
Pancreatic head vs pancreatic body/tail cancer:Are they different?
2022-03-30 02:05:06KaiSunCharismaMylavarapuAubreyCrenshawYuqiZhangEnshuoHsuJiaqiongXuMarilynNiravathStephenJonesAdrianaOrdonezMaenAbdelrahim
lNTRODUCTlON
Pancreatic cancer is the fourth-leading cause of cancer deaths in the United States.Even though the survival rates have improved slightly over the past four decades,the outcome of pancreatic cancer is still dismal.Anatomically pancreatic cancer can be divided into pancreatic head cancer(PHC)and pancreatic body/tail cancer(PBTC).The lower part of head and uncinate process of pancreas has different embryological origins from the rest of the pancreas[1].This embryological difference leads to significant differences in cell composition,blood supply,lymphatic and venous drainage and innervations between the head and body/tail of pancreas.
Pancreatic tumor location impacts patient presentation and survival,which has been shown in large data-based analyses,even though with conflicting results.49%-77.5% pancreatic cancers are PHC[2-4],which tend to present at earlier stages than PBTC.Historically,survival of PBTC cancer is believed to be worse than PHC;and PBTC is considered as an independent poor prognostic risk factor.However,PBTC was found to have much better survival over PHC(20%
9%)when the tumor is localized[2].
Genetic analyses of pancreatic cancer have suggested that PHC and PBTC are different tumors.Advanced technology including whole genome sequencing and RNA sequencing further classified pancreatic cancer into four subtypes:Classical,squamous,ADEX and immunogenic[5].The squamous subtype is characterized by genes highly expressed in the C2-squamous-like class of tumors(
,lung and head and neck cancer)[6].PBTC is found to have more squamous subtypes[7,8].
I gazed at her big brown eyes and flawless skin. I held her hand in mine, counting each finger. I held her close and sang to her softly, “Jesus loves me.” Time stood still.
Given that TP53 mutations predict gemcitabine sensitivity,gemcitabine containing chemotherapy should be considered for PBTC as first line.
AT a rich merchant s house there was a children s party, and thechildren of rich and great people were there. The merchant was alearned man, for his father had sent him to college, and he had passedhis examination. His father had been at first only a cattle dealer,but always honest and industrious1, so that he had made money, andhis son, the merchant, had managed to increase his store. Clever as hewas, he had also a heart; but there was less said of his heart than ofhis money. All descriptions of people visited at the merchant s house,well born, as well as intellectual, and some who possessed2 neitherof these recommendations.
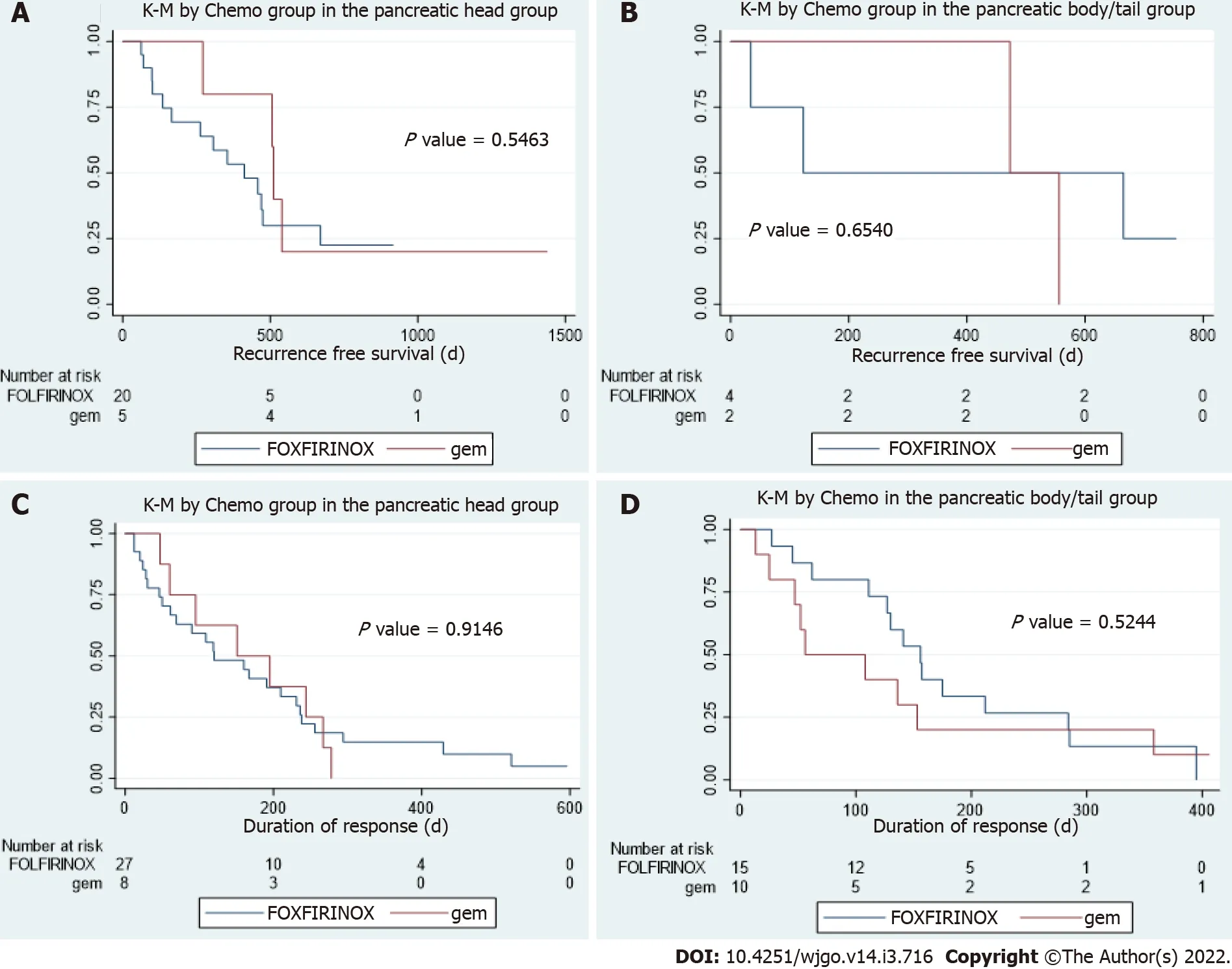
In patients who underwent resection,there were no statistical differences in disease free interval between patients with PHC or PBTC who received FOLFIRINOX based chemotherapy and those whoreceived gemcitabine-based chemotherapy(
values are 0.55 and 0.65 respectively,Figure 3A and B).In patients with metastatic disease,there were no statistical differences in duration of response to first line palliative chemo between patients with PHC or PBTC who received FOLFIRINOX-based chemotherapy and those who received gemcitabine-based chemotherapy(
values are 0.91 and 0.52 respectively,Figure 3C and D).
MATERlALS AND METHODS
The study was approved by the institutional review boards.Informed consent was waived given the retrospective nature of the study.The patient data was queried from Epic electronic medical record system of Houston Methodist Hospital.Patients who had a diagnosis of pancreatic cancer from July 2016 through June 2020 were included.Patient demographics,tumor location,pathology,staging,molecular profiles,treatment history and survival were collected retrospectively.Molecular profiles were performed through a multiplatform approach including next gene sequencing(NGS)and RNA sequencing by commercially available testing from Caris Life Sciences(Phoenix,AZ),FoundationOne(Cambridge,MA),Guardant360(Redwood City,CA),Tempus(Chicago,IL)and NeoGenomics(Fort Meyers,FL),and in house 50 gene or 70 gene panel that was developed and validated in our institution.Panels of gene mutations are available on each company’s website.Duration of response is defined as the duration of having complete response,partial response or stable disease.Overall survival is defined as the time from pancreatic cancer diagnosis to the date of death or date of last follow-up.Disease free interval is defined as the time from definitive treatment to the date of disease recurrence.Patients who had response and survival data were included in the survival and response analysis.Patients who had molecular profiling data were included in the tumor location analysis.Those who didn’t have either records were excluded from the study.
If anyone deserves a special day, it s these brave souls who ve had to carve out a place for themselves in readymade families with the care and caution of a neurosurgeon.
When his peapole doubled over, he knew something huge was on the other end. His father watched with admiration6 as the boy skillfully worked the fish alongside the dock.
RESULTS
Patients
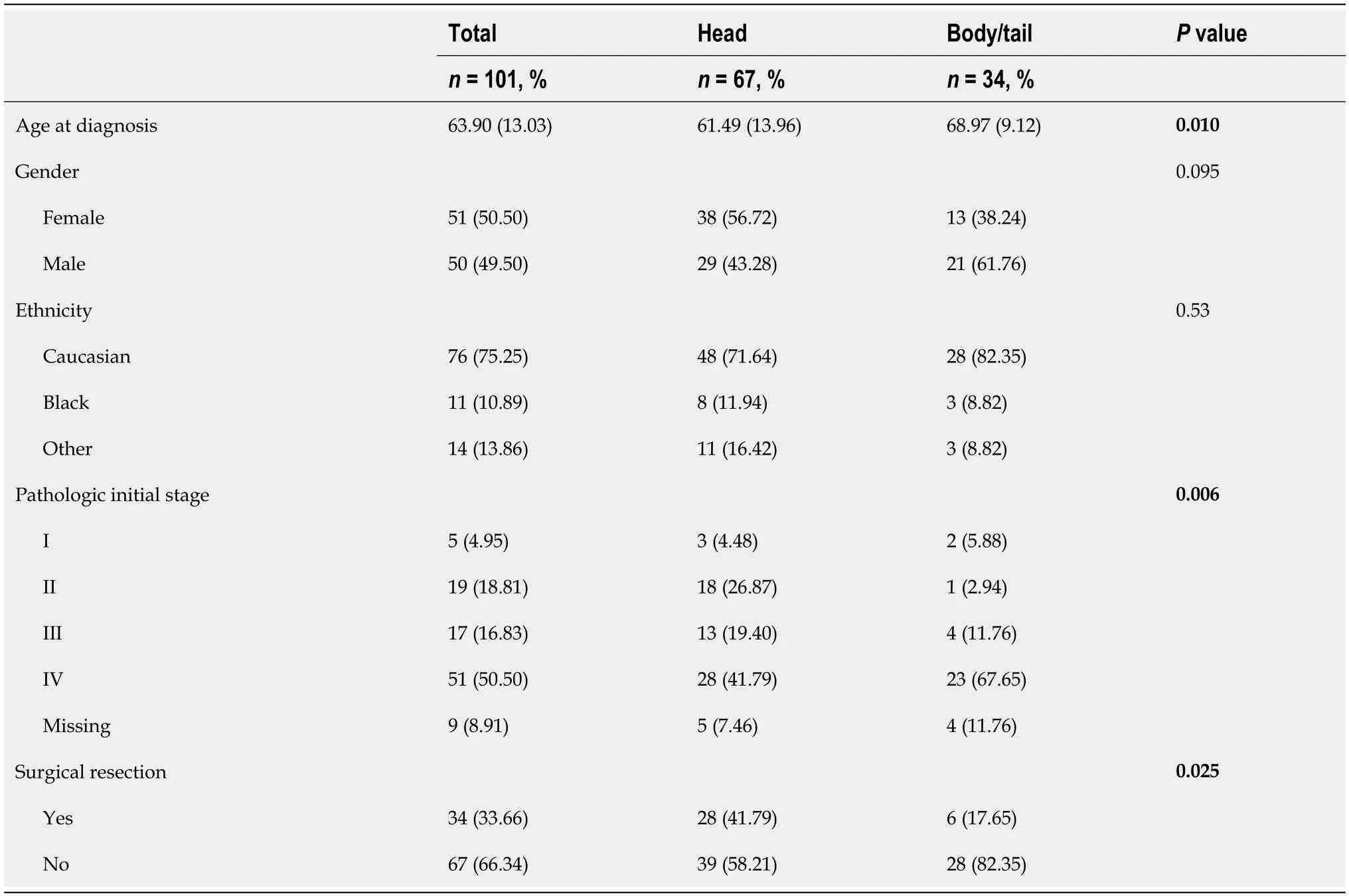
From July,2016 to June,2020,a total of 500 records was retrieved and 101 patients with complete medical records were included in the analysis.67 patients had PHC and 34 patients had PBTC.Compared to patients with PHC,patients with PBTC are older at diagnosis(68.97
61.49,
= 0.01),diagnosed at more advanced stage(
= 0.006)and are less likely to undergo surgical resection(
=0.025)(Table 1).There is no significant difference in gender,ethnicity between patients with PHC and patients with PBTC(
= 0.10 and 0.53 respectively).
Survival and tumor location
To study the relationships of pancreatic cancer location with molecular profiling,response to chemotherapy and survival.
Molecular profiling and tumor location
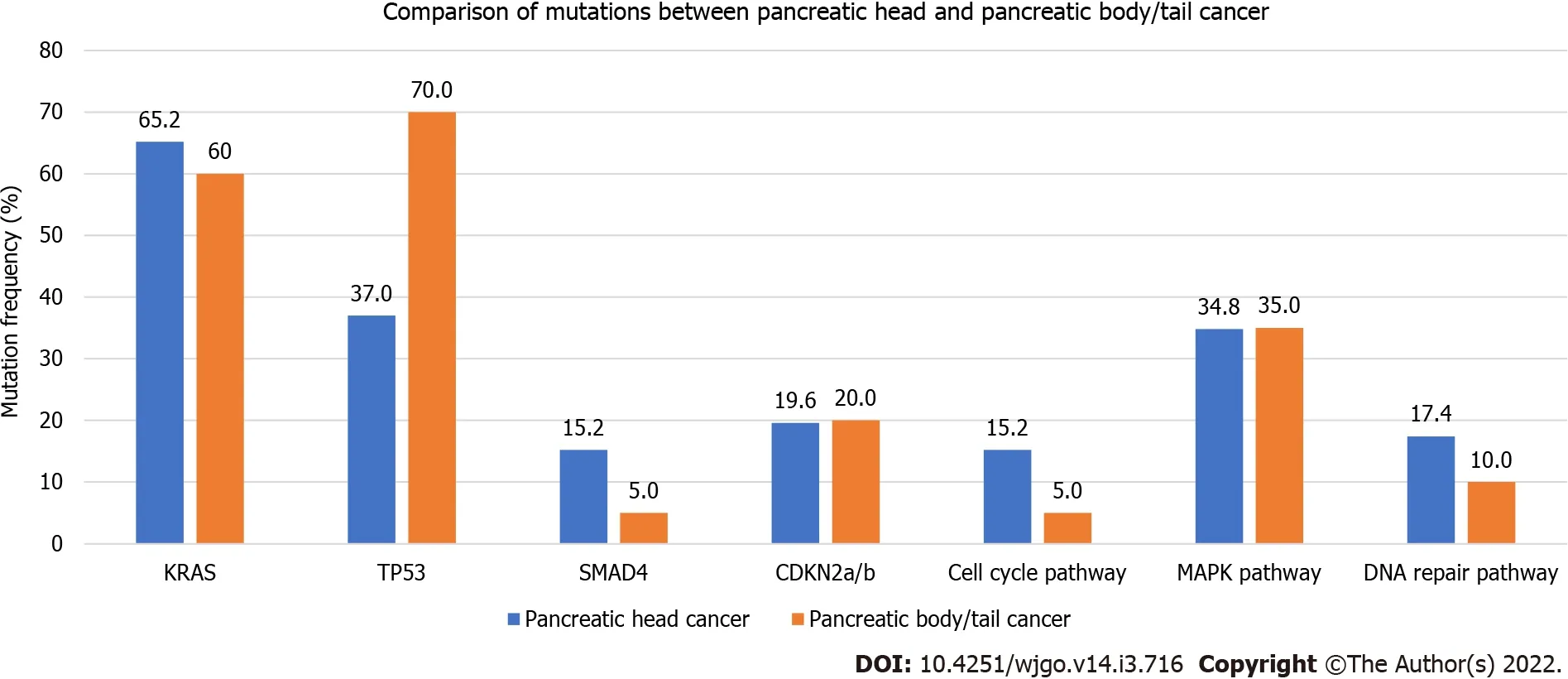
A total of 66 patients(46 PHC and 20 PBTC)who had complete medical records and molecular profiling were reviewed.20/66(30.3%)had molecular testing performed on biopsy specimen,24/66(36.4%)on peripheral blood,14/66(21.2%)on surgical resection specimen and the remaining on samples with unknown sources.Rates of pathogenic mutations were recorded and compared between PHC and PBTC(Figure 2).PHC and PBTC have similar tumor mutation numbers(
= 0.79).The most common mutations were KRAS mutations(63.6% in total,65.2% in PHC
60.6% in PBTC,
= 0.78),TP53 mutations(47.0% in total,37.0% in PHC
70.0% in PBTC,
= 0.03),SMAD mutations(12.1% in total,15.2% in PHC
5.0% in PBTC,
= 0.42)and CDKN2a/b mutations(19.7% in total,19.6% in PHC
20.2% in PBTC,
= 1.00).Only TP53 mutations were significantly different.12.1%% of the mutations were involved in cell cycle pathway(15.2% in PHC
5%% in PBTC,
= 0.47),34.9% in MAPK pathway(34.8% in PHC
35.0% in PBTC,
= 0.99)and 15.1% in DNA repair pathway(17.4% in PHC
10.0% in PBTC,
= 0.71).There were no differences in the mutations involved in these pathways.
Response to chemotherapy and tumor location
We hypothesize that PHC and PBTC are distinct diseases based on their embryological origins and current genetic profiling evidence.To further explore the impact of tumor location on molecular profiling,survival,and response to chemotherapy,we retrospectively reviewed patients with pancreatic cancer in our institution.
DlSCUSSlON
In this retrospective study,patients with PHC and PBTC were retrieved and the relationships of tumor locations with molecular profiling,overall survival,or response to chemotherapy were explored.Our study showed that patients with PBTC tend to present at later stages and are less likely to undergo resection,consistent with previous studies[11-13].PBTC are older at diagnosis in our study,which could have explained the lower resection rate.
The impact of tumor location on survival has been a controversy.Several population-based studies[2,3,11,14,15]reported contradictory survival of PBTC and PHC in the overall population;however,better survival in PBTC is seen in early stage patients,especially stage I and II.Winer
[14]examined the relationship of survival and tumor location in patients who had tumor resection and found that even though PHC were more of early stage at presentation and more likely to be resected,they tended to have higher grade,more positive lymph nodes and worse overall survival.The survival advantage of PBTC from this study was further supported by a single center study[16]which examined survival in matched stage II PBTC and PHC.Only one single center study[12]reported worse outcome for PBTC patients who had resection and among those patients with Stage I disease,the survival seemed to be better in PBTC however not statistically significant.Even though our study didn’t show a survival difference in PHC and PBTC,long-term survival was seen in three patients with Stage I/II PBTC who underwent resection.The findings from previous studies and our study suggest that resected early stage PBTC have better survival than those with PHC.
The four most common mutations in our study were KRAS,TP53,SMAD and CDKN2a/b mutations,which is consistent with previous reports[13,17].Among these most common mutations,only TP53 mutations were found to be significantly higher in PBTC in our study.Even though the frequency of SMAD mutations was higher in PHC(15.5%)compared to PBTC(5%),this result was not statistically significant because the total number of SMAD mutations observed was only 12.12% in our study.The lower frequencies of those mutations detected in our study could be explained by NGS being performed on insufficient tissues,as majority of samples were biopsy specimens or peripheral blood(66.7%).TP53 mutation is enriched in pancreatic squamous cell type[5]that is similar to lung squamous subtype,and might be similarly more sensitive to gemcitabine therapy.TP53 was also found to predict sensitivity to gemcitabine-based adjuvant therapy in a survival and mutational analysis from CONKOO-001 study[17].Based on these,our finding of more TP53 mutations in PBTC suggest gemcitabine-based adjuvant therapy to be considered in PBTC,especially in those who can’t tolerate FOLFIRINOX therapy.
To our knowledge,our study is the first study that looked at the impact of tumor location on response to different chemotherapy regimens.Neither PHC or PBTC responded differently to FOLFIRINOX based or gemcitabine-based chemotherapies,suggesting a universal poor prognosis of pancreatic cancer regardless of tumor location when compared based on chemotherapy response.However,differential response to targeted therapy or immunotherapy is yet to be explored given the different distribution of pancreatic cancer subtype like immunogenic.
Meanwhile the King was asking the Enchanter to what he was indebted for the honour of this visit, and on his replying that he would not say until the Queen was also present, messenger after messenger was dispatched to her to beg her immediate71 attendance
Limitations
Our study was a retrospective study in a single institution and a relatively small number of patients was retrieved.Due to the retrospective nature,the NGS platforms utilized,and the depths of sequencing were not uniform.This added another layer of bias in data interpretation.However,this reflects the real-world experience in many community and academic cancer centers that often rely heavily on commercial NGS platforms.Even though there is a trend to suggest better survival in early stage PBTC patients after resection,there were few patients and events in this subgroup and no definitive conclusion can be made.
CONCLUSlON
A larger and prospective study should be performed to explore the role of gemcitabine in PBTC.
ARTlCLE HlGHLlGHTS
Research background
Pancreatic head and pancreatic body/tail have different embryological origins.Tumors arising at different locations of pancreas might carry different mutations and respond differently to chemotherapy.
Research motivation
To better define pancreatic cancer and search for precision oncological targets that yield better outcomes.
Research objectives
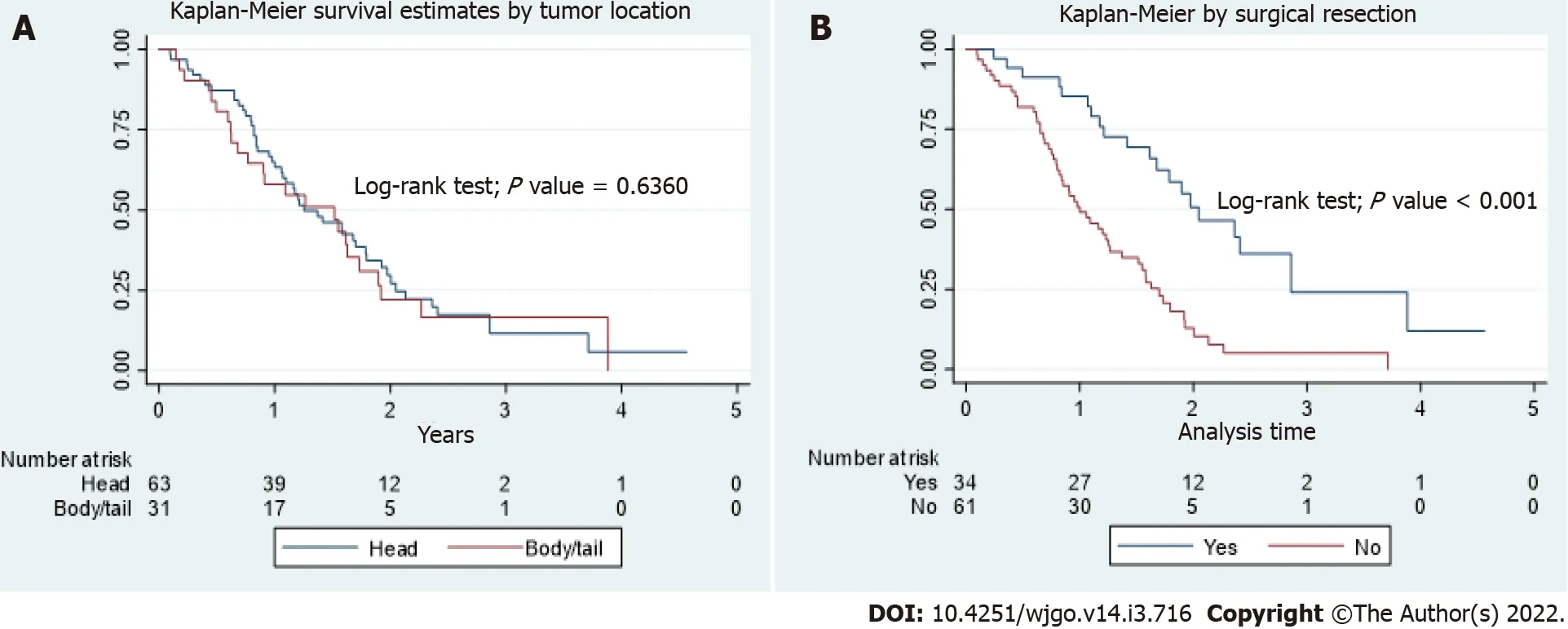
In the total population,the OS between PHC and PBTC was not statistically different(
= 0.64,Figure 1A).Patients who underwent surgical resection had better OS than patients who did not(
<0.001,Figure 1B),with a median OS of 2.05 years(interquartile range,1.21 to 2.86)and 1.00 year(interquartile range,0.77 to 1.70)respectively.There were no differences in survival between PHC and PBTC in those who underwent surgical resection,those who didn’t undergo surgical resection,or those who had Stage IV disease on presentation.In the subgroup of patients who had stage I and II disease,there were 3 patients with PBTC and those were long-term survivors.However,due to small number of patients,no definite conclusion can be made.
Mean and standard deviation were calculated for the continuous variables and frequency and percentage[
(%)]were calculated for those categorical variables.T-test was used to compare the mean of a continuous variables between the 2 groups of pancreatic cancer and the Fisher’s exact test was used to find the association between a patient’s characteristic and the pancreatic cancer’s groups.Kaplan Meier curves and Log-rank test were used to compare the survival time between the two location groups of pancreatic cancer.Stata/MP 16.1 for Windows was used to analyze the data.A test was considered statistically significant if the
value was < 0.05.
One of the littlest moths flew to ask the queen of the butterflies for help. The butterflies were too vain and selfish to give up any of their colors for neither the people nor the angels. So, the moths decided to try to make the rainbow themselves. They beat their wings very hard and the powder on them formed little clouds that the winds smoothed over like glass. Unfortunately, the rainbow wasn’t big enough so the moths kept giving a little more and a little more until the rainbow stretched all the way across the sky. They had given away all their color except brown, which didn’t fit into their beautiful rainbow.
Research methods
This is a single institution retrospective study that retrieved patients who carry a diagnosis of pancreatic cancer from July 2016 to June 2020.Patient demographics and molecular profiling information were reviewed and the relationship between tumor location and molecular profiling,response to chemotherapy and survival were analyzed.
Research results
Pancreatic head cancer and pancreatic body/tail cancer(PBTC)have different presentations but similar overall survival and response to chemotherapy.PBTC have significantly more TP53 mutations.
Research conclusions
Pancreatic squamous subtype shares similar molecular abnormalities with lung squamous subtype,which include loss of TP53,RB1,CDKN2A and PIK3CA,NOTCH1,NFE2L2,KDM6A and EP300 mutations.Squamous cell lung cancer was found to be more sensitive to platinum and gemcitabine combination therapy[9].When the combination therapy was tested in advanced pancreatic cancer,there was an improvement in overall survival,disease free survival and response rate,even though not statistically significant[10].Given that PBTC had more squamous subtype,it is possible that PBTC is more responsive to gemcitabine-based treatment.
Research perspectives
There is no difference in OS between PHC and PBTC but the long-term survival observed in early stage PBTC after resection suggests better survival in this subgroup of patients.PBTC has significantly more mutations involved in TP53 mutations and its predictive role in gemcitabine sensitivity should be explored in future studies.
FOOTNOTES
Sun K and Abdelrahim M designed the study;Sun K,Mylavarapu C,Crenshaw A and Zhang Y performed chart review;Hsu E,Xu JQ and Ordonez A analyzed the data;Niravath M and Jones SL performed bioinformatics and retrieved patient records;Sun K and Abdelrahim M wrote the manuscript;all authors have read and approve the final manuscript.
The youngest daughter performs these tasks with gentle reserve and is thus rewarded for her humble service (and perhaps her strong stomach).Return to place in story.
The study was reviewed and approved by the Houston Methodist Hospital Institutional Review Board,Approval No.MOD00002232.
Informed consent from patients was waived.
By this time he was somewhat alarmed, and did his best to put the ship about and get back to the river, but wind and tide were too strong for him, and he began to think of the number of times, from his childhood up, that he had been warned not to meddle82 with water
There is no conflict-of-interest.
Technical appendix,statistical code,and dataset available from the corresponding author at ksun2@houstonmethodist.org.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
United States
23. But the Three Bears never saw anything more of her: This story rarely ends with a lived happily ever after ending. The Bears have been the victims of breaking and entering as well as robbery. Goldilocks has survived and hopefully learned her lesson, but we usually aren t rooting for her anyway. Our best consolation58 is that the bears never see her again.
Kai Sun 0000-0001-5338-3920;Charisma Mylavarapu 0000-0003-1789-0022;Aubrey Crenshaw 0000-0002-6551-6265;Yuqi Zhang 0000-0001-8245-2091;Enshuo Hsu 0000-0002-8137-0171;Jiaqiong Xu 0000-0002-3463-2327;Marilyn Niravath 0000-0002-5653-965X;Stephen L Jones 0000-0002-1106-171X;Adriana Ordonez 0000-0001-9169-800X;Maen Abdelrahim 0000-0002-6631-5035.
Wu YXJ
A
On Christmas Day, all the joys of a close family relationship radiated throughout our parents home. The smells of roasted turkey, Southern?baked ham and homemade bread hung in the air. Tables and chairs were set up everywhere to accommodate toddlers, teenagers, parents and grandparents. Every room was lavishly1 decorated. No family member had ever missed Christmas Day with our mother and father.
Wu YXJ
1 Bastidas-Ponce A,Scheibner K,Lickert H,Bakhti M.Cellular and molecular mechanisms coordinating pancreas development.
2017;144:2873-2888[PMID:28811309 DOI:10.1242/dev.140756]
2 Lau MK,Davila JA,Shaib YH.Incidence and survival of pancreatic head and body and tail cancers:a population-based study in the United States.
2010;39:458-462[PMID:19924019 DOI:10.1097/MPA.0b013e3181bd6489]
3 Matsuno S,Egawa S,Fukuyama S,Motoi F,Sunamura M,Isaji S,Imaizumi T,Okada S,Kato H,Suda K,Nakao A,Hiraoka T,Hosotani R,Takeda K.Pancreatic Cancer Registry in Japan:20 years of experience.
2004;28:219-230[PMID:15084961 DOI:10.1097/00006676-200404000-00002]
4 Saad AM,Turk T,Al-Husseini MJ,Abdel-Rahman O.Trends in pancreatic adenocarcinoma incidence and mortality in the United States in the last four decades;a SEER-based study.
2018;18:688[PMID:29940910 DOI:10.1186/s12885-018-4610-4]
5 Bailey P,Chang DK,Nones K,Johns AL,Patch AM,Gingras MC,Miller DK,Christ AN,Bruxner TJ,Quinn MC,Nourse C,Murtaugh LC,Harliwong I,Idrisoglu S,Manning S,Nourbakhsh E,Wani S,Fink L,Holmes O,Chin V,Anderson MJ,Kazakoff S,Leonard C,Newell F,Waddell N,Wood S,Xu Q,Wilson PJ,Cloonan N,Kassahn KS,Taylor D,Quek K,Robertson A,Pantano L,Mincarelli L,Sanchez LN,Evers L,Wu J,Pinese M,Cowley MJ,Jones MD,Colvin EK,Nagrial AM,Humphrey ES,Chantrill LA,Mawson A,Humphris J,Chou A,Pajic M,Scarlett CJ,Pinho AV,Giry-Laterriere M,Rooman I,Samra JS,Kench JG,Lovell JA,Merrett ND,Toon CW,Epari K,Nguyen NQ,Barbour A,Zeps N,Moran-Jones K,Jamieson NB,Graham JS,Duthie F,Oien K,Hair J,Grützmann R,Maitra A,Iacobuzio-Donahue CA,Wolfgang CL,Morgan RA,Lawlor RT,Corbo V,Bassi C,Rusev B,Capelli P,Salvia R,Tortora G,Mukhopadhyay D,Petersen GM;Australian Pancreatic Cancer Genome Initiative,Munzy DM,Fisher WE,Karim SA,Eshleman JR,Hruban RH,Pilarsky C,Morton JP,Sansom OJ,Scarpa A,Musgrove EA,Bailey UM,Hofmann O,Sutherland RL,Wheeler DA,Gill AJ,Gibbs RA,Pearson JV,Waddell N,Biankin AV,Grimmond SM.Genomic analyses identify molecular subtypes of pancreatic cancer.
2016;531:47-52[PMID:26909576 DOI:10.1038/nature16965]
6 Hoadley KA,Yau C,Wolf DM,Cherniack AD,Tamborero D,Ng S,Leiserson MDM,Niu B,McLellan MD,Uzunangelov V,Zhang J,Kandoth C,Akbani R,Shen H,Omberg L,Chu A,Margolin AA,Van't Veer LJ,Lopez-Bigas N,Laird PW,Raphael BJ,Ding L,Robertson AG,Byers LA,Mills GB,Weinstein JN,Van Waes C,Chen Z,Collisson EA;Cancer Genome Atlas Research Network,Benz CC,Perou CM,Stuart JM.Multiplatform analysis of 12 cancer types reveals molecular classification within and across tissues of origin.
2014;158:929-944[PMID:25109877 DOI:10.1016/j.cell.2014.06.049]
7 Birnbaum DJ,Bertucci F,Finetti P,Birnbaum D,Mamessier E.Head and Body/Tail Pancreatic Carcinomas Are Not the Same Tumors.
2019;11[PMID:30965637 DOI:10.3390/cancers11040497]
8 Dreyer SB,Jamieson NB,Upstill-Goddard R,Bailey PJ,McKay CJ;Australian Pancreatic Cancer Genome Initiative,Biankin AV,Chang DK.Defining the molecular pathology of pancreatic body and tail adenocarcinoma.
2018;105:e183-e191[PMID:29341146 DOI:10.1002/bjs.10772]
9 Scagliotti GV,Parikh P,von Pawel J,Biesma B,Vansteenkiste J,Manegold C,Serwatowski P,Gatzemeier U,Digumarti R,Zukin M,Lee JS,Mellemgaard A,Park K,Patil S,Rolski J,Goksel T,de Marinis F,Simms L,Sugarman KP,Gandara D.Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer.
2008;26:3543-3551[PMID:18506025 DOI:10.1200/JCO.2007.15.0375]
10 Heinemann V,Quietzsch D,Gieseler F,Gonnermann M,Sch?nek?s H,Rost A,Neuhaus H,Haag C,Clemens M,Heinrich B,Vehling-Kaiser U,Fuchs M,Fleckenstein D,Gesierich W,Uthgenannt D,Einsele H,Holstege A,Hinke A,Schalhorn A,Wilkowski R.Randomized phase III trial of gemcitabine plus cisplatin compared with gemcitabine alone in advanced pancreatic cancer.
2006;24:3946-3952[PMID:16921047 DOI:10.1200/jco.2005.05.1490]
11 van Erning FN,Mackay TM,van der Geest LGM,Groot Koerkamp B,van Laarhoven HWM,Bonsing BA,Wilmink JW,van Santvoort HC,de Vos-Geelen J,van Eijck CHJ,Busch OR,Lemmens VE,Besselink MG;Dutch Pancreatic Cancer Group.Association of the location of pancreatic ductal adenocarcinoma(head,body,tail)with tumor stage,treatment,and survival:a population-based analysis.
2018;57:1655-1662[PMID:30264642 DOI:10.1080/0284186X.2018.1518593]
12 Sheng W,Dong M,Wang G,Shi X,Gao W,Wang K,Song H,Shi G,Tan X.The diversity between curatively resected pancreatic head and body-tail cancers based on the 8th edition of AJCC staging system:a multicenter cohort study.
2019;19:981[PMID:31640615 DOI:10.1186/s12885-019-6178-z]
13 Zhang X,Feng S,Wang Q,Huang H,Chen R,Xie Q,Zhang W,Wang A,Zhang S,Wang L,Yao M,Ling Q.Comparative genomic analysis of head and body/tail of pancreatic ductal adenocarcinoma at early and late stages.
2021;25:1750-1758[PMID:33452856 DOI:10.1111/jcmm.16281]
14 Winer LK,Dhar VK,Wima K,Morris MC,Lee TC,Shah SA,Ahmad SA,Patel SH.The Impact of Tumor Location on Resection and Survival for Pancreatic Ductal Adenocarcinoma.
2019;239:60-66[PMID:30802706 DOI:10.1016/j.jss.2019.01.061]
15 Zheng Z,Wang M,Tan C,Chen Y,Ping J,Wang R,Liu X.Disparities in survival by stage after surgery between pancreatic head and body/tail in patients with nonmetastatic pancreatic cancer.
2019;14:e0226726[PMID:31856205 DOI:10.1371/journal.pone.0226726]
16 Ling Q,Xu X,Ye P,Xie H,Gao F,Hu Q,Liu Z,Wei X,R?der C,Trauzold A,Kalthoff H,Zheng S.The prognostic relevance of primary tumor location in patients undergoing resection for pancreatic ductal adenocarcinoma.
2017;8:15159-15167[PMID:28122349 DOI:10.18632/oncotarget.14768]
17 Sinn M,Sinn BV,Treue D,Keilholz U,Damm F,Schmuck R,Lohneis P,Klauschen F,Striefler JK,Bahra M,Bl?ker H,Bischoff S,Pelzer U,Oettle H,Riess H,Budczies J,Denkert C.TP53 Mutations Predict Sensitivity to Adjuvant Gemcitabine in Patients with Pancreatic Ductal Adenocarcinoma:Next-Generation Sequencing Results from the CONKO-001 Trial.
2020;26:3732-3739[PMID:32234756 DOI:10.1158/1078-0432.CCR-19-3034]
 World Journal of Gastrointestinal Oncology2022年3期
World Journal of Gastrointestinal Oncology2022年3期
- World Journal of Gastrointestinal Oncology的其它文章
- Re:Association between intestinal neoplasms and celiac disease -beyond celiac disease and more
- Association of Blastocystis hominis with colorectal cancer:A systematic review of in vitro and in vivo evidences
- Clinical efficacy and prognostic risk factors of endoscopic radiofrequency ablation for gastric low-grade intraepithelial neoplasia
- Computed tomography-based radiomic to predict resectability in locally advanced pancreatic cancer treated with chemotherapy and radiotherapy
- Cost-effective low-coverage whole-genome sequencing assay for the risk stratification of gastric cancer
- RNA-Seq profiling of circular RNAs in human colorectal cancer 5-fluorouracil resistance and potential biomarkers