
Non-alcoholic Wernicke encephalopathy in an esophageal cancer patient receiving radiotherapy:A case report
2022-06-22 11:27:38YeZhangLeiWangJinJiangWenYuChen
World Journal of Clinical Cases 2022年17期
lNTRODUCTlON
Wernicke encephalopathy is an acute or subacute neuropsychiatric disorder secondary to thiamine(vitamin B1)deficiency.It is characterized by the classical triad of ophthalmoplegia,gait ataxia,and altered mental status[1-3],which,however,presents in only 10%-16% of the cases[1,3,4].Chronic alcoholism is the most common predisposing factor for thiamine deficiency,followed by malnutrition or decreased thiamine absorption secondary to hyperemesis gravidarum,gastrointestinal disease,prolonged fasting,prolonged parenteral nutrition support,hemodialysis,or malignant disease[5-9].Compared to alcoholic Wernicke encephalopathy,non-alcoholic Wernicke encephalopathy may be prone to diagnostic delays owing to its atypical clinical presentation and the interval between symptom onset and clinical diagnosis[10].To the best of our knowledge,there have been no reports of Wernicke encephalopathy occurring in cases of esophageal cancer.Moreover,the most common predisposing factors for non-alcoholic Wernicke encephalopathy in cancer include gastrectomy,chemotherapy,or end-stage of life;radiotherapy is rarely documented.Herein,we describe the first case of non-alcoholic Wernicke encephalopathy accompanying esophageal cancer in a patient receiving radiotherapy.
CASE PRESENTATlON
Chief complaints
A 64-year-old man was admitted to our hospital with complaints of progressive difficulty in swallowing.
History of present illness
The patient’s symptoms started 2 mo prior,with recurrent episodes of difficulty in swallowing.He could ingest fluids with ease,but semi-liquid foods only with difficulty.He also reported feeling fatigued.
History of past illness
There was no remarkable medical history.He had a history of smoking for 20 years,but no history of alcohol or drug consumption.
Personal and family history
The patient had a disease-free personal and family history.
Physical examination
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
The troll said that he would always be welcome; he had served him faithfully for the three years they had agreed upon, and he could make no objections to his leaving now
Laboratory examinations
Before long the sexton25 came by and saw his master, the parson, running behind three girls. He was astonished at this and called out, Hi, your reverence8, whither away so quickly? do not forget that we have a christening to-day! and running after him he took him by the sleeve, but was also held fast to it.
Imaging examination
An esophagogastroscopy revealed a significant esophageal tumor located 26-33 cm from the upper incisors,and biopsy results indicated squamous cell carcinoma.Chest contrast-enhanced computed tomography(CT)revealed thickening of the middle and lower esophageal wall with luminal stenosis.The abdominal CT findings were unremarkable.As per the eighth edition of the Union for International Cancer Control staging,the final diagnosis was locally advanced esophageal squamous cell carcinoma,clinical stage cT3N2M0(stage IIIB).
Further diagnostic work-up
the Scientific Technology Plan Program for Healthcare in Zhejiang Province,No.2021KY1100;and the Key Discipline of Jiaxing General Practice Medicine Construction Project,No.2019-fc-03.
FlNAL DlAGNOSlS
At first,the signs and symptoms rendered cerebrovascular disease or metastatic brain tumors as the most probable diagnosis.However,after combining the clinical manifestations and typical brain MRI findings,a final diagnosis of Wernicke encephalopathy secondary to thiamine deficiency was made.
TREATMENT
We started immediate intravenous thiamine replacement therapy at a dose of 500 mg/d for 3 d,followed by 200 mg for a week,and one tablet of 100 mg oral thiamine per day.
There was in the town a large dark gate, through which she had to pass night and morning with the geese; would he kindly20 hang up Falada s head there, that she might see it once again? The slaughterer said he would do as she desired, chopped off the head, and nailed it firmly over the gateway21
OUTCOME AND FOLLOW-UP
Our case illustrates that Wernicke encephalopathy can occur in non-alcoholic patients with esophageal cancer.Clinicians should keep in mind that patients with esophageal cancer and underlying malnutrition are at a high risk of Wernicke encephalopathy.Nutritional evaluation and diagnosis are necessary at the earliest possible instance.Any clinical suspicion of Wernicke encephalopathy should be treated promptly with thiamine supplementation to prevent permanent neurological damage.
DlSCUSSlON
Wernicke encephalopathy is a neurological disorder resulting from the deficiency of thiamine,and is commonly related to the chronic abuse of alcohol[1,2].Recently,the incidence of non-alcoholic Wernicke encephalopathy has been increasing,and malignancy is one of the attributable causes.The most common type of malignancy reported with non-alcoholic Wernicke encephalopathy is haematological,followed by gastrointestinal neoplasms.There have been no studies reporting cases of Wernicke encephalopathy in patients with esophageal cancer thus far.
Thiamine cannot be synthesized in the human body,and hence is mainly derived from food.Therefore,any kind of malnutrition lasting for more than 3-4 wk depletes the thiamine reserve[11].Esophageal cancer is often accompanied by malnutrition due to dysphagia and declined appetite.The potential for subclinical thiamine deficiency should be considered despite the absence of changes in the mental state[12].
In patients with cancer,Wernicke encephalopathy can occur after surgery,during chemotherapy,or at the end of life.It is extremely rare in patients receiving radiotherapy based on existing reports,and there is no guidance on whether radiotherapy can accelerate thiamine deficiency.It needs to be confirmed by more studies in the future.We concluded that chronic malnutrition caused by repeated dysphagia and vomiting was the main reason for Wernicke encephalopathy in our patient.Therefore,a total nutritional evaluation and prophylactic thiamine supplementation are major preventative and therapeutic measures for impaired dietary intake in non-surgical esophageal cancer patients from the time of diagnosis,especially before radiotherapy.
The classically described clinical triad of ophthalmoplegia,ataxia,and mental disturbances is often absent in Wernicke encephalopathy.Therefore,a non-alcoholic patient presenting with atypical clinical manifestations can frequently be misdiagnosed.Day
[13]reported underdiagnosis rates of 68% and 94% in alcoholic and non-alcoholic Wernicke encephalopathy,respectively.Delayed diagnosis and treatment can lead to the progression of the disease.As per recommendations,the diagnosis of Wernicke encephalopathy is made when two of the following signs are present:(1)Dietary deficiencies;(2)eye signs;(3)cerebellar dysfunction;and(4)either an altered mental state or a mild memory impairment[8].In our patient,the clinical suspicion of Wernicke encephalopathy was delayed as the patient was a non-alcoholic,and disturbance of consciousness was the only manifestation.
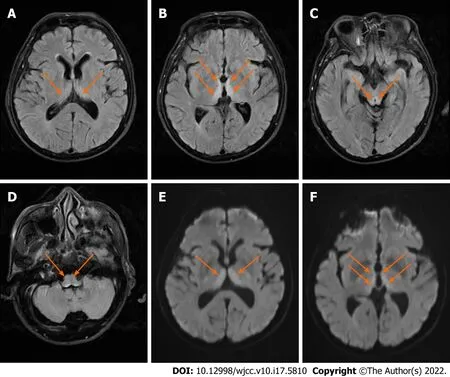
MRI is currently considered the most valuable method for the diagnosis of non-alcoholic Wernicke encephalopathy,especially the FLAIR sequence which has a 93% specificity[14].The common MRI findings for non- alcoholic Wernicke encephalopathy are hyperintense signals in the dorsal medial thalamic nuclei,periaqueductal gray area,and the third or fourth ventricles as seen on DWI,T2-weighted imaging,and FLAIR sequence[1,11,15,16].In our patient,there were no obvious abnormalities on CT,but typical findings were detected on MRI,similar to that in current literature reports.Therefore,it is important to detect Wernicke encephalopathy in the early stages of the disease using MRI,since CT has a low sensitivity in the acute phase.Wernicke encephalopathy should be considered as one of the common differential diagnoses when patients develop unexplained altered mental status during radiotherapy while admitted to the Department of Oncology.
Blood biochemistry revealed mild hypoproteinemia(36 g/L).The results of routine blood and urine tests and arterial blood gas analysis were normal.
Thiamine plays a major role in glucose metabolism.The administration of glucose may thus accelerate the consumption of thiamine and hasten the onset of Wernicke encephalopathy.Our patient received no thiamine,but received continuous glucose solutions as a part of his parenteral nutrition supplement,which is consistent with that reported in the literature[17-19].Therefore,glucose should be used with caution.
Once a diagnosis of Wernicke encephalopathy is suspected,it is advisable to administer thiamine as early as possible to prevent permanent neurological damage[20].Although there are no published guidelines for the treatment of Wernicke encephalopathy in non-alcoholics patients,intravenous thiamine supplementation in the acute stage is currently recommended.Several researchers recommend that patients be treated with a high-dose thiamine regimen,consisting of 500 mg thiamine every 8 h intravenously for at least 2-3 d,followed by 250 mg thiamine once a day intravenously for 5 d[21].In our patient,there was significant improvement in his mental state,but mild cognitive impairment remained due to the late diagnosis of the condition.Therefore,our objective in reporting this case is to emphasize the importance of early nutritional evaluation and diagnosis,so that lasting neurological sequelae can be avoided in patients with Wernicke encephalopathy.
CONCLUSlON
The patient regained consciousness within 3 d.After 5 d,his mental status improved,and he could understand simple commands.At discharge,the patient’s neurological symptoms were improved significantly.Neurological examination at the 2-mo follow-up was normal,except for mild memory impairment.
Annie Mae was my in-law’s maid. She prepared and served meals in her quiet, gentle way and then returned to the kitchen to read her Bible while we ate. She was a dedicated3 and devoted4 Christian5. To me, she reflected the fruit of the Holy Spirit as found in Galatians 5:22-23. I found this increasingly true even though I came to know her more by observation than by conversation.
Then the curtain fell before it once more, and the Prince, after many ceremonies, was presented with a raven which perched upon his wrist, and was conducted slowly back to the iron gate
FOOTNOTES
Zhang Y and Jiang J were the patient’s doctors,reviewed the literature,and contributed to manuscript drafting;Wang L reviewed the literature and contributed to manuscript drafting;Chen WY analyzed and interpreted the imaging findings;Zhang Y and Wang L were responsible for the revision of the manuscript for important intellectual content;all authors issued final approval for the version to be submitted.
The patient refused surgery or chemotherapy.In order to alleviate dysphagia due to malignant esophageal stenosis,he received 60 Gy of local radiotherapy in 30 fractions without concurrent chemotherapy.Repeated vomiting and dorsalgia occurred during radiotherapy,without diarrhea.A parenteral nutritional supplement including high glucose but no thiamine was administered.On day 8 of radiotherapy,the dysphagia status was markedly improved.From day 10 of radiotherapy,the patient gradually displayed apathy,disorientation,and passivity;was disinterested in his surroundings;and slept abundantly.On neurological examination,he was minimally responsive to verbal and painful stimuli,uncooperative for the finger-to-nose examination,had a slow pupillary response to light,and a Glasgow coma scale score of 10.This was followed by the onset of lethargy on day 12 of radiotherapy.An emergency brain CT scan performed immediately was normal.Brain magnetic resonance imaging(MRI)showed bilateral symmetrical hyperintensities in the dorsal thalamus,the periventricular region of the third ventricle,and around the cerebral aqueduct as seen on T2-weighted imaging,fluidattenuated inversion recovery(FLAIR),and diffusion-weighted imaging(DWI)(Figure 1).
He sent for his Grand Wazeer and told him that he was going on one of his lonely expeditions, and that the Wazeer must invent some excuse to account for his absence
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Dr.Zhang reports grants from Scientific Technology Plan Program for Healthcare in Zhejiang Province during the conduct of the study.
The patient was emaciated and had a body mass index of 19.88 kg/m
.There were no mental status changes,cerebellar symptoms,or abnormal eye movements.No clinical ophthalmoplegia or encephalopathy was detected.The other items of the physical examination were normal.
One day he went again to the king and said, These eleven brothers have now procured19 the dove and the boar, but they can do much more than that; I know they have said that if they liked they could get for the king a lamp that can shine over seven kingdoms
The messenger awoke with such a start, and when he saw that the hour had almost run out he snatched up the answer and rushed back with such speed that the clock had not yet struck when he entered the palace
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Ye Zhang 0000-0001-9740-1502;Lei Wang 0000-0002-0246-1607;Jin Jiang 0000-0002-2518-0162;Wen-Yu Chen 0000-0002-4930-9530.
Yan JP
Wang TQ
Yan JP
1 Sinha S,Kataria A,Kolla BP,Thusius N,Loukianova LL.Wernicke Encephalopathy-Clinical Pearls.
2019;94: 1065-1072[PMID: 31171116 DOI: 10.1016/j.mayocp.2019.02.018]
2 Vogrig A,Zanoni T,Moretto G.Nystagmus and Lower Extremity Hyperalgesia After Colectomy.
2016;316: 1488-1489[PMID: 27727364 DOI: 10.1001/jama.2016.13658]
3 Harper CG,Giles M,Finlay-Jones R.Clinical signs in the Wernicke-Korsakoff complex: a retrospective analysis of 131 cases diagnosed at necropsy.
1986;49: 341-345[PMID: 3701343 DOI: 10.1136/jnnp.49.4.341]
4 Zuccoli G,Gallucci M,Capellades J,Regnicolo L,Tumiati B,Giadás TC,Bottari W,Mandrioli J,Bertolini M.Wernicke encephalopathy: MR findings at clinical presentation in twenty-six alcoholic and nonalcoholic patients.
2007;28: 1328-1331[PMID: 17698536 DOI: 10.3174/ajnr.A0544]
5 Arita T,Komatsu S,Kosuga T,Konishi H,Morimura R,Murayama Y,Kuriu Y,Shiozaki A,Ikoma H,Nakanishi M,Ichikawa D,Okamoto K,Otsuji E.[Laparoscopic Gastrostomy for a Patient with Wernicke's Encephalopathy after Gastrectomy--A Case Report with a Literature Review].
2015;42: 2037-2039[PMID: 26805256]
6 D'Ettorre M,Rosa F,Coppola A,Mele C,Alfieri S,Doglietto GB.Postoperative suspected Wernicke's encephalopathy in a rectal cancer patient:A case report.
2012;28: 290-292[PMID: 23413765]
7 Zafar A.Wernicke's encephalopathy following Roux en Y gastric bypass surgery.
2015;36: 1493-1495[PMID: 26620994 DOI: 10.15537/smj.2015.12.12643]
8 Galvin R,Br?then G,Ivashynka A,Hillbom M,Tanasescu R,Leone MA;EFNS.EFNS guidelines for diagnosis,therapy and prevention of Wernicke encephalopathy.
2010;17: 1408-1418[PMID: 20642790 DOI: 10.1111/j.1468-1331.2010.03153.x]
9 Sriram K,Manzanares W,Joseph K.Thiamine in nutrition therapy.
2012;27: 41-50[PMID: 22223666 DOI: 10.1177/0884533611426149]
10 Dhir S,Tarasenko M,Napoli E,Giulivi C.Neurological,Psychiatric,and Biochemical Aspects of Thiamine Deficiency in Children and Adults.
2019;10: 207[PMID: 31019473 DOI: 10.3389/fpsyt.2019.00207]
11 Zuccoli G,Pipitone N.Neuroimaging findings in acute Wernicke's encephalopathy: review of the literature.
2009;192: 501-508[PMID: 19155417 DOI: 10.2214/AJR.07.3959]
12 Yoshioka A,Sato I,Onishi H,Ishida M.Subclinical thiamine deficiency identified by pretreatment evaluation in an esophageal cancer patient.
2021;75: 564-566[PMID: 32895510 DOI: 10.1038/s41430-020-00735-y]
13 Day GS,del Campo CM.Wernicke encephalopathy: a medical emergency.
2014;186: E295[PMID: 24016788 DOI: 10.1503/cmaj.130091]
14 Guler A,Alpaydin S,Sirin H,Calli C,Celebisoy N.A non-alcoholic Wernicke's encephalopathy case with atypical MRI findings: Clinic
radiology.
2015;28: 474-477[PMID: 26306933 DOI: 10.1177/1971400915598080]
15 Manzo G,De Gennaro A,Cozzolino A,Serino A,Fenza G,Manto A.MR imaging findings in alcoholic and nonalcoholic acute Wernicke's encephalopathy: a review.
2014;2014: 503596[PMID: 25050351 DOI: 10.1155/2014/503596]
16 Zuccoli G,Santa Cruz D,Bertolini M,Rovira A,Gallucci M,Carollo C,Pipitone N.MR imaging findings in 56 patients with Wernicke encephalopathy: nonalcoholics may differ from alcoholics.
2009;30: 171-176[PMID: 18945789 DOI: 10.3174/ajnr.A1280]
17 Jin J,Mulesa L,Carrilero Rouillet M.Trace Elements in Parenteral Nutrition: Considerations for the Prescribing Clinician.
2017;9[PMID: 28452962 DOI: 10.3390/nu9050440]
18 Harada D,Nakayama M.Influence of Glucose Dosage in Parenteral Nutrition on Body Thiamine Levels in Rats.
2019;16: 1-7[PMID: 30662322 DOI: 10.7150/ijms.28756]
19 Gralak MA,D?bski B,Drywień M.Thiamine deficiency affects glucose transport and β-oxidation in rats.
2019;103: 1629-1635[PMID: 31259440 DOI: 10.1111/jpn.13146]
20 Smith H,McCoy M,Varughese K,Reinert JP.Thiamine Dosing for the Treatment of Alcohol-Induced Wernicke's Encephalopathy: A Review of the Literature.
2021;37: 107-113[PMID: 34752552 DOI: 10.1177/8755122520962859]
21 Ho PA,York A,Rustad JK,Felde A,Stern TA.Non-Alcohol-Related Wernicke's Encephalopathy: Diagnosis and Treatment.
2021;23[PMID: 34651469 DOI: 10.4088/PCC.21f02968]
 World Journal of Clinical Cases2022年17期
World Journal of Clinical Cases2022年17期
- World Journal of Clinical Cases的其它文章
- Repetitive transcranial magnetic stimulation for post-traumatic stress disorder:Lights and shadows
- Response to dacomitinib in advanced non-small-cell lung cancer harboring the rare delE709_T710insD mutation:A case report
- Loss of human epidermal receptor-2 in human epidermal receptor-2+breast cancer after neoadjuvant treatment:A case report
- Tumor-like disorder of the brachial plexus region in a patient with hemophilia:A case report
- High-frame-rate contrast-enhanced ultrasound findings of liver metastasis of duodenal gastrointestinal stromal tumor:A case report and literature review
- Gitelman syndrome:A case report