
Analysis of cancer incidence and mortality in Heilongjiang cancer registries,2016
2020-07-14 05:49:46HuiXinSunMaoXiangZhangWanYingWangHaiHanJiaBingBingSong
Cancer Advances 2020年4期
Hui-Xin Sun ,Mao-Xiang Zhang ,Wan-Ying Wang,Hai-Han Jia,Bing-Bing Song *
1Institute of Cancer Prevention and Treatment,Harbin Medical University,Harbin 150081,China;2Heilongjiang Academy of Medical Science,Harbin 150081,China;3Heilongjiang Cancer Center,Harbin 150081,China.
Abstract
Key words:Tumor registry,Incidence,Mortality,Heilongjiang
Background
In September 2019,National Health Commission and other 10 departments jointly issued the implementation plan of Health China action:cancer prevention and control (2019–2022) [1].Heilongjiang Province actively implemented comprehensive prevention and control measures following the requirements of the plan,such as steadily promoted system construction,tumor registration,early diagnosis and treatment,standardized diagnosis and treatment,scientific and technological innovation and other critical areas,and achieved initial results in prevention and control [2].However,the current cancer prevention system and serviceability in our province are still confusing to meet the demand of people’s growing health.Moreover,cancer prevention and treatment of insufficient imbalance problem are still outstanding,cancer prevention and control of form are still grim,to understand the current situation of incidence and mortality in our province.Now finishing tumor incidence and mortality data in Heilongjiang Province in 2016,through the review and the evaluation results,select quality qualified registry data analysis,now report as follows.
Materials and methods
Data sources
Twelve registries in Heilongjiang Province reported the data of cancer incidence,mortality and the corresponding population database.The reporting time of the database was from January 1,2016 to December 31,2016 for the first time confirmed new malignant tumors (ICD10:C00.0–C97,D45–D47) and benign tumors of the central nervous system (ICD10:D32.0–D33.9).Death cases were malignant tumor deaths in cancer registration (CR) areas during the same period.
Quality evaluation
According to theGuidelines for Cancer Registration in China(2016) [3],and referring toCancer Incidence in Five ContinentsVolume IX and the requirements for registration quality of the International Cancer Research Center/International Association for Cancer Registration [4–5],SAS9.4 statistical software was used to examine and evaluate the data.The integrity,validity and timeliness of the data were assessed by the main indicators such as percentage of morphologically verified cases (MV%),percentage of death certificate only (DCO%) and mortality to incidence ratio (M/I).
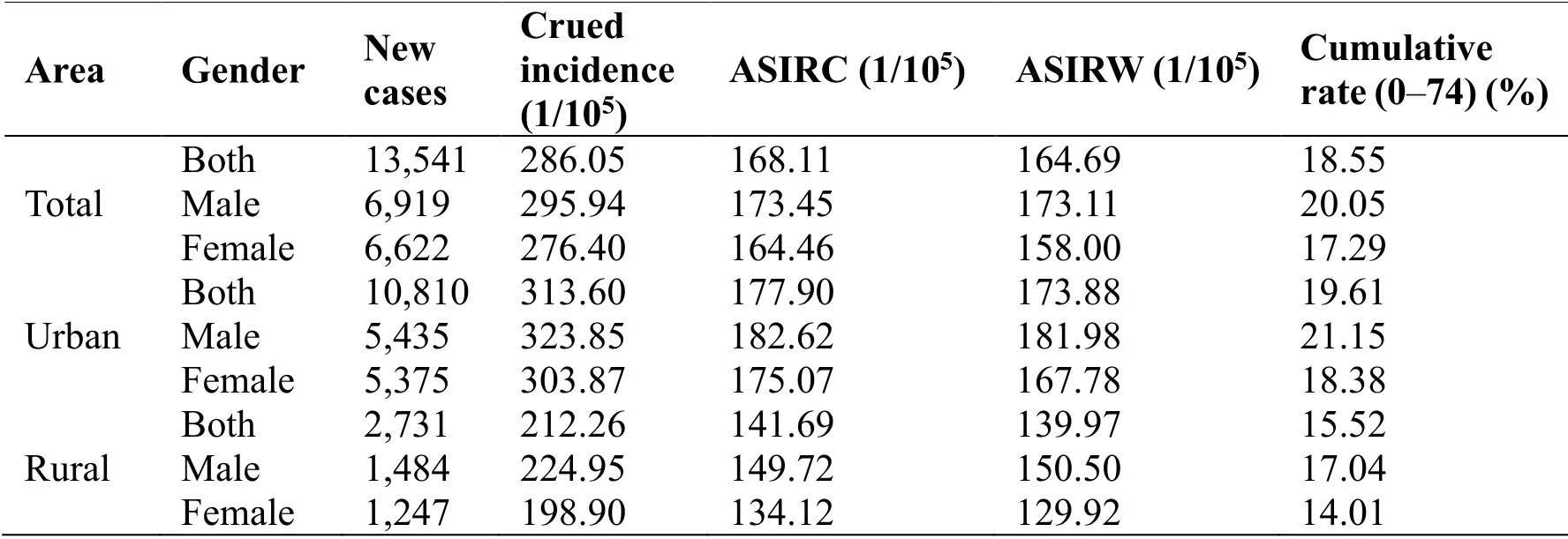
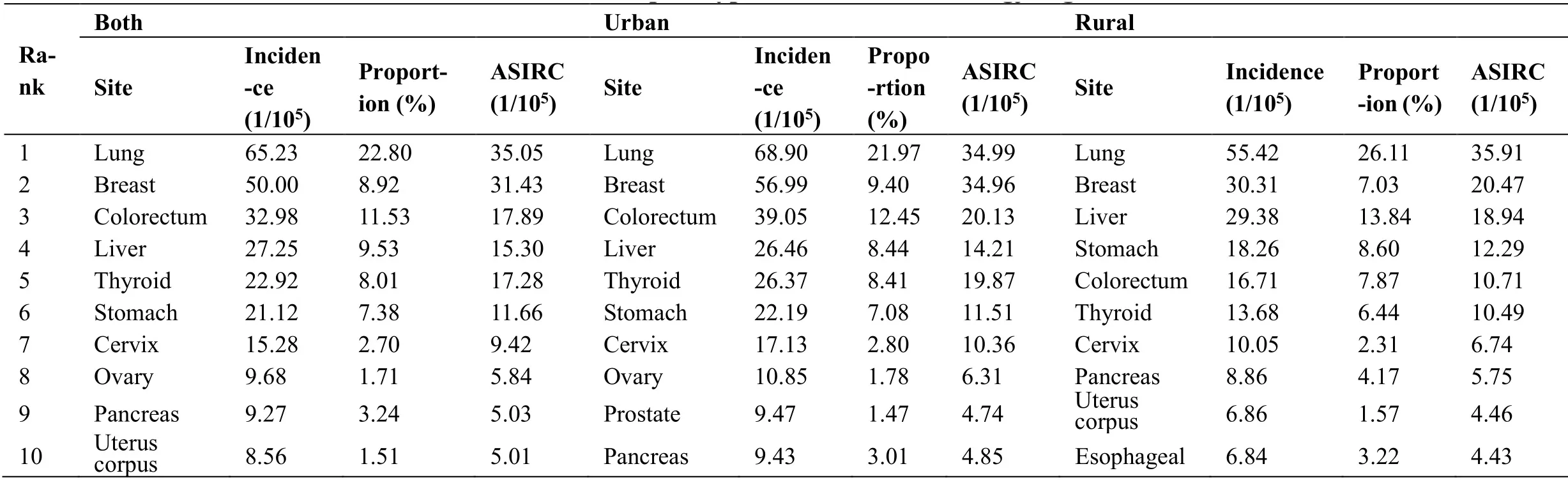
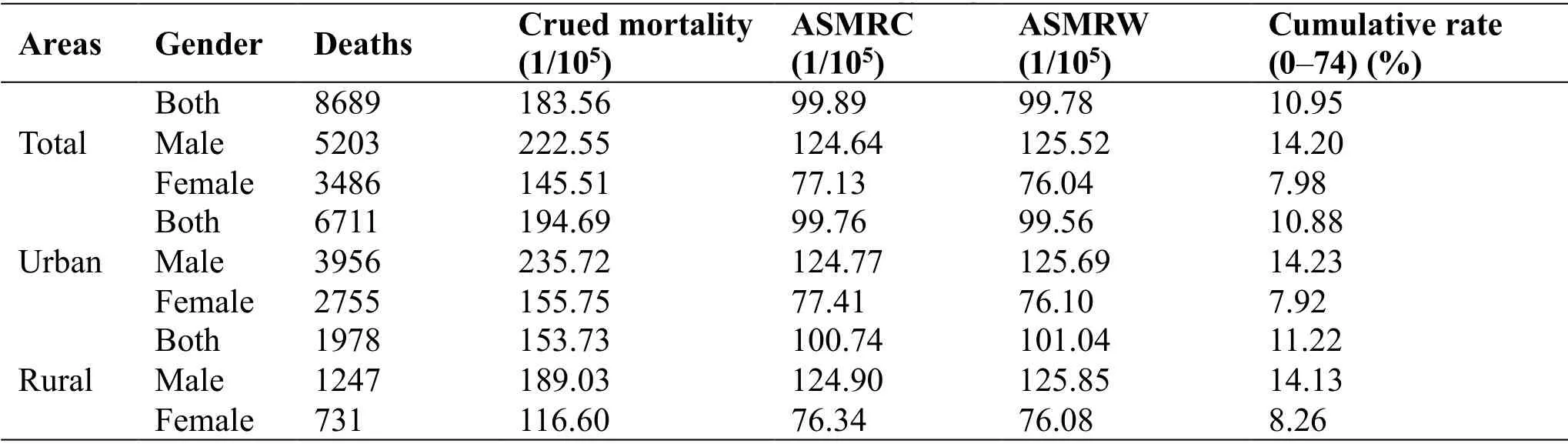
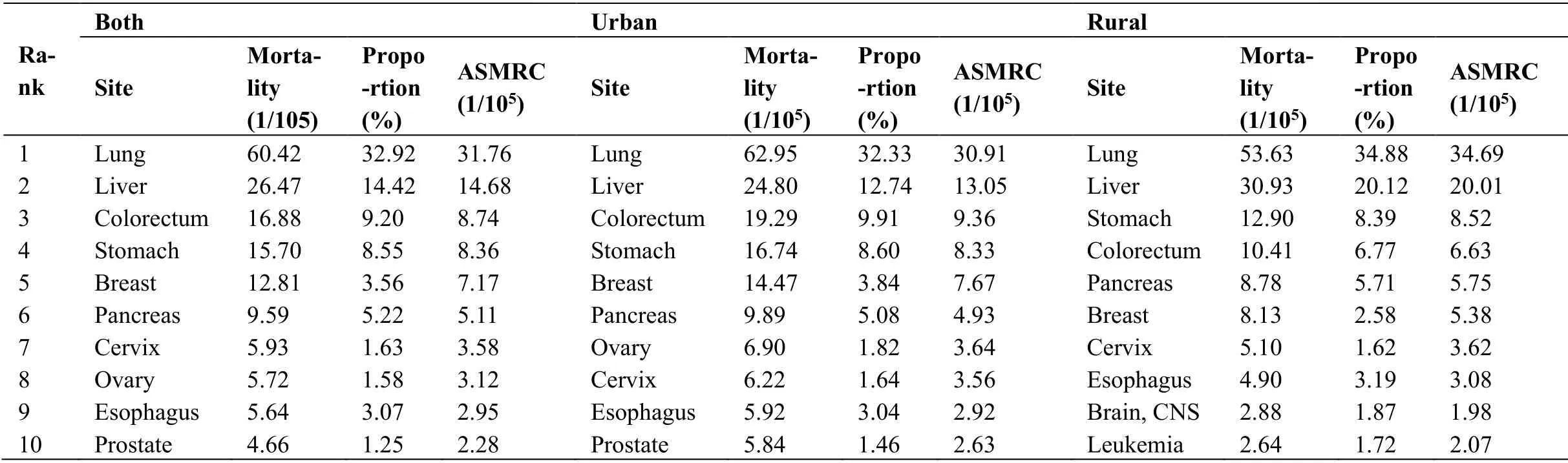
The quality evaluation criteria of CR data received by the National Cancer Center in China are 55% Crude incidence and mortality,sex and age-specific incidences and mortalities,age-standardized rates,cumulative rates,and truncated rates were analyzed.The top 10 malignant tumors in incidence and mortality were described emphatically.The Segi’s world population and the China 2000 population census data were used as the population standards. In 2016,the crude incidence of malignant tumors was 286.05/100,000 (295.94/100,000 males and 276.40/100,000 females),age-standardized incidence rates by the standard Chinese population (ASIRC) and by standard world population (ASIRW) were 168.11/100,000 and 164.69/100,000 respectively,and the cumulative rate (0–74 years old) was 18.55%. The crude incidence of malignant tumors in urban CR areas was 313.60/100,000 (323.85/100,000 males and 303.87/100,000 females),ASIRC and ASIRW were 177.90/100,000 and 173.88/100,000,respectively,and the cumulative rate (0–74 years old) was 19.61%.The crude incidence of malignant tumors in rural CR areas was 212.26/100,000 (224.95/100,000 males and 198.90/100,000 females).ASIRC and ASIRW were 141.69/100,000 and 139.97/100,000,respectively,and the cumulative rate (0–74 years old) was 15.52%.Compared with rural areas,the total incidence of males and females in urban areas is higher than that in rural areas (Table 1). In 2016,the incidence of malignant tumors in the Heilongjiang CR area increased slowly before 25 years old and rapidly after 25 years old.In the age group of 25–50 years old,the incidence of malignant tumors in females was higher than that in males.After 55 years old,the incidence of malignant tumors in males was higher than that in females.In urban areas,the incidence rate of male and female in the age group of 0–20 years is rising slowly alternately;in the age group of 25–50 years,the incidence rate of the female is higher than that of the male;after the age of 55 years,the incidence rate of male is higher than that of the female.In rural areas,the incidence rate of females is higher than that of males in the age group of 15–50 years old.After 55 years old,the incidence rate of males is higher than that of females (Figure 1). In 2016,lung cancer had the highest overall incidence in tumor registries areas in Heilongjiang Province,with a crude rate of 65.23/100,000,accounting for 22.81% of all new malignant tumor cases.It was followed by breast cancer,colorectal cancer,liver cancer,thyroid cancer,stomach cancer,cervical cancer,ovarian cancer,pancreatic cancer and corpus uteri cancer.Lung cancer has the highest incidence in urban areas,with a crude extent of 68.90/100,000,accounting for 21.97% of all new malignant tumor cases.It was followed by breast cancer,colorectal cancer,liver cancer,thyroid cancer,stomach cancer,cervical cancer,ovarian cancer,prostate cancer and pancreatic cancer.Lung cancer was the most common cancer in rural areas,with a crude incidence of 55.42/100,000,accounting for 26.11% of all new malignant tumor cases.Next were breast cancer,liver cancer,stomach cancer,colorectal cancer,thyroid cancer,cervical cancer,pancreatic cancer,corpus uteri cancer,and esophageal cancer (Table 2). In 2016,the crude mortality rate of malignant tumors in the Heilongjiang CR area was 183.56/100,000,agestandardized mortality rates by standard Chinese population (ASMRC) and age-standardized mortality ratesd by standard world population (ASMRW) were 99.89/100,000 and 99.78 /100,000,respectively,and the cumulative rate (0–74 years old) was 10.95%.The crude mortality rate of malignant tumors in urban areas was 194.69/100,000,ASMRC and ASMRW were 99.76/100,000 and 99.56/100,000,respectively,the cumulative rate (0–74 years old) was 10.88%.In rural areas,the crude mortality rate of malignant tumors was 153.73/100,000,ASMRC and ASMRW were 100.74/100,000 and 101.04/100,000,respectively,and the cumulative rate (0–74 years old) was 11.22% (Table 3). In 2016,the mortality of malignant tumors in the tumor registration area of Heilongjiang Province increased slowly before the age of 35,and rapidly after the age of 35,males have a higher mortality rate after age 30 than females.After the age of 40 in urban areas,the incidence rate of males is higher than that of females.After the age of 30 in rural areas,the incidence rate of males is higher than that of females (Figure 2). Lung cancer ranked first among the malignant tumor death orders in the tumor registration areas of Heilongjiang Province.Lung cancer with a crude mortality rate of 60.42/100,000,accounting for 32.92% of all malignant tumor death cases,followed by liver cancer,colorectal cancer,stomach cancer,breast cancer,pancreatic cancer,cervical cancer,ovarian cancer,esophagus cancer and prostate cancer.Lung cancer also ranks first in the death order of malignant tumors in urban areas,with a crude mortality rate of 62.95/100,000.The mortality rate was followed by liver cancer,colorectal cancer,gastric cancer,breast cancer,pancreatic cancer,ovarian cancer,cervical cancer,esophageal cancer and prostate cancer.Lung cancer was the leading cause of cancer mortality in rural areas,with a crude mortality rate of 53.63/100,000.It was followed by liver cancer,gastric cancer,colorectal cancer,pancreatic cancer,breast cancer,cervical cancer,esophageal cancer,brain cancer and leukemia (Table 4). Table1 Incidence of malignant tumors in Heilongjiang Province,2016 The health China action:cancer prevention and control implementation plan (2019–2022) pointed out that the tumor registration and reporting system should be improved.All districts and counties should be covered by 2022,and annual tumor registration reports should be issued at the provincial level.Heilongjiang Province achieved the full coverage of tumor registration districts and counties in 2020,and released the 2018 annual report of tumor registration in Heilongjiang Province at the beginning of 2020 [6].Besides,Heilongjiang Province used the national CR information platform system to report tumor incidence and death data,which improved the reporting efficiency and quality,and promoted the application research of big cancer data [7].Timely understanding of cancer incidence trends in our province can not only carry out targeted prevention and control work,but also provide a theoretical basis for cancer prevention and control.The population covered by the 10 cancer registries included in this study accounts for 12.5% of the total population of the province,and the results can reflect the latest cancer epidemic situation in Heilongjiang Province to a certain extent. In 2016,the incidence of malignant tumors in the tumor registration areas of Heilongjiang Province was 286.05/100,000,which was the same as the national average incidence level in 2015 (285.83/100,000) [8].Compared with the 2015 data in this province (incidence of 259.90/100,000) [9],the incidence rate has increased.Compared with 2015,colorectal cancer and pancreatic cancer increased by 1 position,liver cancer and uterus corpus cancer decreased by 1 position,and other cancers did not change.The incidence of cancer in urban areas was higher than that in rural areas,and there was a big difference in the rank of cancer species between urban and rural areas.In 2016,the mortality rate of malignant tumors in the tumor registration areas of Heilongjiang Province was 183.56/100,000,higher than the national average death level in 2015 (the mortality rate was 170.05/100,000) and the provincial death rate in 2015 (the mortality rate was 164.69/100,000).The crude mortality rate in urban areas is much higher than that in rural areas.Compared with 2015,colorectal cancer increased by 1 position,gastric cancer decreased by 1 position,and cervical cancer increased by 2 positions.Esophageal cancer decreased by 2 positions. The incidence and mortality of lung cancer ranked first in our province,air pollution and occupational exposure are also related to the occurrence of lung cancer.The development of industrialization has led to increased air pollution in recent years,and longterm exposure to such an environment has significantly increased the risk of lung cancer.The study shows that for every 10 μg/m3increase of PM2.5 in the surrounding environment,the risk of lung cancer increases 1.43 times [10–11].Since the implementation of the Framework Convention on Tobacco Control in China in 2006,tobacco control policies have been introduced in various regions.Through legislation and measures such as raising tobacco tax rates,China’s public smoking rates drop dramatically.However,the 2015 China Adult Tobacco Survey Report issued by the China Center for Disease Control and Prevention points out that China’s tobacco consumption is prevalent and people still need to improve the awareness of the dangers of tobacco.Breast cancer is associated with postmenopausal hormone use,alcohol consumption and obesity,and breast-feeding and appropriate physical activity are protective factors against breast cancer [12]. Helicobacter pylori(HP) is a significant risk factor for gastric cancer.HP cause almost 90% of new cases of non-cardia gastric cancer.Although the prevalence of HP has a reasonable correlation with the incidence rate of gastric cancer,in addition to HP,salt-cured foods,low fruit intake,alcohol consumption and smoking were also identified risk factors for gastric cancer [13].World Cancer Research Fund/American Institute for Cancer Research pointed out that salt and salted food may be the cause of gastric cancer. Table2 The incidences of top 10 types of cancer in Heilongjiang Province,2016 Table3 Cancer mortalities in Heilongjiang Province,2016 Table4 The mortality of top 10 types of cancer in Heilongjiang Province,2016 High concentration of salt can lead to hyperplasia of gastric epithelium and damage of parietal cells,increase HP colonization,and improve the ability of HP to change the function of epithelial cells [14].The main risk factors for liver cancer are chronic infection with hepatitis B virus (HBV) or hepatitis C virus (HCV),aflatoxin-contaminated food,heavy alcohol consumption,obesity,smoking and type 2 diabetes.In countries with high rates of liver cancer,the key determinants are chronic HBV infection and aflatoxin exposure.In contrast,in other countries (Japan,Egypt),HCV infection may be the primary cause.The increased prevalence of obesity is believed to be a contributing factor to the increased incidence of liver cancer in low-risk liver cancer areas [15].Since 1982,primary prevention of the majority of liver cancer cases has been possible through the HBV vaccine,which has significantly reduced the incidence of liver cancer with HBV infection.However,there is currently no vaccine to prevent HCV infection.Although there has been a substantial decline in the spread of HCV in resource-rich countries,however,continued use of contaminated needles and unsafe blood transfusions are still the routes of transmission of the HCV [16].The cause of thyroid cancer is unknown.The only established risk factor for thyroid cancer is ionizing radiation,especially in childhood.However,there is evidence that other factors (obesity,smoking,hormone exposure,and certain environmental pollutants) may also play a role.The incidence of thyroid cancer has been increasing in many countries since the early 1980s,but the mortality rate has remained fairly stable.An increasing incidence of thyroid cancer is believed to be caused by overdiagnosis,especially after the introduction of new diagnostic techniques [17]. The burden of cancer in our province is still heavy,so we can take a three-level prevention model of cancer with community hospitals as the starting point,promote the prevention of causes,reduce the damage of external adverse factors.Also,it is recommended that high-risk groups conduct early cancer screening to achieve the purpose of early detection,early diagnosis and early treatment,so as to move forward the prevention and treatment.More funds will be spent on basic public health services,and suggest a comprehensive public health service system to prevent and control incidence rate and mortality.Statistical analysis
Results
The incidence of malignant tumors
Age-specific morbidity
Incidence of major cancers
Mortality of malignant tumors
Age-specific mortality
Mortality of malignant tumors
Discussion
- Cancer Advances的其它文章
- Anti-cancer drugs targeting using nanocarrier niosomes-a review
- Clinical Research progress of traditional Chinese medicine in treating esophageal cancer
- Thick tongue coating:diagnostic markers for metastatic colorectal cancer?
- Pretreatment levels of circulating endothelial cells on efficacy of first-line therapy in patients with advanced non-small cell lung cancer