuvadia K,Al-Haddad M.Performance characteristics of EUSFNA biopsy for adrenal lesions: A meta-analysis.
2019;8: 180-187[PMID: 30880721 DOI: 10.4103/eus.eus_42_18]
16 Kerimaa P,Marttila A,Hyv?nen P,Ojala R,Lappi-Blanco E,Tervonen O,Blanco Sequeiros R.MRI-guided biopsy and fine needle aspiration biopsy(FNAB)in the diagnosis of musculoskeletal lesions.
2013;82: 2328-2333[PMID: 24099641 DOI: 10.1016/j.ejrad.2013.09.005]
17 Patil R,Ona MA,Papafragkakis C,Duddempudi S,Anand S,Jamil LH.Endoscopic ultrasound-guided fine-needle aspiration in the diagnosis of adrenal lesions.
2016;29: 307-311[PMID: 27366030 DOI: 10.20524/aog.2016.0047]
18 Denny N,Raghunath S,Bhatia P,Abdelaziz M.Rifampicin-induced adrenal crisis in a patient with tuberculosis: a therapeutic challenge.
2016;2016[PMID: 27899384 DOI: 10.1136/bcr-2016-216302]
19 Shrestha B,Omran A,Rong P,Wang W.Successfully treated unusual case of primary adrenal and spinal tuberculosis with three years follow up.
2014;17: 108[PMID: 25018843 DOI: 10.11604/pamj.2014.17.108.2575]
20 Manso MC,Rodeia SC,Rodrigues S,Domingos R.Synchronous presentation of two rare forms of extrapulmonary tuberculosis.
2016;2016: 10.1136/bcr-2015[PMID: 27090536 DOI: 10.1136/bcr-2015-212917]
21 Thijs E,Wierckx K,Vandecasteele S,Van den Bruel A.Adrenal insufficiency,be aware of drug interactions!
2019;2019[PMID: 31581123 DOI: 10.1530/EDM-19-0062]
22 Shah M,Reed C.Complications of tuberculosis.
2014;27: 403-410[PMID: 25028786 DOI: 10.1097/QCO.0000000000000090]
23 Kusuki K,Watanabe S,Mizuno Y.Tuberculous Addison's disease with increased hydrocortisone requirements due to administration of rifampicin.
2019;12[PMID: 30872343 DOI: 10.1136/bcr-2018-228293]
24 Sarin BC,Sibia K,Kukreja S.Study of adrenal function in patients with tuberculosis.
2018;65: 241-245[PMID: 29933867 DOI: 10.1016/j.ijtb.2017.08.033]
25 Zhao N,Gao Y,Ni C,Zhang D,Zhao X,Li Y,Sun B.An autopsy case of unexpected death due to Addison's disease caused by adrenal tuberculosis.
2021;26: 137[PMID: 34863306 DOI: 10.1186/s40001-021-00611-w]
26 Alevritis EM,Sarubbi FA,Jordan RM,Peiris AN.Infectious causes of adrenal insufficiency.
2003;96: 888-890[PMID: 14513986 DOI: 10.1097/01.SMJ.0000073269.49575.DF]
27 Penrice J,Nussey SS.Recovery of adrenocortical function following treatment of tuberculous Addison's disease.
1992;68: 204-205[PMID: 1589379 DOI: 10.1136/pgmj.68.797.204]
 World Journal of Clinical Cases2022年17期
World Journal of Clinical Cases2022年17期
- World Journal of Clinical Cases的其它文章
- Repetitive transcranial magnetic stimulation for post-traumatic stress disorder:Lights and shadows
- Response to dacomitinib in advanced non-small-cell lung cancer harboring the rare delE709_T710insD mutation:A case report
- Loss of human epidermal receptor-2 in human epidermal receptor-2+breast cancer after neoadjuvant treatment:A case report
- Tumor-like disorder of the brachial plexus region in a patient with hemophilia:A case report
- High-frame-rate contrast-enhanced ultrasound findings of liver metastasis of duodenal gastrointestinal stromal tumor:A case report and literature review
- Gitelman syndrome:A case report