
Higher volume growth rate is associated with development of worrisome features in patients with branch duct-intraductal papillary mucinous neoplasms
2022-06-22 11:27:10TommasoInnocentiGinevraDantiEricaNicolaLynchGabrieleDragoniMatteoGottinFilippoFedeliDanielePalatresiMariaRosaBiaginiStefanoMilaniVittorioMieleAndreaGalli
World Journal of Clinical Cases 2022年17期
lNTRODUCTlON
Pancreatic intraductal papillary mucinous neoplasms(IPMN),in their branch-duct form(BD-IPMN)are the most frequent cystic tumours of the exocrine pancreas and harbour a low risk of malignant transformation[1,2].For this reason,it is essential to stratify the risk of malignancy in order to plan the most appropriate follow-up for each patient.
The current guidelines suggest an individual risk-based screening with computed tomography(CT)scan,magnetic resonance imaging(MRI)or endoscopic ultrasound(EUS)[3-5].Cyst diameter growth rate is one of the parameters that is associated with the development of malignant features in patients with BD-IPMN[6,7].However,only the International Guidelines by Tanaka
[4]consider the cyst diameter growth rate as a worrisome feature.Recently,a nomogram based on cyst size,pancreatic duct size,presence of mural nodule,serum carbohydrate antigen(CA)19.9 and carcinoembryonic antigen(CEA)was constructed to predict malignancy in BD-IPMNs[8].However,none of the current guidelines take into account the volume of the cysts and its evolution over time,although it has recently been shown that this is a highly reproducible parameter with low inter-observer variability[9].To date,there are no studies investigating the correlation between cyst volume growth rate and the risk of malignant degeneration in patients with BD-IPMN.
In light of the lack of agreement between current guidelines,we believe it would be useful to implement the available evidence regarding the risk factors for malignancy of pancreatic BD-IPMN.Moreover,assessing cyst volume growth rate may enable the identification of patients who would benefit from a close follow-up,distinguishing them from those for whom it would be more useful to delay check-ups over time or even interrupt them for cost-effective reasons.
In all the waggon-loads there was not one piece of linen the tenth part of which would go through the ring, and the two elder brothers, who had at first sneered20 at their youngest brother for returning with no baggage, began to feel rather small
In this study,we assess the growth rate(both diameter and volume)of low-risk BD-IPMNs and evaluate its correlation with the development of malignant characteristics.Moreover,we aim to evaluate the possible superiority of measuring cyst volume instead of cyst diameters in predicting poor outcomes.
MATERlALS AND METHODS
Study design and patient enrolment
We designed a single-centre,retrospective study at our tertiary referral centre.In accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments,we evaluated data of 148 patients who were referred to our pancreatic disease outpatient clinic(Gastroenterology Unit,Careggi University Hospital,Florence,Italy)for regular IPMN follow-up.We searched in the digital clinical records using a free text entry(“IPMN”or“intraductal papillary mucinous neoplasms”or“pancreatic cyst”and“branch-duct”or“BD”)into a 10-years-period(between July 2011 and July 2021).The study was approved by the local Ethical Committee of Careggi University Hospital on July 13th 2021(protocol number: 20256_oss).
We included all adult patients with a known BD-IPMN who had at least two contrast-enhanced MRI studies or CT scans at our centre and a 12-mo minimum follow-up time.For patients who had multifocal BD-IPMN,the largest cyst was considered.Exclusion criteria were paediatric age(< 18 years),prior history of pancreatic cancer or surgery,history of acute or chronic pancreatitis,patients with worrisome features or high-risk stigmata(mentioned later)at first imaging study and patients who had their imaging studies in other clinical centres or for whom radiological study images were unavailable.
When they grew older, things became worse and worse, and at last one day as they were walking through a wood the elder youth seized hold of the other, tied him to a tree, and went on his way hoping that the boy might starve to death
IPMN were defined as a grape-like cluster of small cysts originating from a branch of the pancreatic duct,a multilocular cyst with finger-like projections or a single,lobulated cyst communicating with the main pancreatic duct(MPD)[6,10].Mucinous fluid at fine-needle aspiration and cyst fluid cytology consistent with IPMN were additional criteria.
This study has some limitations.First,the retrospective design could not allow us to set predetermined timepoints of imaging follow-up.We solved this problem by assessing growth rate rather than the total growth.Moreover,we could not assess the presence of atypia or dysplasia as histology was not available for our patients unless they underwent surgery.Third,we could not carry out a proper statistical analysis involving the characteristics of the cyst fluid as FNA was not routinely performed in our patients.However,our study was meant to search for characteristics that predict the development of worrisome features so clinical,radiological and biochemical parameters were sufficient for our purposes.Finally,since BD-IPMNs grow very slowly[29,30],a possible criticism could be addressed to the length of our cohort follow-up median time(40.5 mo
55 mo in the study by Kolb
[7]).It must be said that small increases in diameter can result in bigger volume variations so a shorter follow-up is justified.Indeed,the first-year volume growth was superior to diameter growth in predicting the development of worrisome features in our cohort.Anyway,a prospective extension of our study is ongoing to confirm our results.
For each patient we collected demographic and clinical data including sex,age at start of follow-up,smoking habits,familial history,diabetes history and follow-up duration(in months).When possible,we collected biochemical data including serum CA19.9 and CEA.Serum CA19.9 was considered high if > 37 IU/L,as reported in a recent update by Ciprani
[11].When available,we also collected data regarding EUS examination including cyst dimension(two largest diameters)and(if FNA was performed)cyst fluid CEA,amylases and cytology characteristics.
The messenger finding all still, went into the kitchen to light a candle, and, taking the glistening14 fiery15 eyes of the cat for live coals, he held a lucifer-match19 to them to light it. But the cat did not understand the joke, and flew in his face, spitting and scratching. He was dreadfully frightened, and ran to the back-door, but the dog, who lay there sprang up and bit his leg; and as he ran across the yard by the straw-heap, the donkey gave him a smart kick with its hind12 foot. The cock, too, who had been awakened16 by the noise, and had become lively, cried down from the beam, Cock-a-doodle-doo!
Radiological protocol
All CT investigations were carried out on a 128-slice CT scanner(Brilliance iCT,Philips Medical Systems,Netherlands).Patients were scanned in the supine position with cranio-caudal breath-hold scans.All patients underwent non-contrast and contrast-enhanced CT scanning with a slice thickness of 2-3 mm.Iodinated contrast medium(iopromide 370 mg I/mL - Ultravist
,Bayer Schering,Berlin)was injected into the antecubital vein at a flow rate of 3-4 mL/s using an automatic injector,immediately followed by a saline flush.The dose of the contrast medium was administered according to the patient’s body weight[mL/kg body weight: 80-100 mL(< 80 kg)or 100-120 mL(> 80 kg)].Contrast-enhanced CT images were acquired during the arterial(30-35 s),portal venous(80-90 s)and late phase(> 180 s).
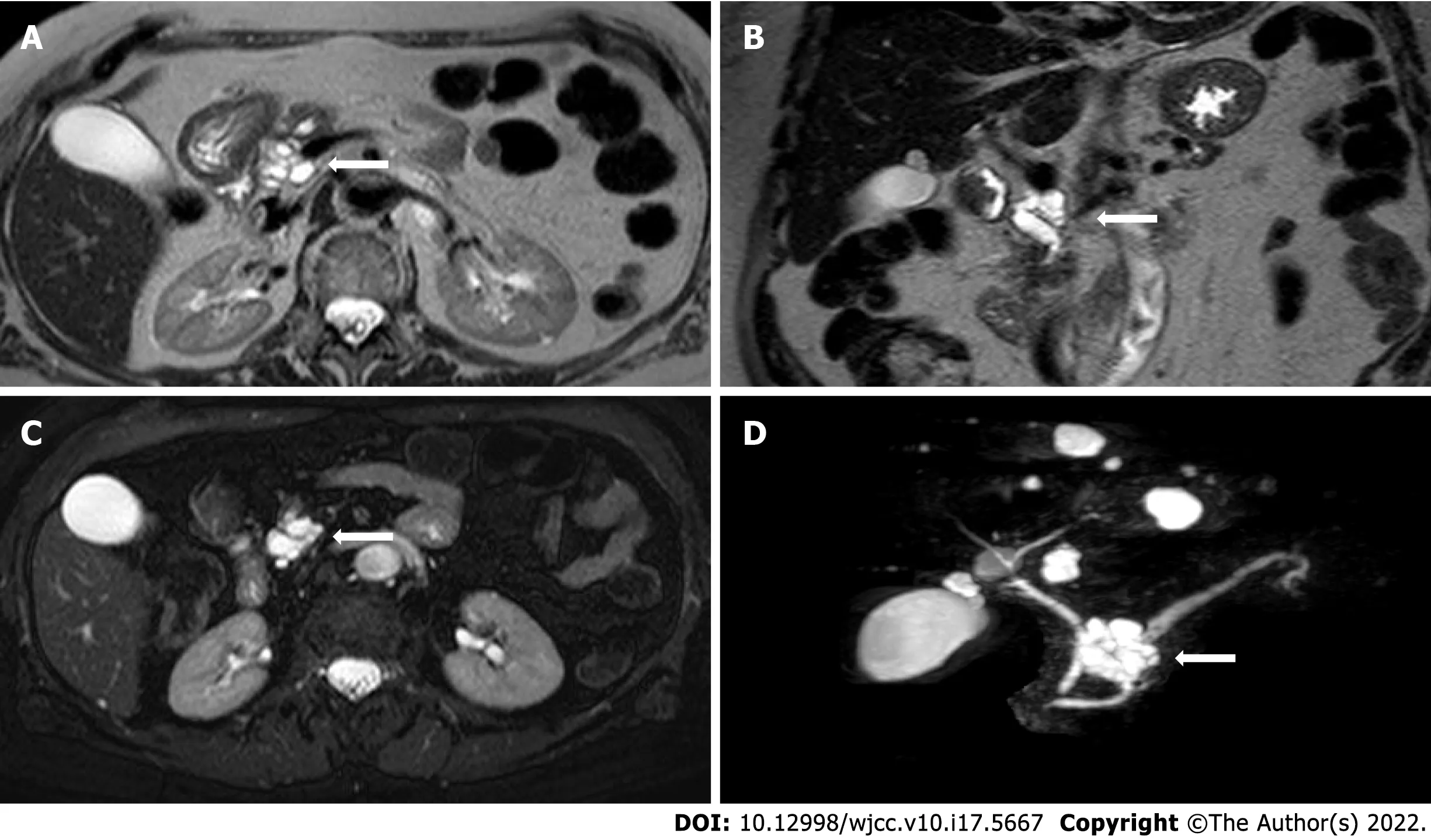
All MRI examinations were carried out on a 1.5 Tesla MRI scanner(MAGNETOM Aera,Siemens,Germany).MRI protocol for IPMN included: T2-weighted Turbo Spin Echo(TSE)or Single Shot TSE sequence acquired in axial and coronal planes;T1-weighted gradient echo(GRE)in-phase and out-ofphase sequence acquired in the axial plane;diffusion weighted imaging(DWI)(b value = 0;100;500;800)acquired in the axial plane and ADC map;cholangiographic sequences,that is T2-weighted Single Shot TSE 2D(radial)fat-sat sequences and T2-weighted volume(3D)TSE fat-sat sequences(with maximum intensity projection reconstructions).The dynamic study was obtained during the intravenous administration of gadolinium chelates contrast agents(gadoteridol 279.3 mg/mL - Prohance
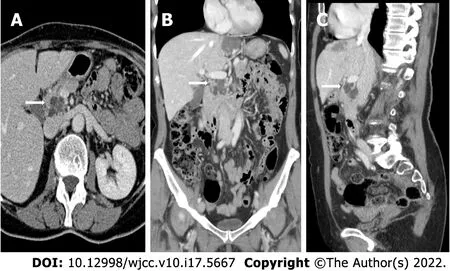
,Bracco Diagnostics Inc.,Germany;0.2 mL/kg of body weight)at a rate of 2-3 mL/s followed by saline injection with a triphasic technique: pancreatic(35-45 s),portal venous(80-90 s),and late phase(> 180 s).The dynamic study was performed with T1-weighted volume GRE sequences(3D),with selective fat saturation acquired in the axial plane.The slice thickness necessarily included the entire biliary tree and pancreatic ductal system.Figure 2 and Figure 3 report examples of our patients’ CT and MRI images.
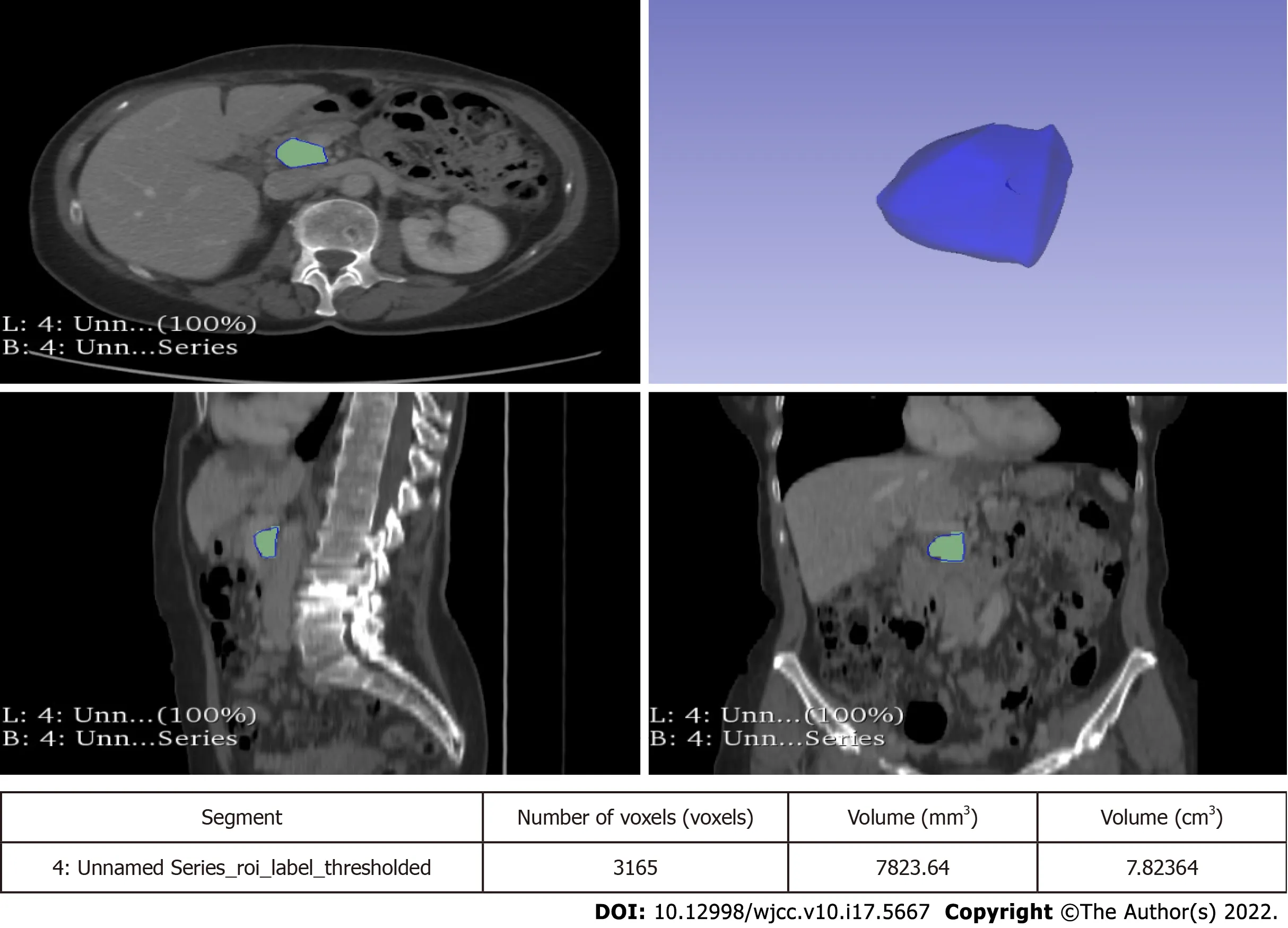
Lesions were measured on both CT and MRI images along the three major diameters(anteroposterior,latero-lateral,cranio-caudal).Volume measurement was obtained by manual segmentation with 3D Slicer software version 4.10.2(available at https://slicer.org).Manual segmentation is a widely validated and reliable method for volume measurement in both abdominal radiology and in other fields of research[12-15].The volume of the entire cyst was determined by manually drawing a region of interest along the edge of the neoplasm on each consecutive slice covering the whole lesion.Therefore,a three-dimensional(3D)volume of interest was finally obtained with the calculated value expressed in cm
.More particularly,the tumour contours were individually outlined slice-by-slice by two radiologists(at least 5 years of experience)and then reviewed by a senior radiologist(more than 10 years of experience).Any disagreement between the readers was discussed until a final consensus was generated.An example of segmentation is reported in Figure 4.
Statistical analysis
All statistical analyses were performed using SPSS Statistics version 26.0(IBM,Armonk,NY,United States).Continuous variables were expressed as medians and interquartile ranges(IQR)while categorical variables were presented as percentages.Descriptive statistics was used to compare the characteristics of patients who developed worrisome features or high-risk stigmata with that of patients who did not: continuous variables were compared using the Mann-Whitney
-test while categorical variables were compared with a Yate’s
test or a Fisher’s exact test(depending on the sample size).A two-sided
value < 0.05 was considered as significant.
“I know nothing about it,” said the emperor. “Music! music!” he cried; “the large Chinese drum! that I may not hear what they say.” But they still went on, and Death nodded like a Chinaman to all they said. “Music! music!” shouted the emperor. “You little precious golden bird, sing, pray sing! I have given you gold and costly presents; I have even hung my golden slipper round your neck. Sing! sing!” But the bird remained silent. There was no one to wind it up, and therefore it could not sing a note.
Outcomes
The primary outcomes of our study were to assess the volume growth rate of BD-IPMNs without worrisome features or high-risk stigmata at baseline and to evaluate if a higher volume growth rate correlates with the development of worrisome features or high-risk stigmata.The secondary outcomes were the following:(1)To evaluate the impact of measuring volume dimension
flat dimension(axial,coronal and longitudinal diameters);(2)To evaluate the impact of measuring volume growth rate
diameter growth rate;and(3)To test the ability of first-year volume growth rate to predict the development of worrisome features or high-risk stigmata.
One autumn evening the merchant s wife called the three girls to her and gave them each a task. One of her daughters she bade make a piece of lace, the other to knit a pair of hose, and to Vasilissa she gave a basket of flax to be spun16. She bade each finish a certain amount. Then she put out all the fires in the house, leaving only a single candle lighted in the room where the three girls worked, and she herself went to sleep.
RESULTS
Study population
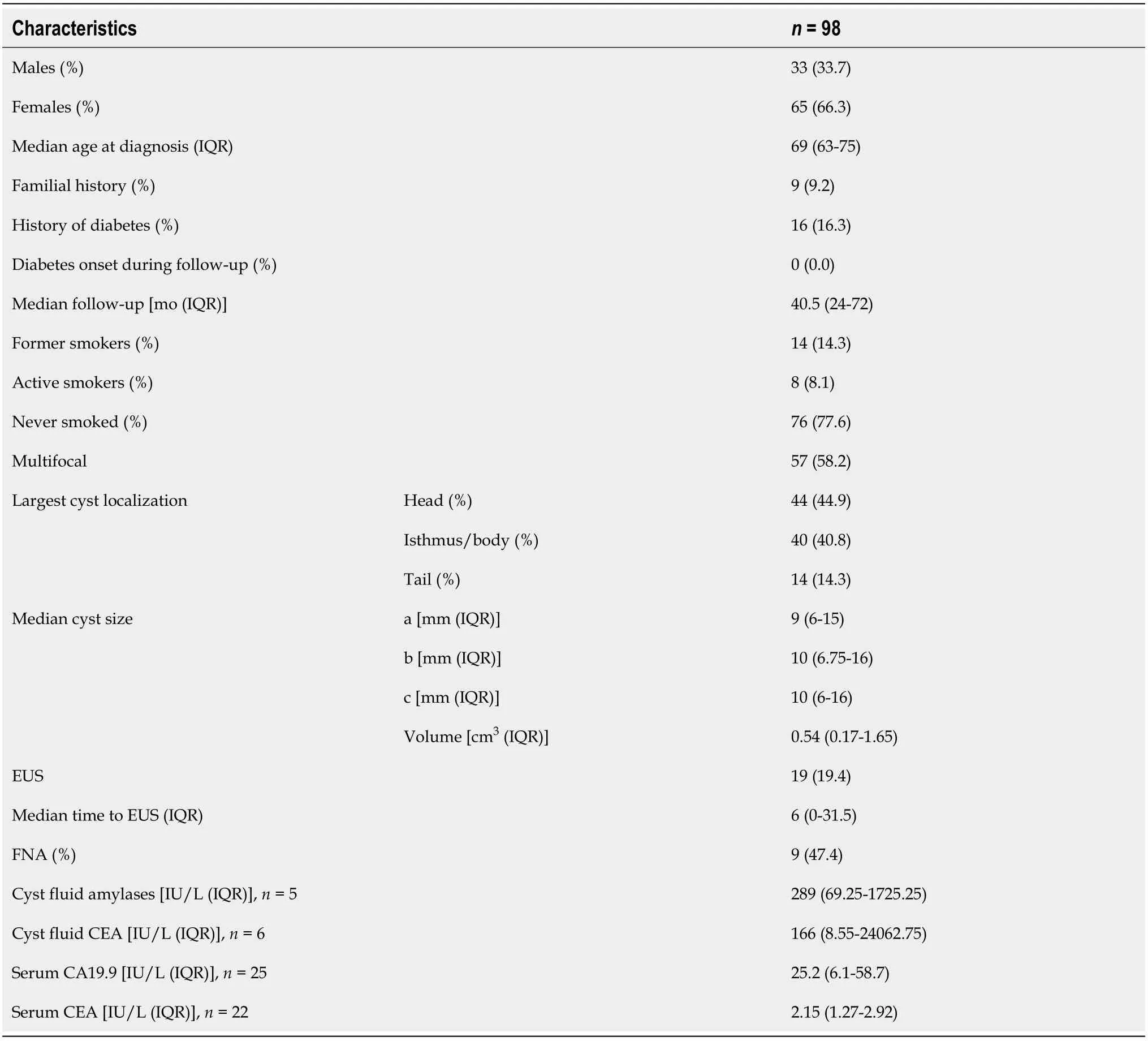
Overall,148 patients were identified.Five patients had worrisome features or high-risk stigmata at baseline and were excluded from the study.An additional 45 patients were excluded as they had unsatisfactory or incomplete follow-up information.Therefore,a total of 98 patients were included in our study.Baseline and demographic characteristics of the patients and cysts are reported in Table 1.
For some months the king’s grief was great; then gradually he began to forget a little, and, besides, his counsellors were always urging him to seek another wife. At first he refused to listen to them, but by-and-by he allowed himself to be persuaded to think of it, only stipulating7 that the bride should be more beautiful and attractive than the late queen, according to the promise he had made her.
Cyst dimension and growth rate
Baseline median cyst sizes were 9 mm(IQR 6-15)× 10 mm(IQR 6.75-16)× 10 mm(IQR 6-16).Measurements are intended to be sagittal(antero-posterior)× transversal(latero-lateral)× coronal(cranio-caudal).Baseline cyst volume was 0.54 cm
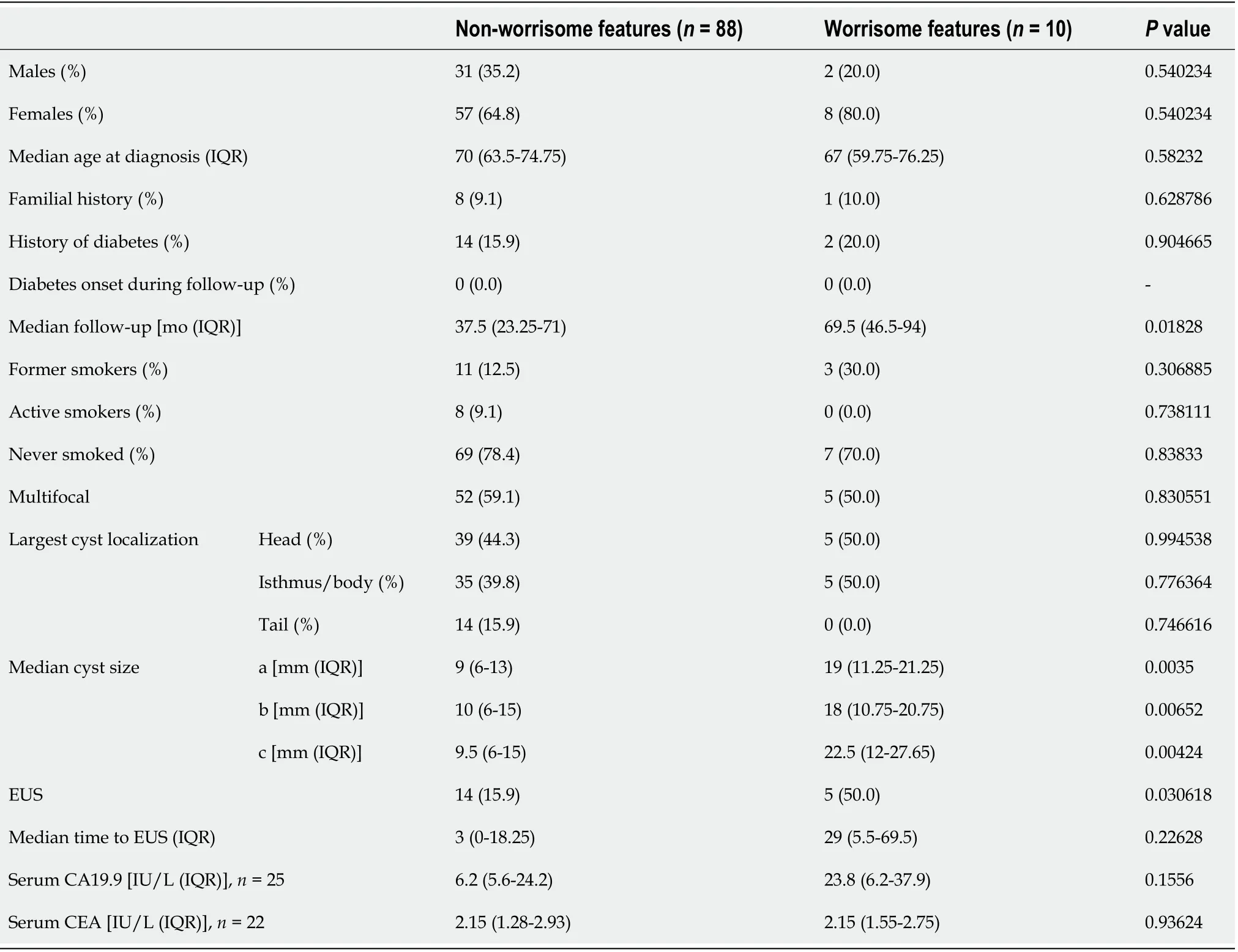
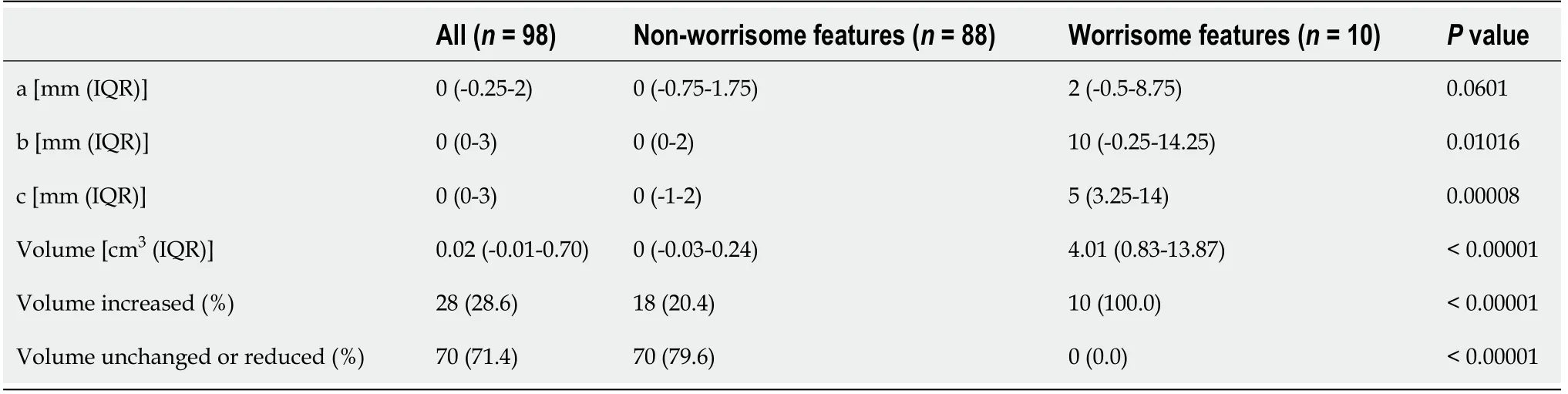
(IQR 0.17-1.65).Cysts at baseline were significantly larger in patients who developed worrisome features,as reported in Table 4.Cyst sizes and growth after follow-up are resumed in Tables 5-7.Particularly,at the end of the follow-up,patients who developed worrisome features had a median cyst volume of 10.17 cm
(IQR 2.72-19.36),with a median growth of 4.01 cm
(IQR 0.83-13.87).Both volume and cyst volume growth were significantly higher in patients who developed worrisome features(
= 0.0005 and
< 0.00001,respectively).Indeed,in patients who developed worrisome features,cyst volume grew faster than in patients who did not(1.12 cm
/year,IQR 0.28-2.65
0 cm
/year,IQR -0.02-0.17,
= 0.0001).Diameter size also grew more in patients who developed worrisome features but this growth was not always significant across all three measurement planes.
First-year prediction of worrisome features
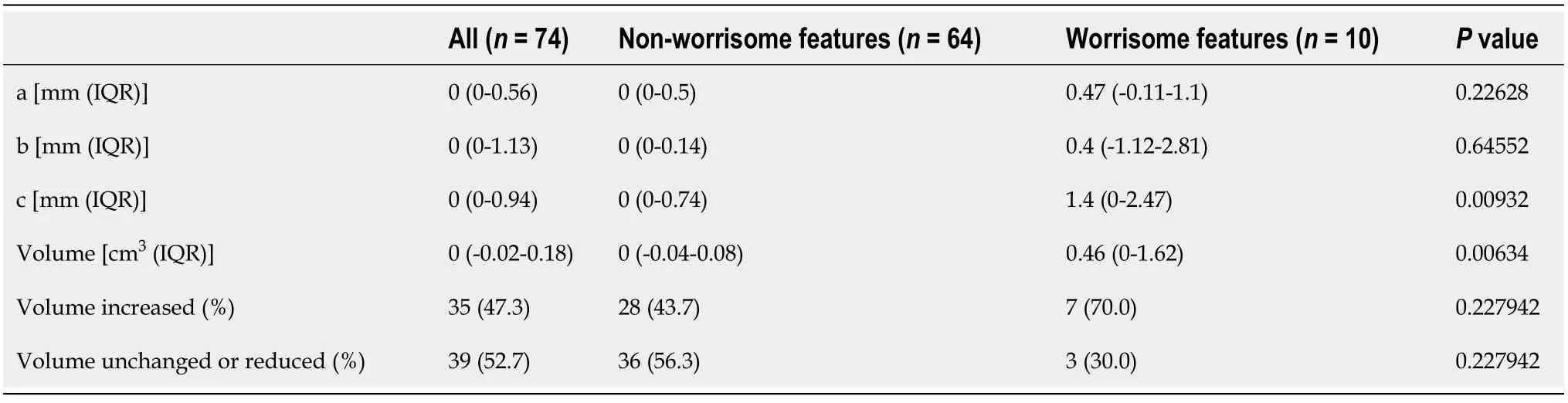
Seventy-four patients had at least 3 follow-up timepoints,of which at least two were 12 mo apart and another one later in time.In this subgroup of patients,followed for a median time of 56.5 mo(IQR 30-80.25),10 developed worrisome features.The first-year volume growth rate was higher in patients who developed worrisome features(
= 0.00634).The first-year diameter growth rate was also higher in patients with worrisome features at the end of follow-up but differences with patients who did not end up with worrisome features were not always significant.Data regarding this group of patients are reported in Table 8.




DlSCUSSlON
Pancreatic cystic neoplasms are often detected incidentally in patients who undergo abdomen CT scans or MRI for various indications[16-18].IPMNs are the most frequently diagnosed pancreatic cystic neoplasms[1]and they come in several variants: main duct IPMN or type 1(MD-IPMN),branch duct IPMN or type 2(BD-IPMN),and mixed type[19].IPMNs have a malignancy progression cumulative risk of 7%-24% in 10 years and percentages vary on an individual risk basis[2].In particular,MD-IPMN may reach a malignancy risk of 60%,while in BD-IPMN the risk remains lower than 25% in both surgical and non-surgical series[20-22].
After a 40.5-mo median follow-up(IQR 24-72),10 patients(10.2%)developed worrisome features: 6 patients had cysts larger diameter > 3 cm;3 patients had increased serum CA19.9(> 37 IU/L);1 patient had MPD ≥ 5 mm.No patients developed high-risk stigmata.Baseline cyst dimensions,both diameter and volume,were the only patient baseline characteristics which were significantly associated with the development of worrisome features(Table 2).Two of the patients who developed worrisome features underwent surgical resection.They both had a pancreaticoduodenectomy and their main characteristics are resumed in Table 3.
Current guidelines agree on surgically treating MD-IPMN and MT-IPMN and monitoring most BDIPMN(CT scan,MRI,EUS)[3-5].BD-IPMN follow-up may vary on the basis of some radiological characteristics of the cysts and on clinical and biochemical parameters.In particular,International Guidelines outlined some“high-risk stigmata
and“worrisome features
[4].The former guide the physician to a surgical approach,while the latter require a tighter follow-up.
But the King came towards her and gave her his hand, and danced with her, thinking to himself, My eyes have never beheld10 anyone so fair! When the dance was ended, she curtseyed to him, and when the King looked round she had disappeared, no one knew whither
As already mentioned,the baseline characteristic which is considered most important by the scientific community is the dimension of the cyst of larger diameter and only the International Guidelines by Tanaka
[4]include the cyst diameter growth rate as a worrisome feature.What is more,it is not always easy to identify which is the larger diameter especially when comparing different methods such as CT scan,MRI and EUS.In this study,we tried to find a new parameter that is easy to use and thatbrings more information about the evolutionary potential of BD-IPMNs: we identified it in the volume of the cysts.Cyst volume is a parameter with high reproducibility and low inter-observer variability[9]and in our opinion may allow the diagnostician to overcome some issues related to the flat measurement of the cyst.
In this study,we assess the diameter and volume growth rate of BD-IPMNs and evaluate its correlation with the development of worrisome features.We reviewed both CT and MRI images: many previous studies confirmed that diagnostic performance of contrast-enhanced CT and MRI is comparable without significant differences[23-25].We retrospectively analysed the evolution of BDIPMNs of 98 patients,who were referred to our tertiary referral centre for pancreatic diseases.Worrisome features appeared in 10.8% of patients,while no-one had high-risk stigmata,over a median 40.5-mo follow-up time.These data are in line with the current literature[26,27].
In our cohort,patients who developed worrisome features had larger cysts at baseline.In this group,cysts were significantly larger if we considered both diameters(for all diameters,
= 0.0035,
= 0.00652,
= 0.00424,respectively)and volume(
= 0.00222).Patients who developed worrisome features had a median baseline cyst volume of 5.8 cm
and a final cyst volume of 10.17 cm
.These findings are in line with a previous study in which CT and MRI techniques were used to measure IPMNs volume: a volume > 10 cm
was associated with malignancy[28].However,this study did not assess volume changes over time but only a spot volume measurement.
In summary,as opposed to diameter growth,the cyst volume growth(total,annual and first-year growth)was consistently greater in patients who developed worrisome features.The diameter growth rate was also significantly correlated in some cases,but not of all diameters at once,and not always of the largest diameter.Therefore,the flat growth rate could be misinterpreted if it is not the largest diameter that grows,or when the cysts have an irregular shape which is hard to measure in a reproducible way.The volume measurement could overcome these issues.In fact,the volume has a unique size instead of diameters that are virtually endless.For these reasons,volume measurement could be more comparable than diameters.Recently,Pandey
[9]demonstrated that measurement of volume is feasible and reproducible and can be considered as an alternative to diameter measurement.In their work,they used both a manual and a semiautomatic technique of measurement while we used a manual technique.
The peculiarity of our work was the measurement of cyst volume over time.In our cohort,total growth and growth rate were significantly higher in patients who developed worrisome features if compared to patients who did not(
< 0.00001 and
= 0.0001,respectively).To our knowledge,this isthe first study in which baseline volume and particularly volume total growth and growth rate are correlated with development of worrisome features in patients with BD-IPMN.
Indeed! said the Vizier; so that when I go home my wife may scratch my eyes out! Besides, I am an old man, and your Highness is still young and unmarried, and a far more suitable match for a young and lovely Princess
Beyond the raw data of annual growth,we set out to identify a parameter that allows the early prediction of development of worrisome features in the medium-long term: we found out that patients who developed worrisome features had a higher first-year cyst volume growth if compared with patients who did not(0.46 cm
/year
0.0 cm
/year,
= 0.00634).These data are notable if we consider that the diameter growth rate was not significantly different between the two groups,except for the cranio-caudal one(
= 0.22628,
= 0.64552,
= 0.00932).To our knowledge,this is a unique result asthis is the first study to prove that cyst volume growth in the first year predicts development of worrisome features in patients with BD-IPMN without worrisome features at baseline.This could be an important tool to add to the current knowledge to improve the management of low-risk IPMNs.
In the group of patients who developed worrisome features,diameter growth rate was significantly higher if we considered latero-lateral and cranio-caudal diameters(1.55 mm/year
0.0 mm/year,
= 0.0394,and 1.96 mm/year
0.0 mm/year,
= 0.00152,respectively),but not antero-posterior diameters(0.63 mm/year
0.0 mm/year,
= 0.14156).In a recent study by Kolb
[7],188 patients were followed-up for a median 55-mo period and 12 out of all patients developed worrisome features.They measured cysts diameter on both the axial and coronal plans on X and Y axis and cyst growth rate was higher in patients who developed worrisome features(axial X 2.84 mm/year
0.23 mm/year,
< 0.001;axial Y 1.02 mm/year
0.02 mm/year,
= 0.033;coronal X 1.21 mm/year
0.19 mm/year,
= 0.001,coronal Y 1.56 mm/year
0.00 mm/year,
< 0.001).The larger population and the longer median follow-up period may have contributed to improving statistical significance in their work.A similar result was obtained in a previous surgical cohort(4.1 mm/year
1.0 mm/year,
= 0.001)[6].
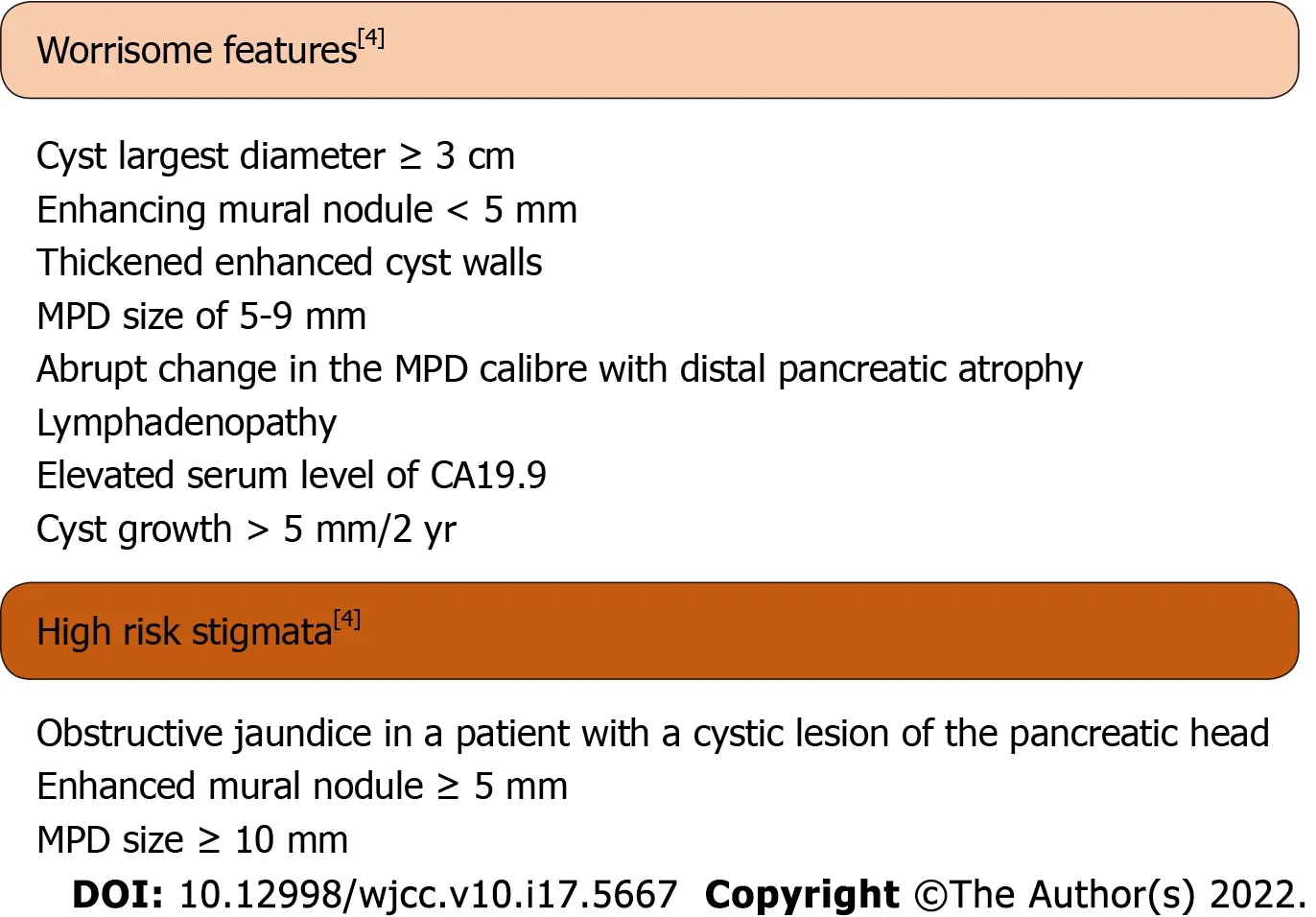
Worrisome features and high-risk stigmata were defined as in the 2017 Fukuoka guidelines(Figure 1).Worrisome features include cyst of ≥ 3 cm,enhancing mural nodule < 5 mm,thickened enhanced cyst walls,MPD size of 5-9 mm,abrupt change in the MPD calibre with distal pancreatic atrophy,lymphadenopathy,an elevated serum level of CA19.9 and a rapid rate of cyst growth > 5 mm/2 years.High-risk stigmata include obstructive jaundice in a patient with a cystic lesion of the pancreatic head,enhanced mural nodule ≥ 5 mm and MPD size ≥ 10 mm[4].
CONCLUSlON
However, the fairy did not think of that, but, carried away by her new ideas, she hastily formed a Council, and named as Prime Minister the excellent Ditto, so called because he had never been known to contradict anybody
ARTlCLE HlGHLlGHTS
Research background
Branch duct-intraductal papillary mucinous neoplasms(BD-IPMNs)are the most common pancreatic cystic tumours.Cyst diameter growth rate is one of the parameters that current guidelines take into account to predict the development of malignant features in patients with BD-IPMN.However,to date,there are no studies investigating the correlation between cyst volume growth rate and the risk of BDIPMNs malignant degeneration.
Research motivation
The optimal surveillance protocol for BD-IPMNs has not been established as there is lack of agreement on when follow-up should be intensified or interrupted mainly due to the slow growth rate of BDIPMNs.We propose a more precise tool for the measurement of BD-IPMNs which allows an early prediction of the development of worrisome features.
Research objectives
The primary objective of our research was to assess the volume growth rate of BD-IPMNs without worrisome features or high-risk stigmata at baseline and to evaluate its correlation with the development of worrisome features or high-risk stigmata during follow-up.We also aimed to evaluate the impact of measuring volume
diameter growth rate and to test the ability of first-year volume growth rate to predict the development of worrisome features or high-risk stigmata.
Research methods
We measured diameter in CT-scans and MRI on three planes,while we calculated the volume by manual segmentation: the volume of the cyst was determined by drawing a region of interest along the edge of the neoplasm on each consecutive slice covering the whole lesion;therefore,a three-dimensional volume of interest was finally obtained with the calculated value expressed in cm
.Changes in size over time and development of worrisome features or high-risk stigmata were measured.
Research results
Ninety-eight patients were evaluated across a 40.5-mo median follow-up time,of which 10 developed worrisome features,while none developed high-risk stigmata.Baseline volume was larger,and volume and first-year volume growth rate were higher in patients who developed worrisome features than in patients who did not.Baseline diameter was larger in patients who developed worrisome features.Diameter growth rate was higher as well but the difference did not always reach statistical significance.
Research conclusions
The measurement of baseline volume and of its variation over time is a reliable tool for the follow-up of BD-IPMNs.Particularly,in the first year of BD-IPMNs follow-up,volume measurement is more accurate than diameter alone for risk stratification.
At the sight of these wonders even the scolding tongue ceased, and the woman approached, and took the stones in her hand, setting greedily aside those that were the largest and most costly15
Research perspectives
We suggest that measuring cyst volume routinely could be a useful tool to monitor low-risk IPMNs.Larger cohorts of patients and a longer follow-up time are needed to corroborate these data and to understand whether our findings could influence routine clinical practice.
Our study confirms that BD-IPMN higher cyst growth rate is associated with a higher risk of developing worrisome features.Moreover,we proved that cyst volume growth rate is also related to the emergence of worrisome features and that the cyst volume increase in the first year of follow-up is an early predictor of the development of worrisome features.More specifically,our data show that in the first year of follow-up,volume measurement is more accurate than diameter alone for risk stratification.This suggests that measuring cyst volume routinely could be a useful tool to monitor low-risk IPMNs.Further studies,comprehensive of a larger pool of patients and a longer follow-up time are needed to corroborate these data and to understand whether our findings could influence routine clinical practice.
FOOTNOTES
Innocenti T designed the study and drafted the initial manuscript;Innocenti T,Danti G,Lynch EN and Gottin M participated in the acquisition,analysis and interpretation of the data;Danti G,Fedeli F and Palatresi D participated in the acquisition and segmentation of the CT and MRI images and provided important contribution to analysis and interpretation of the data;Biagini MR,Milani S,Miele V and Galli A revised the article critically for important intellectual content;Lynch EN provided English language revision as a native speaker;Galli A cooperated to set the study design,revised the statistical analysis and was the guarantor of the study;All authors approved the final version of the article.
The study was approved by the local Ethical Committee of Careggi University Hospital on July 13th 2021(protocol number: 20256_oss).
All study participants provided informed written consent about personal and medical data collection prior to study enrolment.
The Authors declare no conflict of interest and no financial interests in any products mentioned in this paper.
No additional data are available.
The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
When he was very nearly home he again thought of the cow that was with calf9, so he laid down the money, ran home, and asked his wife whether the cow had calved yet
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Italy
Tommaso Innocenti 0000-0002-2154-0490;Ginevra Danti 0000-0002-7109-8119;Erica Nicola Lynch 0000-0002-2638-2559;Gabriele Dragoni 0000-0001-5752-5113;Matteo Gottin 0000-0002-9292-7078;Filippo Fedeli 0000-0002-7918-9912;Daniele Palatresi 0000-0003-0452-7232;Maria Rosa Biagini 0000-0003-4840-6731;Stefano Milani 0000-0002-1337-9107;Vittorio Miele 0000-0002-7848-1567;Andrea Galli 0000-0001-5416-6290.
Società Italiana Di Gastroenterologia Ed Endoscopia Digestiva.
Although she was intimidated6 by the crowd at Balmoral, Diana was wise enough not to stay in the castle itself. She asked for, and was granted, an invitation to stay with her sister Jane and her young husband at their cottage on the Balmoral estate.
Gong ZM
He left that to her. She learned sign language as quickly as possible. Her husband wasn t interested. When he talked to the boys, he treated them like they were dogs, patting them on the head, barking out a word or two.
Filipodia
Gong ZM
1 Nagtegaal ID,Odze RD,Klimstra D,Paradis V,Rugge M,Schirmacher P,Washington KM,Carneiro F,Cree IA;WHO Classification of Tumours Editorial Board.The 2019 WHO classification of tumours of the digestive system.
2020;76: 182-188[PMID: 31433515 DOI: 10.1111/his.13975]
2 Choi SH,Park SH,Kim KW,Lee JY,Lee SS.Progression of Unresected Intraductal Papillary Mucinous Neoplasms of the Pancreas to Cancer: A Systematic Review and Meta-analysis.
2017;15: 1509-1520.e4[PMID: 28342950 DOI: 10.1016/j.cgh.2017.03.020]
3 Vege SS,Ziring B,Jain R,Moayyedi P;Clinical Guidelines Committee;American Gastroenterology Association.American gastroenterological association institute guideline on the diagnosis and management of asymptomatic neoplastic pancreatic cysts.
2015;148: 819-822;quize12[PMID: 25805375 DOI: 10.1053/j.gastro.2015.01.015]
4 Tanaka M,Fernández-Del Castillo C,Kamisawa T,Jang JY,Levy P,Ohtsuka T,Salvia R,Shimizu Y,Tada M,Wolfgang CL.Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas.
2017;17: 738-753[PMID: 28735806 DOI: 10.1016/j.pan.2017.07.007]
5 European Study Group on Cystic Tumours of the Pancreas.European evidence-based guidelines on pancreatic cystic neoplasms.
2018;67: 789-804[PMID: 29574408 DOI: 10.1136/gutjnl-2018-316027]
6 Kang MJ,Jang JY,Kim SJ,Lee KB,Ryu JK,Kim YT,Yoon YB,Kim SW.Cyst growth rate predicts malignancy in patients with branch duct intraductal papillary mucinous neoplasms.
2011;9: 87-93[PMID: 20851216 DOI: 10.1016/j.cgh.2010.09.008]
7 Kolb JM,Argiriadi P,Lee K,Liu X,Bagiella E,Gupta S,Lucas AL,Kim MK,Kumta NA,Nagula S,Sarpel U,DiMaio CJ.Higher Growth Rate of Branch Duct Intraductal Papillary Mucinous Neoplasms Associates With Worrisome Features.
2018;16: 1481-1487[PMID: 29535058 DOI: 10.1016/j.cgh.2018.02.050]
8 Jang JY,Park T,Lee S,Kim Y,Lee SY,Kim SW,Kim SC,Song KB,Yamamoto M,Hatori T,Hirono S,Satoi S,Fujii T,Hirano S,Hashimoto Y,Shimizu Y,Choi DW,Choi SH,Heo JS,Motoi F,Matsumoto I,Lee WJ,Kang CM,Han HS,Yoon YS,Sho M,Nagano H,Honda G,Kim SG,Yu HC,Chung JC,Nagakawa Y,Seo HI,Yamaue H.Proposed Nomogram Predicting the Individual Risk of Malignancy in the Patients With Branch Duct Type Intraductal Papillary Mucinous Neoplasms of the Pancreas.
2017;266: 1062-1068[PMID: 27607098 DOI: 10.1097/SLA.0000000000001985]
9 Pandey P,Pandey A,Varzaneh FN,Ghasabeh MA,Fouladi D,Khoshpouri P,Shao N,Zarghampour M,Hruban RH,Canto M,O'Broin-Lennon AM,Kamel IR.Are pancreatic IPMN volumes measured on MRI images more reproducible than diameters?
2018;28: 2790-2800[PMID: 29404774 DOI: 10.1007/s00330-017-5268-z]
10 Kim SY,Lee JM,Kim SH,Shin KS,Kim YJ,An SK,Han CJ,Han JK,Choi BI.Macrocystic neoplasms of the pancreas: CT differentiation of serous oligocystic adenoma from mucinous cystadenoma and intraductal papillary mucinous tumor.
2006;187: 1192-1198[PMID: 17056905 DOI: 10.2214/AJR.05.0337]
11 Ciprani D,Morales-Oyarvide V,Qadan M,Hank T,Weniger M,Harrison JM,Rodrigues C,Horick NK,Mino-Kenudson M,Ferrone CR,Warshaw AL,Lillemoe KD,Fernández-Del Castillo C.An elevated CA 19-9 is associated with invasive cancer and worse survival in IPMN.
2020;20: 729-735[PMID: 32332003 DOI: 10.1016/j.pan.2020.04.002]
12 Zhang X,Zhong L,Zhang B,Zhang L,Du H,Lu L,Zhang S,Yang W,Feng Q.The effects of volume of interest delineation on MRI-based radiomics analysis: evaluation with two disease groups.
2019;19: 89[PMID: 31864421 DOI: 10.1186/s40644-019-0276-7]
13 Granata V,Fusco R,Barretta ML,Picone C,Avallone A,Belli A,Patrone R,Ferrante M,Cozzi D,Grassi R,Izzo F,Petrillo A.Radiomics in hepatic metastasis by colorectal cancer.
2021;16: 39[PMID: 34078424 DOI: 10.1186/s13027-021-00379-y]
14 Nazari M,Shiri I,Zaidi H.Radiomics-based machine learning model to predict risk of death within 5-years in clear cell renal cell carcinoma patients.
2021;129: 104135[PMID: 33254045 DOI: 10.1016/j.compbiomed.2020.104135]
15 Sepehri S,Tankyevych O,Iantsen A,Visvikis D,Hatt M,Cheze Le Rest C.Accurate Tumor Delineation
Rough Volume of Interest Analysis for
F-FDG PET/CT Radiomics-Based Prognostic Modeling inNon-Small Cell Lung Cancer.
2021;11: 726865[PMID: 34733779 DOI: 10.3389/fonc.2021.726865]
16 Laffan TA,Horton KM,Klein AP,Berlanstein B,Siegelman SS,Kawamoto S,Johnson PT,Fishman EK,Hruban RH.Prevalence of unsuspected pancreatic cysts on MDCT.
2008;191: 802-807[PMID: 18716113 DOI: 10.2214/AJR.07.3340]
17 Lee KS,Sekhar A,Rofsky NM,Pedrosa I.Prevalence of incidental pancreatic cysts in the adult population on MR imaging.
2010;105: 2079-2084[PMID: 20354507 DOI: 10.1038/ajg.2010.122]
18 Pezzilli R,Buscarini E,Pollini T,Bonamini D,Marchegiani G,Crippa S,Belfiori G,Sperti C,Moletta L,Pozza G,De Nucci G,Manes G,Mandelli ED,Casadei R,Ricci C,Alicante S,Vattiato C,Carrara S,Di Leo M,Fabbri C,Giovanelli S,Barresi L,Tacelli M,Mirante VG,Conigliaro R,Antonini F,Macarri G,Frulloni L,De Marchi G,Sassatelli R,Cecinato P,Del Vecchio Blanco G,Galli A,Pezzullo A,Fantin A,Graffeo M,Frego M,Stillittano D,Monica F,Germanà B,Capurso G,Quartini M,Veneroni L,Cannizzaro R,Falconi M.Epidemiology,clinical features and diagnostic work-up of cystic neoplasms of the pancreas: Interim analysis of the prospective PANCY survey.
2020;52: 547-554[PMID: 32122771 DOI: 10.1016/j.dld.2020.02.003]
19 Klibansky DA,Reid-Lombardo KM,Gordon SR,Gardner TB.The clinical relevance of the increasing incidence of intraductal papillary mucinous neoplasm.
2012;10: 555-558[PMID: 22210438 DOI: 10.1016/j.cgh.2011.12.029]
20 Perri G,Marchegiani G,Frigerio I,Dervenis CG,Conlon KC,Bassi C,Salvia R.Management of Pancreatic Cystic Lesions.
2020;37: 1-9[PMID: 30636253 DOI: 10.1159/000496509]
21 Pergolini I,Sahora K,Ferrone CR,Morales-Oyarvide V,Wolpin BM,Mucci LA,Brugge WR,Mino-Kenudson M,Patino M,Sahani DV,Warshaw AL,Lillemoe KD,Fernández-Del Castillo C.Long-term Risk of Pancreatic Malignancy in Patients With Branch Duct Intraductal Papillary Mucinous Neoplasm in a Referral Center.
2017;153: 1284-1294.e1[PMID: 28739282 DOI: 10.1053/j.gastro.2017.07.019]
22 Crippa S,Capurso G,Cammà C,Fave GD,Castillo CF,Falconi M.Risk of pancreatic malignancy and mortality in branchduct IPMNs undergoing surveillance: A systematic review and meta-analysis.
2016;48: 473-479[PMID: 26965783 DOI: 10.1016/j.dld.2016.02.003]
23 Choi SY,Kim JH,Yu MH,Eun HW,Lee HK,Han JK.Diagnostic performance and imaging features for predicting the malignant potential of intraductal papillary mucinous neoplasm of the pancreas: a comparison of EUS,contrast-enhanced CT and MRI.
2017;42: 1449-1458[PMID: 28144718 DOI: 10.1007/s00261-017-1053-3]
24 Liu H,Cui Y,Shao J,Shao Z,Su F,Li Y.The diagnostic role of CT,MRI/MRCP,PET/CT,EUS and DWI in the differentiation of benign and malignant IPMn:A meta-analysis.
2021;72: 183-193[PMID: 33321460 DOI: 10.1016/j.clinimag.2020.11.018]
25 Huynh T,Ali K,Vyas S,Dezsi K,Strickland D,Basinski T,Chen DT,Jiang K,Centeno B,Malafa M,Klapman JB,Hodul PJ,Jeong D,Permuth JB.Comparison of imaging modalities for measuring the diameter of intraductal papillary mucinous neoplasms of the pancreas.
2020;20: 448-453[PMID: 32113936 DOI: 10.1016/j.pan.2020.02.013]
26 Canto MI,Almario JA,Schulick RD,Yeo CJ,Klein A,Blackford A,Shin EJ,Sanyal A,Yenokyan G,Lennon AM,Kamel IR,Fishman EK,Wolfgang C,Weiss M,Hruban RH,Goggins M.Risk of Neoplastic Progression in Individuals at High Risk for Pancreatic Cancer Undergoing Long-term Surveillance.
2018;155: 740-751.e2[PMID: 29803839 DOI: 10.1053/j.gastro.2018.05.035]
27 Ciprani D,Weniger M,Qadan M,Hank T,Horick NK,Harrison JM,Marchegiani G,Andrianello S,Pandharipande PV,Ferrone CR,Lillemoe KD,Warshaw AL,Bassi C,Salvia R,Fernández-Del Castillo C.Risk of malignancy in small pancreatic cysts decreases over time.
2020;20: 1213-1217[PMID: 32819844 DOI: 10.1016/j.pan.2020.08.003]
28 Murayama S,Kimura W,Hirai I,Takasu N,Takeshita A,Moriya T.Volumetric and morphological analysis of intraductal papillary mucinous neoplasm of the pancreas using computed tomography and magnetic resonance imaging.
2011;40: 876-882[PMID: 21747312 DOI: 10.1097/MPA.0b013e31821fdcff]
29 Crippa S,Bassi C,Salvia R,Malleo G,Marchegiani G,Rebours V,Levy P,Partelli S,Suleiman SL,Banks PA,Ahmed N,Chari ST,Fernández-Del Castillo C,Falconi M.Low progression of intraductal papillary mucinous neoplasms with worrisome features and high-risk stigmata undergoing non-operative management:A mid-term follow-up analysis.
2017;66: 495-506[PMID: 26743012 DOI: 10.1136/gutjnl-2015-310162]
30 Lee BS,Nguyen AK,Tekeste TF,Chang K,Girgis A,Adeyemo M,Hanna MS,Yao JF,Kwok KK,Giap AQ,Hunt GC,Chaya CT,Kao KT,Attam R,Ko A,Pio JR,Tovar S,Lim BS.Long-term follow-up of branch-duct intraductal papillary mucinous neoplasms with No change in first 5 Years of diagnosis.
2021;21: 144-154[PMID: 33309223 DOI: 10.1016/j.pan.2020.10.040]
 World Journal of Clinical Cases2022年17期
World Journal of Clinical Cases2022年17期
- World Journal of Clinical Cases的其它文章
- Repetitive transcranial magnetic stimulation for post-traumatic stress disorder:Lights and shadows
- Response to dacomitinib in advanced non-small-cell lung cancer harboring the rare delE709_T710insD mutation:A case report
- Loss of human epidermal receptor-2 in human epidermal receptor-2+breast cancer after neoadjuvant treatment:A case report
- Tumor-like disorder of the brachial plexus region in a patient with hemophilia:A case report
- High-frame-rate contrast-enhanced ultrasound findings of liver metastasis of duodenal gastrointestinal stromal tumor:A case report and literature review
- Gitelman syndrome:A case report