
Fibrous histiocytoma of the spermatic cord 1 case and review of the literature
2022-01-04 07:57:16HuaKangWangHuijuanZhouGaiHangQuanWeYuYangWangBoChen
Cancer Advances 2021年6期
Hua-Kang Wang,Hui-juan Zhou,Gai Hang,Quan We,Yu-Yang Wang,Bo Chen*
1Inner Mongolia Medical University,Huhehot 010000 China.2Inner Mongolia Autonomous Region Tongliao City Hospital,Tongliao 028000,China.
Abstract Objective: The diagnosis and treatment of this disease were discussed based on the relevant literature and the clinical data of spermatic fibrous histiocytoma in our hospital.Methods:The clinical data of 1 case of spermatic cord fibrous histiocytoma admitted to urology department were retrospectively analyzed, combined with relevant literature review and discussion.Results: After surgical radical treatment, the pathological result was fibrous histiocytoma.Conclusion: Spermatic cord fibrous histiocytoma is a rare tumor of genitourinary system.The diagnosis is mainly based on pathological results.Surgery is the first choice for treatment.Adjuvant radiotherapy and chemotherapy are not effective and the prognosis is poor.Regular postoperative review is required.
Keywords:spermatic cord, fibrohistiocytoma, pathology
Preface
Fibrohistiocytoma is a kind of mesenchymal-derived tissue-derived tumor, which is a soft tissue sarcoma formed by the differentiation of primitive mesenchymal tissue into fibrous tissue cells, accounting for less than 1% of all solid tumors [1].It can occur in many parts of the body, but fibrous histiocytoma occurring in the seminal cord is very rare.The following is a report of a patient admitted to the Department of Urology of our hospital, together with its clinical characteristics and diagnosis and management, and the related literature to discuss the diagnosis, management and prognosis of this disease.
Clinical information
A 58-year-old male patient was admitted to hospital for 1 year due to left inguinal mass.The patient had found a mass in the left inguinal region without apparent cause and was not treated systematically.Within one year, the tumor gradually increased, no tenderness and pain, no fever, nausea and vomiting.No frequent urination, urgency,pain, no dysuria, hematuria, pyuria.Physical examination : a solid mass can be palpated in the left inguinal region, about 2.0 cm × 2.0 cm in size, without obvious tenderness and smooth surface ; urinary color Doppler ultrasound : 2.3cm × 1.7cm round low mixed echo mass can be seen above the outer ring of left inguinal region, with clear boundary and uneven internal echo.CDFI showed a small number of internal and peripheral blood flow signals.CT examination: the left inguinal region visible round soft tissue shadow, tumor boundary is still clear, internal density is not uniform.Patients underwent radical resection of tumor.During the operation, the tumor was located between the inner and outer ring of the left groin,surrounded by spermatic cord, tough, and obvious adhesion with surrounding tissues.Postoperative pathology showed a round tumor with a size of 2 cm × 2 cm × 2 cm.The boundary was clear, and the section was gray, tough, without bleeding and necrosis, without invasion of testis and epididymis.Under light microscope, it can be seen that the tumor boundary is relatively clear, and the short spindle tumor cells in most regions are loose fascia-like arrangement, and the extracellular space is rich in collagen fiber bundles.The tumor cells were fibroblast-like (Figure 1 ①②), with clear boundary, basophilic cytoplasm, vacuolated nucleus, obvious eosinophilic nucleoli and active mitotic activity.We can see scattered mononuclear and multinucleated giant cells, rich cytoplasm, large nuclei, deep staining,irregular.The tumor cells in the pleomorphic region are abundant,with large nuclei and obvious heteromorphism, forming a fuzzy sheet-like structure, and a large number of pleomorphic giant cells can be seen.There were more lymphocyte infiltration in the front of tumor invasion.Immunohistochemical staining : CD68 ( + ) (Figure 1 ③),Vimentin ( + ) ( (Figure 1 ④), S-100 protein ( ?) ( (Figure 1 ⑤),Desmin(?)((Figure 1 ⑥),EMA(?)((Figure 1 ⑦ ),CD34(?)((F igure 1 ⑧).Pathological results : spermatic fibrous histiocytoma ( mal ignant ), testis and epididymis without tumor involvement.Patients had good postoperative healing and refused to receive adjuvant radiotherapy and chemotherapy.Follow-up for 6 months showed no recurrence or metastasis.
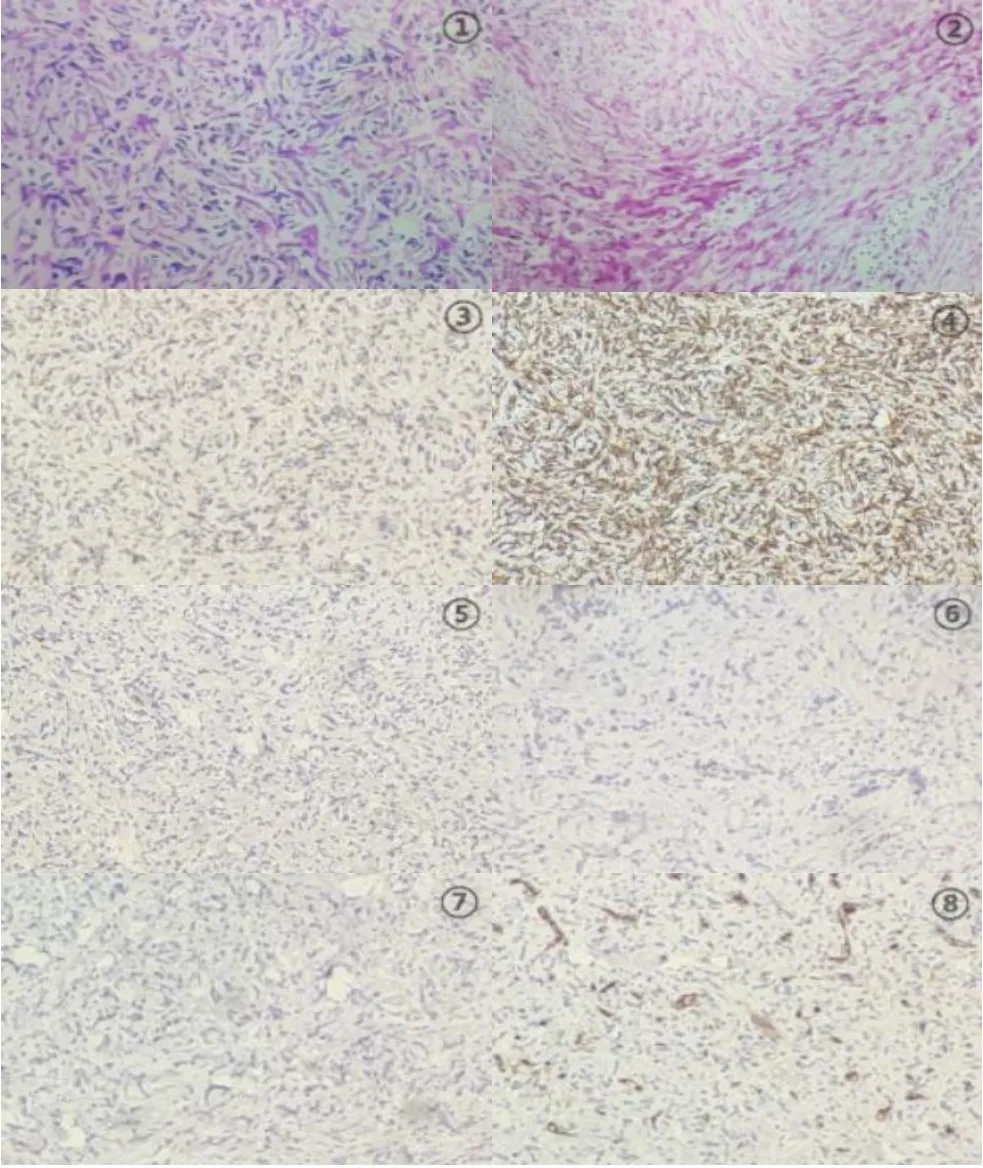
Figure 1.①② Pathologyof spermatic cord mass(100×);③ CD68(+);④ Vimentin (+ );⑤ S-100 protein ( ?); ⑥ Desmin ( ?); ⑦ EMA( ? ); ⑧ CD34 ( ? ); ③-⑧Immunohistochemical results of postoperative pathology(100×).
Discussion
Fibrohistiocytoma originates from the mesoderm and was first mentioned by Klemperer and Rabin in 1931[2] and first reported by O'Brien in 1964[3].Fibrohistiocytoma can occur in all parts of the body, with the proximal extremities (70%) and the deep soft tissues of the retroperitoneum (16%) being the most common and the inguinal region being extremely rare [4], while those occurring in the seminiferous cord are even rarer.In this study, related literature was searched, of which 42 cases were reported in foreign literature [5-7],and 15 cases were reported in domestic literature [8-9].Spermatic fibrous histiocytoma in adults is rare and occurs in elderly patients over 50 years old.The pathogenesis is still not well understood, and some studies suggest that it maybe related to local surgery,pelvic radiotherapy, foreign body reaction, and scar repair.
The main clinical manifestation of fibrous histiocytoma of the spermatic cord is a painless groin area or a gradually enlarged mass in the scrotum.Ultrasound examination is the main examination method, which can distinguish whether the lesion is located in the testis, and is helpful for the differential diagnosis of other lesions.Although fibrous histiocytoma of the spermatic cord often appears as a solid, vascular-rich, heterogeneous, hyperechoic mass on ultrasound,this group of cases appears as a hypoechoic mass similar to benign tumors [10].MRI helps to clarify the size, location, tissue composition, extent of invasion and pelvic lymph nodes of the tumor,and provides an important basis for tumor staging and surgical methods.MRI often manifests as a mass with uneven signal density,reflecting the complex histological components of the tumor [11].CT examination of this group of cases showed clear boundaries and uneven density consistent with previous literature reports.However,imaging features are not specific in distinguishing spermatic cord fibrous histiocytoma, so we must rely on pathological examination.Tumor puncture or biopsy can clarify the nature and histological type of the lesion, but the morphology of multiple spindle cell soft tissue tumors overlaps with each other, and there are many lesions that need to be differentiated and diagnosed, and biopsy is difficult to carry out due to the special location and physiological role of the spermatic cord.It is easy to cause misdiagnosis and missed diagnosis.
Spermatic fibrous histiocytoma is mainly divided into four pathological types, among which striated-polymorphism is the most common (83%), followed by giant cell type (9%), inflammatory type(6%) and mucinous type (2 %)[12].However, the diagnosis is mostly exclusionary.It can be diagnosed after excluding other common histological types and other pleomorphic tumors such as stromal tumor, malignant mesothelioma, malignant melanoma, malignant peripheral nerve sheath tumor, synovial sarcoma, etc.Immunohistochemistry plays an important role in identification and diagnosis.There was no absolute specific tumor marker in the immunohistochemistry of fibrous histiocytoma, and occasional focal expressions of CD68 ( + ), Vimentin ( + ), S-100 protein ( ?),Desmin ( ?), EMA ( ?) CD34 ( ?) were observed.Our report has similar results.
Fibrohistiocytoma of the spermatic cord is rare.The treatment recommendations are all based on case reports, small sample analysis and literature review.Therefore, there is currently no uniform treatment standard for this disease.Radical mass resection and testicular spermatic cord and extensive surrounding soft tissue resection are the current first choices.Surgical methods.However, due to the limitation of the anatomical location and the tumor often invading the surrounding tissues, it is often difficult to complete a wide and far enough tumor margin [13].This group of cases underwent radical mass and testicular spermatic resection after detailed explanation of the condition.Because the role of preventive lymph node dissection has not yet reached a consensus.Therefore,this disease rarely invades regional lymph nodes, and generally causes tumor recurrence and spread through infiltration of surrounding soft tissues.Therefore, preventive retroperitoneal lymph node dissection is not recommended for this disease [14].At present, there is no consensus on the best adjuvant treatment strategy for spermatic fibrous histiocytoma.Some studies have proposed common chemotherapeutic drugs CTX and Aadriamycin [15].However, due to the small number of postoperative chemotherapy samples and the short follow-up time, the prognosis is not clear.The postoperative effects of adjuvant chemoradiation are also the same.Some small sample analysis studies have shown that postoperative radiotherapy can reduce the recurrence rate.Therefore, postoperative adjuvant radiotherapy is recognized by more and more clinicians.
Conclusion
In summary, although there is currently no uniform diagnosis and treatment standard for spermatic fibrous histiocytoma, its clinical manifestations are mainly painless masses in the groin or scrotum.The preoperative auxiliary diagnosis can refer to imaging, and the diagnosis must rely on Pathological and immunohistochemical examination results.At present, the preferred treatment method recommended is radical resection, and there is still academic controversy about whether postoperative radiotherapy and chemotherapy are available.Regular inspections and timely surgical treatment are the best options for this disease, providing the possibility for a good prognosis.The prognosis of this disease is poor and should be followed up for a long time.

- Cancer Advances的其它文章
- Study on the Correlation between Syndrome Differentiation of Malignant Pleural Effusion Treated by External Treatment of Traditional Chinese Medicine and Immunohistochemistry of Biopsy Tissue Based on Medical Video-assisted Thoracoscope
- Lipid peroxidation and cancer
- Reporting Quality Assessment of systematic reviews on Quality of Life in Patients with Enterostomy in China
- "Endogenous wind"Theory theory in the prevention and treatment of anti-tumor treatment-related adverse reaction related research progress