
The preferences and values of patients treated with acupuncture for cancer pain:a qualitative systematic review
2021-10-08 14:20:16JieYunLiJingWenLiMiaoLiKangLeGuoYongFengWangandKeHuYang
Cancer Advances 2021年4期
Jie-Yun Li,Jing-Wen Li,Miao Li,Kang-Le Guo,Yong-Feng Wang,and Ke-Hu Yang
Jie-Yun Li,Miao-Li and Ke-Hu Yang are with Evidence-Based Medicine Center,School of Basic Medical Sciences,Lanzhou University,Lanzhou,730000,China.
Jing-Wen Li,Kang-Le Guo snd Ke-Hu Yang are with Evidence Based Social Science Research Center,School of Public Health,Lanzhou University,Lanzhou,730000,China.
Yong-Feng Wang is with Gansu University of Chinese Medicine,Lanzhou,730000,China.
Ke-Hu Yang is with Evidence-Based Medicine Center,School of Basic Medical Sciences,Lanzhou University,Evidence-Based Medicine Center,School of Basic Medical Sciences,No.199 Donggang West Road,Lanzhou,730000,China.E-mail:kehuyangebm2006@126.com(Corresponding author).
Abstract—Background:Understanding values and preferences in the context of personal,physical,emotional,relational,and social factors is important in optimizing cancer patient counselling,facilitating treatment decisionmaking,and improving guideline recommendations in treating cancer pain patients.Objective:To systematically review the available evidence regarding the values,preferences,and expectations of acupuncture for patients with cancer pain.Methods:A systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was conducted.Eight databases were searched without time limits for eligible studies up to April 26,2021.Reference lists of included articles were also searched manually and authors were contacted to inquire about other relevant papers.The quality of the studies was appraised using the Critical Appraisal Skill Program Qualitative Appraisal Checklist (CASP) for studies.This research was registered on PROSPERO with number CRD42020213396.Results:A total of eight studies published in period from 2002 to 2020 were identified from 8 studies involving 2,835 patients.The number of participants in each study ranged from 76 to 706.The quality of the eight included studies was considered high as judged by the CASP tool.Safety is the main factor influencing patients'willingness and preference to accept acupuncture treatment.Human race,education,gender,and knowledge of acupuncture were potentially correlated with patients'preferences.Patients with moderate to severe pain were more likely to use acupuncture than those with mild pain.Conclusion:The preferences and values of patients with cancer pain to receive acupuncture treatment are mainly related to the safety of acupuncture,the degree of cancer pain and demographic characteristics.It is hoped that future high-quality studies could further confirm our conclusions.
Key words—Acupuncture,Cancer,Pain management,Preference,Willing,Systematic review
INTRODUCTION
When patients are faced with different medical regimens,their clinical choices are often affected by their own values and preferences,which means they may have a great tendency of one specific treatment [1].Some of these personal preferences and values are derived from subjective perceptions of a series factors (e.g.,expectation of treatment,patient experience,choice of needs,perception of treatment methods,and confidence in medical facilities and staff [2,3],and various personal internal factors (e.g.,gender and demographic characteristics) [4,5].Many studies have shown that patients'preferences and values can affect the effectiveness and safety of a specific intervention to a certain extent [6,7].In particular,under the concept of evidence-based medicine,clinical decision-making needs to be patient-centered,which means that a high-quality decision should be informed and consistent with the patient's preferences and values [8,9].
Cancer pain refers to the pain in the process of the occurrence and development of malignant tumor,which is caused indirectly by tumor itself and various treatment measures (i.e.,surgery and drugs) [10].It is shown that 40% of the patients with early or mid-term cancer,and 90% patients with advanced cancer suffered from moderate or severe cancer pain.Unfortunately,70% of them were not effectively controlled in cancer pain [11].Although the"three ladders therapy" proposed by WHO has been widely used in clinic,a treatment of cancer pain with a combination of opioids with different pharmacodynamic grades [12],to the abuse of opioids has become a crisis in pain management due to its addictiveness and adverse reactions [13].Acupuncture is one of the common interventions in traditional Chinese medicine,and has been widely used in clinical pain management [10].Acupuncture analgesia relieves pain by activating specific areas called acupoints on the patient’s body,with multiple transmitters and modulators of endogenous opioids,serotonin,glutamate,norepinephrine,dopamine,acetylcholine,and orexin A are involved [14].A recent metaanalysis found that acupuncture and/or acupressure was significantly associated with reduced cancer pain and decreased use of analgesics [10].In light of the growing number of studies exploring the preference and values of patients with cancer pain,we conducted a qualitative systematic review of the available evidence on preferences and values of patients treated with acupuncture for cancer pain,in order to provide more effective evidence for clinical decision-making.
METHODS
This qualitative systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)guidelines [15].The protocol of this review was registered with PROSPERO (Number:CRD42020213396).
Data sources and search strategy
The Web of Science,Embase,PubMed,Cochrane Library,CNKI,VIP,WANFANG and CBM online databases were extensively searched,with the final search completed on April 26,2021.The search strategy was developed using the following keywords:"neoplasms","cancer","pain","patient preference","patient value","acupuncture" and "electroacupuncture".The details of search strategy were shown in Supplemental material.Publication status,language,or publication date were not restricted.
Selection of studies
The inclusion criteria were as follows:1) Studies on the preferences and values of acupuncture treatment in patients with various cancer pain; 2) Participants were all adults,or more than 80% of the participants were adults (≥ 18 years of age).
We excluded animal experiments,non-acupuncture intervention studies,and studies that were duplicate reports or with insufficient data on the preferences and values of cancer pain patients,such as protocols,conference proceedings,or abstracts.
Before the inclusion or exclusion of each article,we carried out the calibration work.In the process,each researcher evaluated the same studies and discussed any different opinions until each of reviewer clarified the criteria and reached a consensus [16].Two reviewers (JW and KL) independently conducted screening and data extraction,with any differences resolved by consultation with a third reviewer.After removing duplicate articles,two reviewers screened the titles and abstracts according to the inclusion criteria and then determined the final studies for inclusion by reading the full text.For the study with missing data or incomplete data,contact the original author to supplement the required information [17].
Data extraction and quality assessment

Fig.1.PRISMA flow diagram
Two predesigned tables of qualitative studies were used to collate the extracted data respectively.The basic information of each included study was extracted and coding in Table 1,including study design,the setting of trials,study period,number of participants at different stages of trials,the type and stage of the patient's cancer,degree of their pain and patient's sociological background.Both two reviewers independently extracted data.In case of different opinions,the researchers would reach a consensus with the assistance of the third researcher.
The appropriateness of including or excluding qualitative studies in a synthesis based on an appraisal of their quality remains contentious.An assessment of the quality of studies was undertaken using the Critical Appraisal Skills Programme (CASP) in order to gain a richer understanding of the methodological choices within each study [18].Appraisal was blinded,agreement attained and all studies assessed met criteria for research aims,qualitative methodology/design,recruitment strategy,data collection methods/analysis,consideration of researcher participant relationship and presentation of findings.
Data synthesis and analysis
A "five step" approach was used to synthesize the results,including the collection and analysis of qualitative data.1)Identified key topics and coded one or two eligible studies in qualitative study; 2) Basic data extraction tables were designed based on the pilot coding; 3) All categories were identified in the study using an iterative process,and main topics were then refined; 4) The quantitative data were transformed into qualitative data by using the critical metanarrative synthesis; 5) Through the overview of first four steps,the narrative of identification of key topics were extracted and guide data synthesis following.
RESULTS
Eight electronic databases retrieved a total of 581 citations.This total reduced to 484 citations once duplicates were removed.After scanning titles and abstracts against the inclusion criteria,29 citations remained requiring further review by full text article.More detailed full text analysis reduced the set to 8 articles for the final synthesis.This process is outlined in Figure 1.
Characteristics of studies
Two individual countries were represented across the eight studies,five from the United States and three from Sweden.The median date across all studies was 2015(range:2002-2020).As shown in Table 1,the study design of included studies consisted of six cross-sectional studies,one single arm non-randomized controlled trial and one open label trial,involving 2,835 participants,mean age 58± 19.9 years.All eight studies reported the study sites,two of them were from multicenter [20,26],and six from the single center [19,21-25].Seven studies reported cancer types [19,21-26]and five reported the cancer stage [19,21,22,25,26].Six studies were reported the outcomes of breast cancer from 570 participants (20.11%),followed by the patients suffered in lung cancer (9.8%),urinary cancer(9.2%) and gastrointestinal cancer (8.6%).All studies reported the gender ratio of the patients included.Social conditions of the patients were reported in seven studies,such as education level [19,22-25],occupation,and race[23-25].
Main findings
Three themes were identified:1) Feasibility analysis of acupuncture treatment for cancer patients (three studies [19,20,23],314 participants),2) Acceptance or attitude barriers of acupuncture treatment for cancer patients (five studies [21,22,24-26],2,521 participants),3) Statistical analysis of sociodemographic factors related to patients participating in acupuncture treatment of cancer pain (three studies [21,22,25],1,293 participants).
In Table 2,five studies reported the reasons of why cancer patients were willing to accept acupuncture treatment and the existing attitude disorders,four studies reported the statistical analysis of sociodemographic factors [21,22,25].Four studies’ response rate during follow-up was lower than 80% [19,23-25].Three studies showed that race and education level were important factors to predict acupuncture pain preference [22,24,25].Two studies have shown that young patients and highly educated people believe that acupuncture is more effective in treating cancer pain than other interventions [24,25].Two studies indicated that patients with moderate and severe pain were more likely to receive acupuncture treatment than those with mild pain [23,24].One study indicated that patients with prostate cancer may be less likely to use acupuncture therapy than breast cancer patients [32].
No adverse reactions related to acupuncture were reported.
When asked about the value of acupuncture treatment,68 patients (86%) thought it was a very important treatment.11% of patients thought it has a better effectiveness when acupuncture adjuvant chemotherapy,but 3% thought it was useless.90% of the patients were willing to continue to receive acupuncture treatment regardless of their reaction after treatment.Although there is no study detailed report on whether to obtain the informed consent of patients and their families,there are a certain potential bias and influence.
The certainty of evidence which describing values and preferences of qualitative study was assessed by CASP.Among them,four studies (57.1%) were assessed as high risk of bias due to the lack of effectiveness of measurement tools,because the relationship between researchers and participants was not reported,and the details of data analysis process were less [21,24,26].As assessed the certainty in Table 3,123 cancer patients with different symptoms expressed their views on the availability and effectiveness of acupuncture in relieving cancer pain in Johnstone et al.[20].The researchers surveyed 79 patients(89%) by telephone.Most of them (60%) had relieved the pains with at least 30%.One third of the patients thought the cancer pain symptoms did not change.
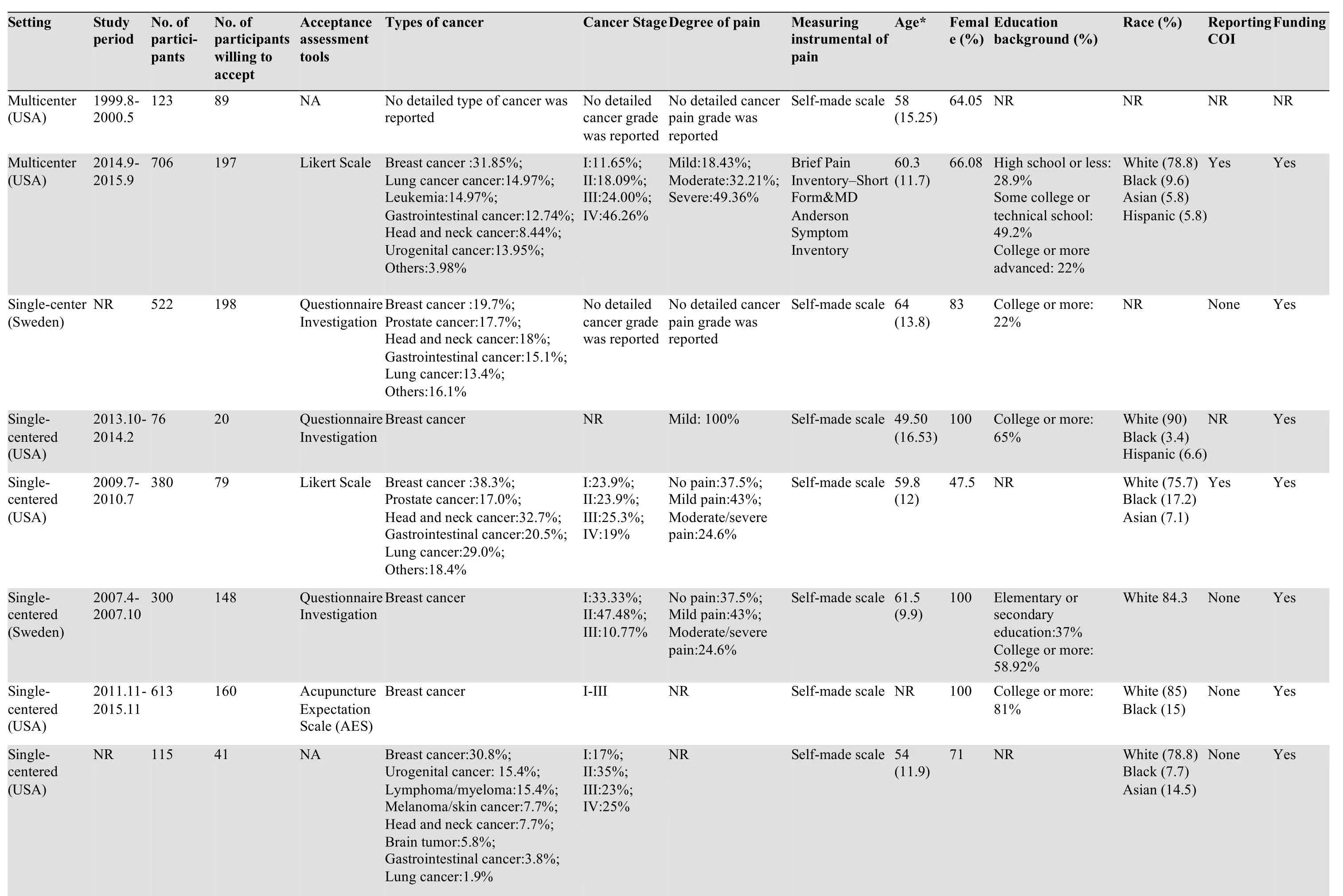
Table 1 Characteristics of studies
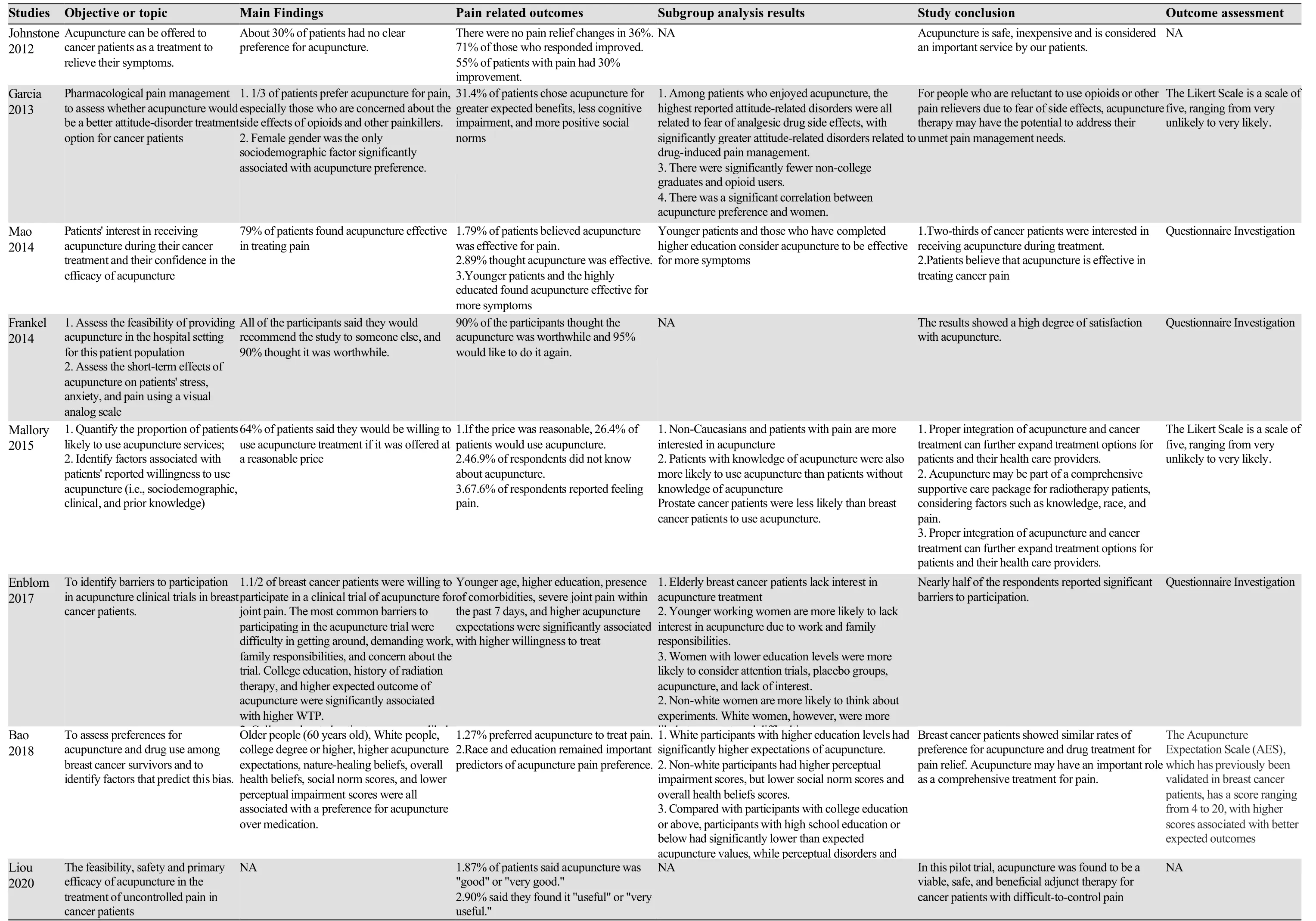
Table 2 Main findings of included studies
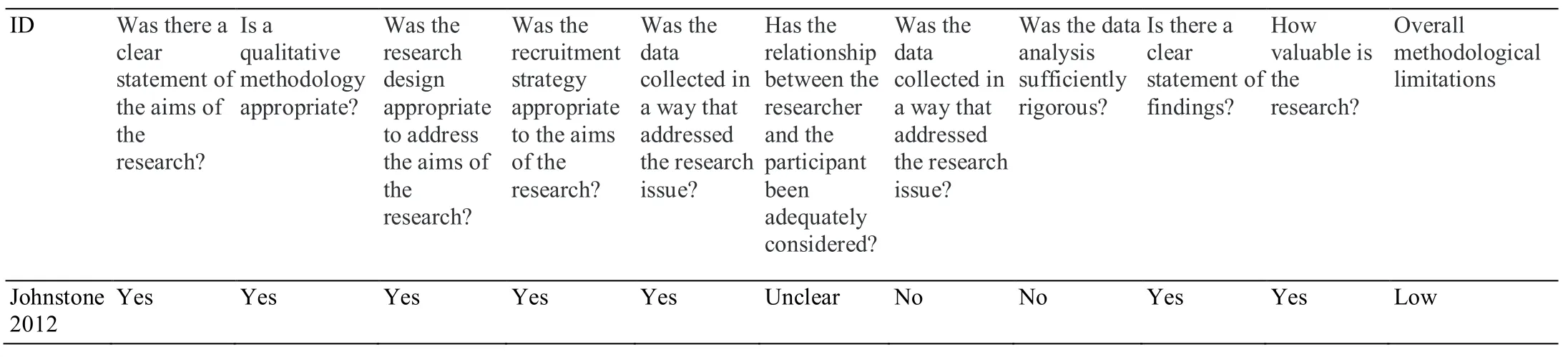
Table 3 Risk of bias of qualitative study
Motivation for patients
Five studies reported the reasons for the use of acupuncture [21,22,24-26].A cross-sectional study of cancer pain patients in the United States showed that fear of side effects of painkillers predicted a preference for acupuncture therapy [26].Of the 628 patients,197 (31.4%)preferred acupuncture,the strongest attitudinal barriers were fear of addiction to painkillers and fear of side effects such as nausea and constipation.146 patients (23.3%)preferred analgesics,and the remaining 285 (45.4%) hadno obvious preference for cancer pain treatment.
In one study,cancer pain patients were willing to receive acupuncture therapy and expressed their belief in natural treatment [25].One study showed that 69% of patients were willing to accept acupuncture because of their curiosity in acupuncture [24].According to the studies by Johnstone [20]and Enblo [24],reasonable price was also a considerable reason.Liou et al.[26]indicated that women with cancer pain have a more positive attitude towards acupuncture treatment than men,which is also related to the high participation rate of women (60.63%).
The overall certainty of the evidence was low.Due to none of the studies reported in detail the specific sampling method of the subjects; The response rate of two studies[19,23]during follow-up was lower than 80%; Three studies [21,23,24]were found to have a high risk of bias due to the lack of effectiveness of measurement instruments.
DISCUSSION
In the international context of the increasing prevalence of opioids,public concern about the potential risks associated with the use and abuse of opioids has been exacerbated [27].This systematic review illustrated that cancer pain patients prefer acupuncture treatment due to its safety.As a complementary medicine focusing on systemic treatment,the side effects of acupuncture are rarely known[28,29].In the three cross-sectional studies we included[24-26],nearly a quarter of survivors strongly preferred acupuncture for pain relief,a quarter preferred medication,and half did not.One fifth opioid patients reported took inadequate doses to control pain in order to reduce their concerns about taking opioids [25].Patients who reported having greater attitudinal barriers to medication pain,especially those who were concerned about the side effects of opioids and other analgesics,were significantly more likely to be treated with acupuncture [19].Acupuncture can potentially solve the “unmet pain management needs” of patients who are unwilling to use pain relieving drugs because of their fear of side effects [30].
Multivariate analysis showed that health attitude and belief were more important than sociodemographic factors(such as race and education level) in predicting pain management preference.Our study identified several sociodemographic attitudes and beliefs associated with acupuncture over drug preference,including gender,race,education level,expectations of acupuncture treatment,social norms and overall health belief scores,and lower perceived barriers.A study clearly suggests that female gender is the only sociodemographic factor significantly related to acupuncture preference [26].This is consistent with other studies,which shown that women could generally tolerate higher levels of pain [31,32].
There has no definitive conclusion as to whether different races have different preferences for acupuncture treatment of cancer pain.Some studies found that nonwhite people are positively correlated with the willingness to use acupuncture [21],while some studies showed that non-white patients with lower education level were less likely to use acupuncture [25].Some study analyzed the fear of the acupuncture,which showed they feel uncomfortable may be due to the abuse of blacks in historical research and the health inequality experienced by minorities for a long time [33,34].Racial differences may be affected by other factors (e.g.,perceptions of the insurance system) that we did not assess in our previous studies [35,36].Further research is needed to clarify the various factors that affect cancer patients' perception of acupuncture.
In addition to the correlation with race,the acceptance of acupuncture educational also related to the education level.Those with lower education level are more likely to mention some obstacles,such as worries about experiments,the existence of placebo and lack of interest in acupuncture[37].To some extent,these factors may reflect a lack of understanding of clinical trials and/or acupuncture therapy[5].Such studies are essential for a better understanding of the potential role of acupuncture in the management of cancer pain,as such differences have a significant impact on ethnic minorities and less educated people.Acupuncture may be able to solve the difference of symptom management in cancer treatment [25,38].
Our study also showed that higher acupuncture expectations,social norms,and overall health belief scores were significantly associated with the likelihood of a greater propensity to use acupuncture to treat pain.This finding suggests potential health differences between nonwhite and less educated people.Specific promotion and education may be needed,and efforts should be made to reduce structural barriers such as cost and insurance coverage,so that acupuncture can become a fair choice for pain management for survivors from different backgrounds.Understandably,if perceived barriers such as cost are reduced,the preference for acupuncture treatment will increase.If a certain amount of free acupuncture treatment is provided to patients,the demand for acupuncture and moxibustion may increase greatly,just like other auxiliary services such as nutrition and general consultation.
One study [39]conducted a systematic review and metaanalysis to evaluate the effects of acupuncture on malignancy-related,chemotherapy (CT)- or radiation therapy (RT)-induced,surgery-induced,and hormone therapy (HT)-induced pain.The analysis indicated that acupuncture significantly reduced cancer-related pain,with a small-size effect of -0.45 (95% CI -0.63 to -0.26);Subgroup analysis showed there was no sufficient evidence to support the beneficial effects of acupuncture for CT- or RT-induced and HT-induced pain.The study suggested that in future studies researchers should define the types of cancer pain (e.g.,malignancy-related pain).Another study[40]found an association between pain reduction and acupuncture (MD = -1.38; 95% CI -2.13 to -0.64;I2=81%); In the sensitivity analysis of pain types,pain was rated as moderate to severe and was significantly heterogeneous (MD = -1.61; 95% CI -2.89 to -0.34;I2=85%).
Though some studies had proved acupuncture is a recognized analgesic therapy,however,it still not been fully accepted in the public health care of oncology.According to a previous study of 1,135 Norwegian doctors,20% of them suggested that acupuncture should not be included in the public health care system [41].Another study had shown that some patients rely on healthcare professionals to provide objective and reliable information about the effectiveness of acupuncture [21].Our findings on patient preferences may lead to acupuncture as a more mainstream choice for pain relief,especially in patients who have higher expectations for acupuncture.Therefore,further controlled studies were welcomed on the treatment relationship between patients and clinicians,including treatment expectations.Meanwhile,professionals were suggested to know the latest scientific information to provide evidence-based advice for cancer patients.As more and more evidence showed the application of acupuncture in oncology,it is crucial to disseminate this knowledge to patients and providers,as there is a correlation between the extent to which patients are informed and their use of acupuncture [19].With this information,patients and doctors can make informed decisions to incorporate acupuncture into treatment to control the symptoms.
This systematic review has the following limitations:First,the included studies only conducted in United States and Sweden,which reflected the willingness of acupuncture treatment for cancer pain patients living in high-income countries.Therefore,we cannot generalize these findings to other populations.Second,due to the included studies combine the mild,moderate,and severe patients in different ways,we could not analyze the clear improvement of patients with different cancer pain levels.
CONCLUSION
This systematic review showed out of consideration of the safety and effectiveness of acupuncture treatment,as well as reasonable treatment prices,most cancer pain patients are interested in trying to reduce cancer pain through acupuncture treatment and with a high satisfaction to continue using.There were an obviously differences among patients of different races,ages,and education levels.Patients are an important part of the treatment process,and attitudes and preferences for treatment desperately needed for more research in the future.
ACKNOWLEDGMENT
This work was supported by the Fundamental Research Funds for the Central Universities (Grant no.18LZUJBWZ X006 and Grant no.2019jbkyzy002):Evidence-based Social Science Research.
The authors are all grateful to Cuncun Lu (Institute of Basic Research in Clinical Medicine,China Academy of Chinese Medical Sciences) for his methodological assistance.
- Cancer Advances的其它文章
- Efficacy and prognosis of mastoscopic axillary lymph node dissection for breast cancer:a systematic evaluation and meta-analysis
- How cancer stem cells cause disease recurrence in recovered patients
- How Can We Give Hope for Cancer Patients to Cure This Disease?
- Common mechanisms in chronic obstructive pulmonary disease and lung cancer