
Application of a new anatomic hook-rod-pedicle screw system in young patients with lumbar spondylolysis:A pilot study
2022-06-22 11:27:14DuanMingLiYongChaoLiWeiJiangBaoGanPeng
World Journal of Clinical Cases 2022年17期
lNTRODUCTlON
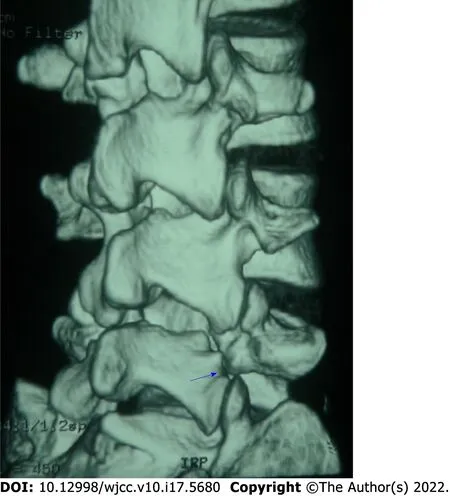
Spondylolysis is a bony defect in the pars interarticularis of a vertebra,which can be complete or incomplete,bilateral or unilateral and more commonly complete bilateral(Figure 1)[1-3].It is often asymptomatic but quite common in young people and adolescents with low back pain[4,5].These patients are usually treated conservatively with analgesics,lumbar orthoses,limitation of movement and physical therapy,and surgery is performed only when the pain persists[6,7].For this young group of patients,spinal surgeons have paid more and more attention to how to minimize the impact on the range of motion of the spine and prevent the adjacent segments from producing excessive mechanical stress[8,9],so as to turn their attention to repairing the pars interarticularis,bone grafting and restoring the stability of the posterior arch[10,11].Because the most common lesion of spondylolysis is acquired pseudarthrosis,bone grafting combined with internal fixation is a treatment that does not require arthrodesis.There are multiple reports on direct pars repair techniques in the literature[12-15].Two common methods are:(1)Direct repair using a lamina/pars compression screw through the isthmic defect;and(2)Compression of the isthmic defect using a set of pedicle screw,rod and laminar hook assembly within the same segment.
More and more surgeons repair lumbar isthmus defects with bone grafting and the pedicle screwlaminar hook system to treat young patients with lumbar spondylolysis because of its firm fixation and good clinical effect[16-18].However,the pedicle screw-laminar hook systems currently in use are not specifically designed for the treatment of lumbar spondylolysis.It has some disadvantages,such as incomplete matching between hook and lamina,difficulty in installation between rod and pedicle screw and large trauma.Complete exposure of the lamina is usually required,resulting in excessive paraspinal soft tissue dissection.To this end,we designed a new anatomical hook-rod-pedicle screw system for lumbar spondylolysis and observed its clinical efficacy.
When he had gone quite out of sight the girl climbed down from the tree and went to the rock, which she pushed aside, and entered the opening before her
MATERlALS AND METHODS
Patient selection
From April 2017 to July 2018,15 men with an average age of 22(18-30 years)participated in the study.There were 11 cases of single segment,including L4(1 case)and L5(10 cases)and 4 cases of double segments,including L3 and L5(1 case)and L4 and L5(3 cases).All cases were bilateral isthmus defects.Inclusion criteria were:(1)The patient presented with severe low back pain and limited lumbar function but no radiating pain(sciatica)in the lower extremities;(2)Computed tomography(CT)of the lumbar spine showed spondylolysis but no spina bifida or missing lamina,and dynamic lumbar radiographs showed no lumbar instability and spondylolisthesis;(3)At isthmic defect and adjacent levels,there was no disc degeneration on magnetic resonance imaging(MRI);(4)Conservative treatment,such as restriction of movement,oral anti-inflammatory analgesics and physiotherapy for 3-6 mo,did not relieve symptoms;and(5)Positive diagnosis test(low back pain disappeared after injection of small dose local anesthetics into the isthmus defect site).Exclusion criteria were metabolic diseases or chronic inflammatory diseases,such as arthrolithiasis,rheumatoid arthritis or ankylosing spondylitis.Physical examination revealed limited lumbar motion,tenderness above and/or adjacent spinous processes and normal motor,sensory and tendon reflexes in both lower extremities.
The study was approved by the ethical review committee from The Third Medical Centre of Chinese PLA General Hospital,and the study was in accordance with the Helsinki Declaration.All patients gave informed written consent.
Surgical procedure
The application of isthmus debridement,bone grafting and anatomical hook-rod-pedicle screw system fixation in young patients with lumbar spondylolysis has the advantages of less trauma,a simple operation and satisfactory curative effect.However,it is not suitable for the cases of lumbar spondylolysis with spondylolisthesis.In addition,it is also not suitable for the cases with missing lamina,bone dysplasia and lumbar disc degenerative diseases.This new hook-rod-pedicle screw system is undergoing biomechanical testing and has been patented in China(Patent No.: ZL201721043286.7).This is a small sample observation study,and further large sample and prospective studies are needed to prove the superiority and reliability of the system.
The contralateral anatomical hook-rod-pedicle screw was installed in the same way.After the installation of both sides,there was no loosening of the hook-rod-pedicle screw system and no movement of bone graft.Then the wound was rinsed with saline,the drainage tube was placed,and the incision was closed layer by layer.The average intraoperative blood loss was 40 mL(28-56 mL).On the second day after the operation,the drainage tube was pulled out,and the patient put on a lumbar brace and got out of bed for low back muscle function exercise.Three months after the operation,the brace can be removed for normal activity and exercise.
Clinical and radiologic assessments
The visual analog scale(VAS)score(in the range of 0 = no pain to 10 = worst pain)was used to evaluate the severity of back pain and donor area pain.The Oswestry disability index(ODI)was used for functional assessment.The measures were recorded preoperatively and 3,6,12 and 24 mo after surgery.Functional status was qualified as“excellent,”“good,”“fair”and“poor”according to the Modified Macnab criteria[19]and recorded at 3,6,12 and 24 mo postoperatively.
Joyce Thomas comments on the trickery and imagery of the bone. The bone provides the imagery of deprivation112 and starvation, one of the primary themes of the tale. Also, the bone Hansel uses imitates the fate awaiting his flesh (the bone could well be the gnawed113 remains114 of the cage s previous occupant) (Thomas 1989).Return to place in story.
Lumbar plain radiographs,CT and MRI were re-examined at 3,6,12 and 24 mo after operation.Lumbar plain radiographs were used to evaluate whether the internal fixation was loose and broken.CT was used to evaluate the fusion of the isthmic fracture and the osteogenesis of the iliac crest donor site.MRI was used to evaluate the degeneration of the intervertebral disc in the corresponding segment of lumbar spondylolysis.
Look, she said softly, her eyes directing me to a spot on the floor beside the dresser. To my amazement19, there, as if it had never been removed, stood the old pickle jar, the bottom already covered with coins.
Statistical analysis
Data were expressed as the mean ± standard error of the mean.Statistical analyses were carried out using SPSS 22.0(IBM Corporation,Armonk,NY,United States).The VAS score and ODI before and after operation were compared using the paired
-test.The significance level was set to 0.05.
RESULTS
During the follow-up period of 24 mo,no patient developed sciatica or motor or sensory disturbance.The VAS score of low back pain and ODI score at 3,6,12 and 24 mo postoperatively significantly improved compared with those before surgery(
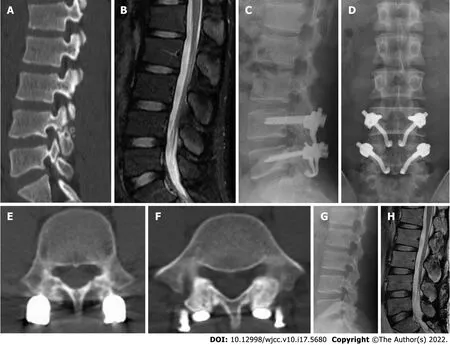
< 0.05,Table 1).At 24 mo after operation,the VAS score of low back pain decreased from 6.73 ± 0.88 preoperatively to 0.73 ± 0.59 postoperatively,and the ODI score decreased from 58.20 ± 8.99 preoperatively to 7.87 ± 4.97 postoperatively(Table 1).CT showed bilateral isthmus bone fusion in 14 cases and unilateral isthmus bone fusion in 1 case.The signs of intervertebral discs in diseased and adjacent segments had no change on MRI.The VAS score of donor site pain was 0.20 ± 0.41.Allogeneic bone filling in the bone donor site showed osteogenesis(Figure 3).According to the Modified Macnab standard,the excellent and good rate of operation was 100% at 24 mo follow-up(Table 2).A typical case was shown in Figure 4.
As his car passed, one child appeared, and a brick smashed into the Jag s side door. He slammed on the brakes and spun3 the Jag back to the spot from where the brick had been thrown.



DlSCUSSlON
Lumbar spondylolysis is one of the common causes of low back pain in adolescents[4].The incidence rate is 3%-10% in adolescents and 6% in adults[20,21].More than 80% of lumbar spondylolysis appears in L4 and L5[4].Patients with lumbar spondylolysis mostly like sports or engage in sports,dancing and other industries.The specific cause of spondylolysis may be stress fractures caused by long-term fatigue on the basis of isthmic dysplasia.For the treatment of symptomatic lumbar spondylolysis in adolescents,active measures should be taken to avoid further problems such as intervertebral disc degeneration,herniation,lumbar instability or spondylolisthesis.If early diagnosis of lumbar spondylolysis is made in adolescents,measures such as wearing a lumbosacral brace and restricting movement will most likely result in isthmic healing[7],but those who do not heal should be actively treated by surgery.The main indication for surgical repair of lumbar spondylolysis is that low back pain is not relieved after at least 6 mo of non-surgical treatment,including activity modification,bracing andphysical therapy.Aggravation of pain,deterioration of neurological symptoms and progressive listhesis also are indications for surgical consideration.In the present study,our patient group,due to severe low back pain,failure of conservative treatment for more than 3 mo,isthmus dissection,osteosclerosis and nonunion,needed surgical treatment.
It was a luxury the ragtag team obviously could not afford. Well, we ended up walloping them. We took every weight class. And as each of their boys got up from the mat, he swaggered around in his tatters with false bravado8, a kind of street pride that couldn t acknowledge defeat.
There are many surgical methods for lumbar spondylolysis.In 1968,Kimura[22]described an isolated bone graft that directly repaired the isthmus defect without internal fixation and retained segmental activity but required a postoperative cast and long bed rest.Later,Scott[23]proposed the use of wire under the lamina and transverse processes,which has been improved by several authors over the years[24,25].In 1970,Buck[26]first used screw internal fixation and bone grafting to repair defects directly,and subsequently other approaches with special constructs and temporary fixations were reported[27,28].There were also posterolateral bone graft fusion,cross-segmental pedicle screw fixation and other methods.Patients with spondylolisthesis or disc herniation can be treated with pedicle screw fixation and interbody fusion[29].
The treatment of young patients with lumbar spondylolysis with isthmus debridement,bone grafting and pedicle screw laminar hook fixation has achieved satisfactory results[16-18],which proves that the pedicle screw-laminar hook system has strong fixation and is conducive to bone graft fusion.It is an intrasegmental fixation and does not affect the lumbar interbody movement and the kinematics of the adjacent segment.Studies[30-32]have reached a consensus that the lumbar intramuscular approach can reduce the dissection of paravertebral muscles,reduce the denervation of paravertebral muscles,preserve the structure of muscle ligament complex,reduce postoperative pain and recover quickly.However,the current pedicle screw-laminar hook fixation system is not specifically designed for lumbar spondylolysis but mainly for the correction of scoliosis.Before the hook is installed,the muscles around the spinous process and lamina need to be separated,resulting in severe tissue damage.At the same time,the installation of the system is difficult because the lamina,hook and pedicle screw are not on the same plane.
To investigate the clinical effects of a new anatomical hook-rod-pedicle screw system in the treatment of lumbar spondylolysis in young adults.
In this study,15 cases of young patients with lumbar spondylolysis were treated with isthmus repair,bone grafting and anatomical hook-rod-pedicle screw fixation and achieved satisfactory results.At the same time,the injury was small,and the operation was simple and convenient.However,in all 15 patients with lumbar spondylolysis who underwent repair of the isthmic defect,1 patient with L5 bilateral isthmic defect had no bone healing on one side.Most of the isthmus defects occurred in preschool,and a few occurred in adulthood.Isthmus rupture will no longer occur in adulthood.After the occurrence of lumbar isthmus defect,the defect usually does not heal spontaneously.In this way,the broken ends of bone on both sides of the defect will atrophy and harden.In this case,nonunion after repair of the isthmus defect is a common complication.Because this is an intrasegmental fixation,the implant usually does not need to be removed.If unilateral nonunion occurs,the implant must not be removed.
When she came in she smelled around her and went all about the hut, tapping with the pestle; but pry37 and examine as she might, again she could see no reason to find fault and was angrier than ever. She clapped her hands and shouted:
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.This study was approved by the ethics committee of The Third Medical Centre of Chinese PLA General Hospital.
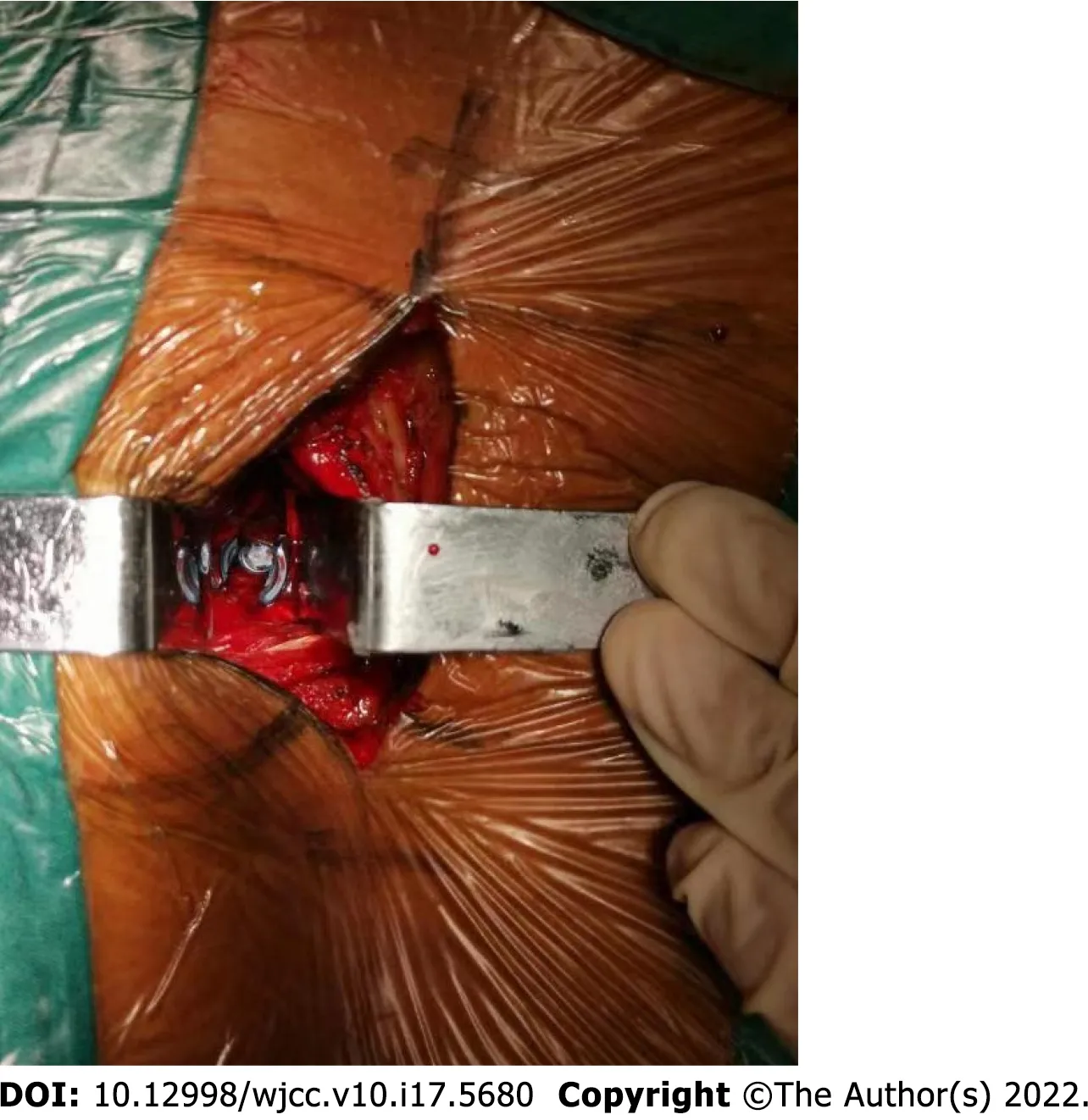
The patient was placed prone on the operating table under general endotracheal anesthesia,carefully cushioning all pressure points and keeping the neck in a neutral position.A midline incision was made,cutting the skin to the deep fascia layer.The deep fascia was cut longitudinally 1.5 cm outside the midline.The longissimus-multifidus muscle interval was bluntly dissected with a finger to avoid unnecessary tissue damage(Figure 2).Through the intermuscular approach,the isthmic defect site and the insertion point of the pedicle screw were exposed,and the fibrous tissue at the defect area was removed.A high-speed burr was used to debride sclerotic surfaces until bleeding bone surface was seen in the fractured pars.Gross motion was noted in the fissure area of the isthmus.Care was taken not to injure the facet joint capsule.Then a universal multiaxial pedicle screw was inserted into the corresponding vertebral body.Autogenous bone graft was obtained from the posterior superior iliac crest and implanted into the isthmus defect site,and the donor area of the posterior superior iliac crest was filled with allogeneic bone.After releasing the lower edge of the lamina with the ligamentum flavum stripper,the middle part of the hook rod was clamped with the rod holding forceps,and the hook could easily hook the lower edge of the lamina.The rod end of the anatomical hook was connected with the multiaxial pedicle screw.The construct was then loaded with compression force and tightened.
CONCLUSlON
Compared with the use of the traditional instrument,the application of this new anatomical hook-rodpedicle screw system to treat young patients with lumbar spondylolysis has the advantages of less trauma,a simple operation and satisfactory clinical effects.
ARTlCLE HlGHLlGHTS
Research background
The pedicle screw-laminar hook system has strong fixation and is conducive to bone graft fusion for lumbar spondylolysis.However,the current pedicle screw-laminar hook fixation system is not specifically designed for lumbar spondylolysis.
Research motivation
Informed written consent was obtained from the patients for publication of this manuscript and any accompanying images.
Something in her eyes had changed, too. They were brighter and filled with the wonder of being alive. It was as though that empty place in her heart had been filled.
Research objectives
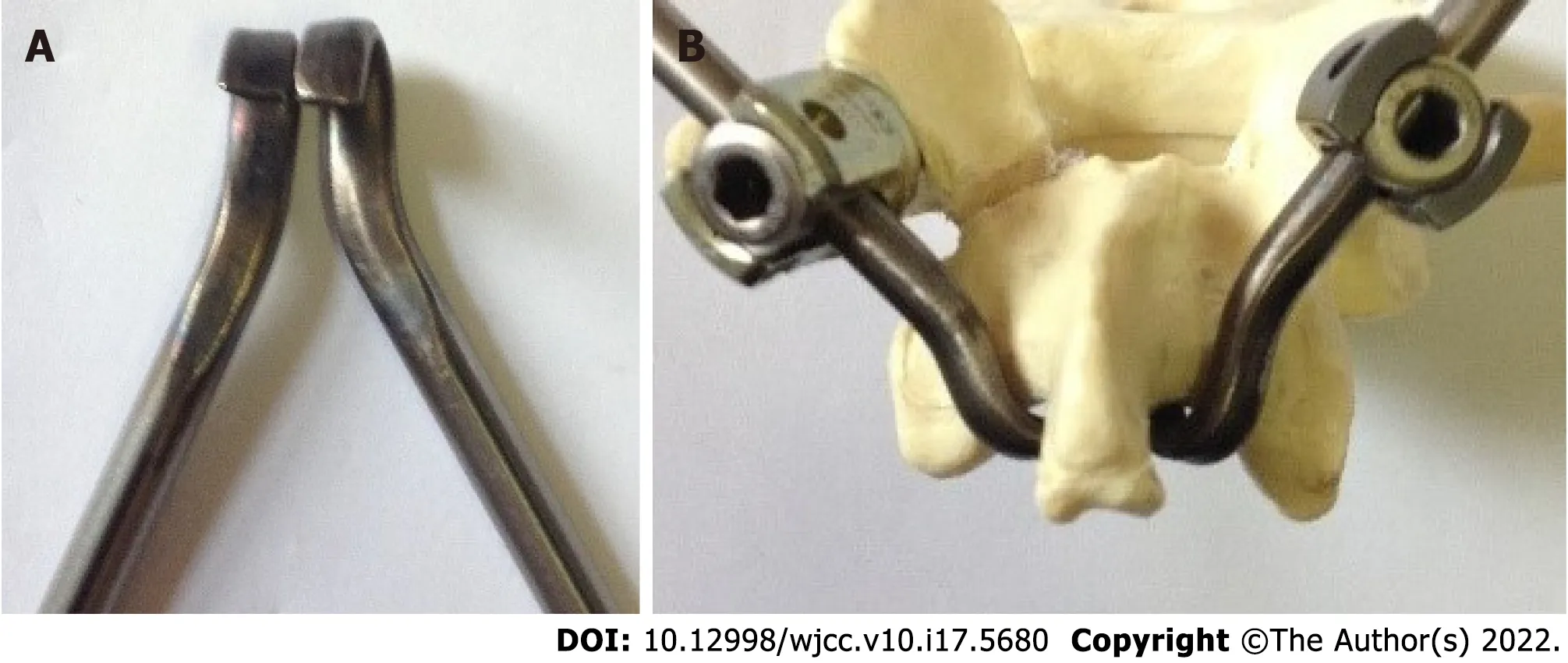
To solve these problems,we designed a new anatomical hook-rod instrument(Figure 5),which combined with pedicle screw to form anatomical hook-rod-pedicle screw system.The system can be installed by the intermuscular approach,which has the advantages of less trauma and convenient operation.At the same time,the system is firmly fixed,which is favorable for bone graft fusion.According to the anatomy of the lumbar spine,the spinous process is at a certain angle with the lamina,the lamina is inclined backward and upward,and the lower edge of lamina and the tail of pedicle screw are at a certain angle with the sagittal plane.According to the above anatomical features,the hook and the rod are inclined in these three directions.The hook is completely matched with the lamina,which is conducive to the installation of the hook at the lower edge of the lamina,and the rod is easy to connect with the universal pedicle screw.Of course,the angles of L4 and L5 are different.We have designed a series of hook-rods with different angles,which are convenient for operation.Of course,in terms of our new implant design,the fundamental principle of this system is only slightly novel compared with the traditional segmental pedicle screw rod and hook.However,according to our literature review,the design of this implant is unique so far.
However, enough cattle were left to make the young man rich, and he and his wife lived happily together, except that every now and then the girl vanished from his sight, and never told him where she had been
Research methods
We designed a new anatomic hook-rod-pedicle screw system for young patients with lumbar spondylolysis.The isthmus and the corresponding pedicle screw entry point were exposed through the intermuscular approach.Autogenous iliac bone graft was obtained to bridge the isthmus defect,and then the anatomic hook-rod-pedicle screw system was used to fix the isthmus in 15 young patients.
After handing me the change from the certificate, she looked at my face and said, “Honey, I can’t tell you exactly why right now, but I want you to go back into the store and buy a turkey, cranberry4 sauce, pumpkin5 pie or anything else you need for a Thanksgiving dinner.”
Research results
At 24 mo follow-up,the visual analogue scale score of low back pain decreased from 6.73 ± 0.88 to 0.73 ± 0.59,and the Oswestry disability index score decreased from 58.20 ± 8.99 to 7.87 ± 4.97.Computed tomography showed bilateral isthmic bone healing in 14 cases and unilateral isthmic bone healing in 1 case.Magnetic resonance imaging showed that the lumbar disc signal of the diseased segment and adjacent segments had no change compared with that before surgery.The pain visual analogue scale score of the donor site was 0.20 ± 0.41 at the last follow-up.According to the Modified Macnab score,the excellent and good rate was 100%.
Research conclusions
The application of this new anatomical hook-rod-pedicle screw system to treat young patients with lumbar spondylolysis has the advantages of less trauma,a simple operation and satisfactory clinical effects.
Research perspectives
The new anatomical hook-rod-pedicle screw system should be evaluated in a large sample multicenter randomized controlled study.
FOOTNOTES
Li DM and Jiang W designed the study;Peng BG wrote the manuscript text;Li DM and Peng BG performed the surgical operations;Li DM and Li YC contributed to critical revision;Peng BG and Jiang W contributed equally to this work;All authors reviewed the manuscript and approved the final version.
Autologous iliac bone graft is the“gold standard”in bone grafting[33],and pain in the iliac bone donor area is a common complication after iliac bone removal[34].There are many reasons for postoperative pain in the donor area,such as bone defect,adhesion,osteoporosis and cutaneous nerve injury in the donor area.A bone block with cortex and cancellous bone is taken from the posterior superior iliac spine and can be trimmed to a suitable size to meet the needs of bone grafting in the isthmus.To solve the problem of donor site pain,we used the allogeneic bone with tissue-engineered human bone morphogenetic proteins to fill the defect area of posterior superior iliac spine.Allogeneic bone contains bone morphogenetic proteins,which can induce new bone formation and promote bone growth.During the follow-up,bone growth was found in the defect of the posterior superior iliac spine,as shown in(Figure 3),and the pain in the bone donor area disappeared.
The pedicle screw-laminar hook system currently in use is not specifically designed for the treatment of lumbar spondylolysis.It has some disadvantages,such as incomplete matching between hook and lamina,difficulty in installation between rod and pedicle screw and large trauma.Complete exposure of the lamina is usually required,resulting in excessive paraspinal soft tissue dissection.
Five years passed, and then a real grief came upon the land. The Chinese really were fond of their emperor, and he now lay so ill that he was not expected to live. Already a new emperor had been chosen and the people who stood in the street asked the lord-in-waiting how the old emperor was; but he only said, “Pooh!” and shook his head.
The authors declare that they have no financial or other conflicts of interest in relation to this research and its publication.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors have read the CONSORT 2010 Statement,and the manuscript was prepared and revised according to the CONSORT 2010 Statement.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Duan-Ming Li 0000-0002-9753-1355;Yong-Chao Li 0000-0002-4460-9702;Wei Jiang 0000-0002-0680-2456;Bao-Gan Peng 0000-0003-1667-4125.
Gong ZM
Filipodia
Gong ZM
1 Farfan HF,Osteria V,Lamy C.The mechanical etiology of spondylolysis and spondylolisthesis.
1976;40-55[PMID: 1277685 DOI: 10.1097/00003086-197606000-00005]
2 Wiltse LL,Newman PH,Macnab I.Classification of spondylolisis and spondylolisthesis.
1976;23-29[PMID: 1277669 DOI: 10.1097/00003086-197606000-00003]
3 Chen MR,Moore TA,Cooperman DR,Lee MJ.Anatomic variability of 120 L5 spondylolytic defects.
2013;3: 243-248[PMID: 24436876 DOI: 10.1055/s-0033-1356765]
4 Hensinger RN.Spondylolysis and spondylolisthesis in children and adolescents.
1989;71: 1098-1107[PMID: 2668295 DOI: 10.2106/00004623-198971070-00020]
5 Nachemson A.Repair of the spondylolisthetic defect and intertransverse fusion for young patients.
1976;101-105[PMID: 776482 DOI: 10.1097/00003086-197606000-00013]
6 Blanda J,Bethem D,Moats W,Lew M.Defects of pars interarticularis in athletes: a protocol for nonoperative treatment.
1993;6: 406-411[PMID: 8274809 DOI: 10.1097/00002517-199306050-00007]
7 Steiner ME,Micheli LJ.Treatment of symptomatic spondylolysis and spondylolisthesis with the modified Boston brace.
1985;10: 937-943[PMID: 3914087 DOI: 10.1097/00007632-198512000-00013]
8 Lee CK.Accelerated degeneration of the segment adjacent to a lumbar fusion.
1988;13: 375-377[PMID: 3388124 DOI: 10.1097/00007632-198803000-00029]
9 Yang SW,Langrana NA,Lee CK.Biomechanics of lumbosacral spinal fusion in combined compression-torsion loads.
1986;11: 937-941[PMID: 3824071 DOI: 10.1097/00007632-198611000-00014]
10 Cyron BM,Hutton WC.The fatigue strength of the lumbar neural arch in spondylolysis.
1978;60-B: 234-238[PMID: 659472 DOI: 10.1302/0301-620X.60B2.659472]
11 Green TP,Allvey JC,Adams MA.Spondylolysis.Bending of the inferior articular processes of lumbar vertebrae during simulated spinal movements.
1994;19: 2683-2691[PMID: 7899964 DOI: 10.1097/00007632-199412000-00016]
12 Hefti F,Seelig W,Morscher E.Repair of lumbar spondylolysis with a hook-screw.
1992;16: 81-85[PMID: 1572778 DOI: 10.1007/BF00182992]
13 Pavlovcic V.Surgical treatment of spondylolysis and spondylolisthesis with a hook screw.
1994;18: 6-9[PMID: 8021074 DOI: 10.1007/BF00180169]
14 Ohmori K,Suzuki K,Ishida Y.Translamino-pedicular screw fixation with bone grafting for symptomatic isthmic lumbar spondylolysis.
1992;30: 379-384[PMID: 1620301 DOI: 10.1097/00006123-199203000-00011]
15 Gillet P,Petit M.Direct repair of spondylolysis without spondylolisthesis,using a rod-screw construct and bone grafting of the pars defect.
1999;24: 1252-1256[PMID: 10382254 DOI: 10.1097/00007632-199906150-00014]
16 Tokuhashi Y,Matsuzaki H.Repair of defects in spondylolysis by segmental pedicular screw hook fixation.A preliminary report.
1996;21: 2041-2045[PMID: 8883209 DOI: 10.1097/00007632-199609010-00023]
17 Roca J,Iborra M,Cavanilles-Walker JM,Albertí G.Direct repair of spondylolysis using a new pedicle screw hook fixation: clinical and CT-assessed study: an analysis of 19 patients.
2005;18 Suppl: S82-S89[PMID: 15699811 DOI: 10.1097/01.bsd.0000123425.12852.3c]
18 Debusscher F,Troussel S.Direct repair of defects in lumbar spondylolysis with a new pedicle screw hook fixation: clinical,functional and Ct-assessed study.
2007;16: 1650-1658[PMID: 17520298 DOI: 10.1007/s00586-007-0392-0]
19 He L,Ni J,Wu B,Yue J,Cao G,Guo Y,Yang L.Coblation annuloplasty in cervical discogenic pain without radiculopathy.
2020;15: 305-312[PMID: 32489491 DOI: 10.5114/wiitm.2019.89394]
20 Rajasekaran S,Kamath V,Avadhani A.Bucks fusion.
2010;19: 343-344[PMID: 20130927 DOI: 10.1007/s00586-010-1308-y]
21 Smith JA,Hu SS.Management of spondylolysis and spondylolisthesis in the pediatric and adolescent population.
1999;30: 487-499,ix[PMID: 10393770 DOI: 10.1016/S0030-5898(05)70101-2]
22 Kimura M.[My method of filing the lesion with spongy bone in spondylolysis and spondylolistesis].
1968;19: 285-296[PMID: 5693611]
23 Askar Z,Wardlaw D,Koti M.Scott wiring for direct repair of lumbar spondylolysis.
2003;28: 354-357[PMID: 12590209 DOI: 10.1097/01.BRS.0000048496.55167.22]
24 Hambly MF,Wiltse LL.A modification of the Scott wiring technique.
1994;19: 354-356[PMID: 8171371 DOI: 10.1097/00007632-199402000-00018]
25 Johnson GV,Thompson AG.The Scott wiring technique for direct repair of lumbar spondylolysis.
1992;74: 426-430[PMID: 1587895 DOI: 10.1302/0301-620X.74B3.1587895]
26 Buck JE.Direct repair of the defect in spondylolisthesis.Preliminary report.
1970;52: 432-437[PMID: 4916960 DOI: 10.1302/0301-620X.52B3.432]
27 Morscher E,Gerber B,Fasel J.Surgical treatment of spondylolisthesis by bone grafting and direct stabilization of spondylolysis by means of a hook screw.
1984;103: 175-178[PMID: 6497607 DOI: 10.1007/BF00435550]
28 Louis R.[Pars interarticularis reconstruction of spondylolysis using plates and screws with grafting without arthrodesis.Apropos of 78 cases].
1988;74: 549-557[PMID: 3070652]
29 Zhang S,Ye C,Lai Q,Yu X,Liu X,Nie T,Zhan H,Dai M,Zhang B.Double-level lumbar spondylolysis and spondylolisthesis: A retrospective study.
2018;13: 55[PMID: 29548343 DOI: 10.1186/s13018-018-0723-3]
30 Vialle R,Wicart P,Drain O,Dubousset J,Court C.The Wiltse paraspinal approach to the lumbar spine revisited: an anatomic study.
2006;445: 175-180[PMID: 16456311 DOI: 10.1097/01.blo.0000203466.20314.2a]
31 Suk KS,Lee HM,Kim NH,Ha JW.Unilateral versus bilateral pedicle screw fixation in lumbar spinal fusion.
2000;25: 1843-1847[PMID: 10888955 DOI: 10.1097/00007632-200007150-00017]
32 Whitecloud TS 3rd,Roesch WW,Ricciardi JE.Transforaminal interbody fusion versus anterior-posterior interbody fusion of the lumbar spine: a financial analysis.
2001;14: 100-103[PMID: 11285420 DOI: 10.1097/00002517-200104000-00002]
33 Dhawan A,Kuklo TR,Polly DW Jr.Analysis of iliac crest bone grafting process measures.
2006;35: 322-326[PMID: 16927657]
34 Delawi D,Dhert WJ,Castelein RM,Verbout AJ,Oner FC.The incidence of donor site pain after bone graft harvesting from the posterior iliac crest may be overestimated: a study on spine fracture patients.
2007;32: 1865-1868[PMID: 17762294 DOI: 10.1097/BRS.0b013e318107674e]
 World Journal of Clinical Cases2022年17期
World Journal of Clinical Cases2022年17期
- World Journal of Clinical Cases的其它文章
- Repetitive transcranial magnetic stimulation for post-traumatic stress disorder:Lights and shadows
- Response to dacomitinib in advanced non-small-cell lung cancer harboring the rare delE709_T710insD mutation:A case report
- Loss of human epidermal receptor-2 in human epidermal receptor-2+breast cancer after neoadjuvant treatment:A case report
- Tumor-like disorder of the brachial plexus region in a patient with hemophilia:A case report
- High-frame-rate contrast-enhanced ultrasound findings of liver metastasis of duodenal gastrointestinal stromal tumor:A case report and literature review
- Gitelman syndrome:A case report