
Lumbar interspinous pressure pain threshold values for healthy young men and women and the effect of prolonged fully flexed lumbar sitting posture: An observational study
2020-03-27 04:08:56MartinPeterssonAllanAbbott
World Journal of Orthopedics 2020年3期
Martin Petersson, Allan Abbott
Martin Petersson, Department of Physiotherapy Gripen, V?rmland Country Council, Karlstad SE-65224, Sweden
Martin Petersson, Allan Abbott, Department of Medical and Health Sciences, Division of Physiotherapy, Faculty of Health Sciences, Link?ping University, Link?ping SE-58183,Sweden
Abstract
Key words: Low back pain; Pain pressure threshold; Algometer; Posture; Spine; Pain mechanism
INTRODUCTION
Low back pain (LBP) is a common condition with large burden worldwide[1].Exposure to prolonged sitting with a flexed lumbar posture has been suggested in the literature to be a potential risk factor for self-reported LBP but strong evidence is lacking regarding if occupational sitting is an independent causal factor[2-5]. Several studies have investigated possible mechanisms of how prolonged flexed postures may influence the onset of LBP and discomfort. Flexed lumbar posture tensions posterior segmental structures such as the interspinous ligaments of the lumbar spine,which contribute to the prevention of lumbar hyperflexion[6]. Prolonged tensioning of posterior segmental structures causes viscoelastic deformation of trunk soft tissues,reductions in intrinsic trunk stiffness and alters the active neuromuscular behavior[7-11].This may in theory produce nociception and peripheral sensitization of these structures leading to reduced thresholds for nociception[12,13]. Furthermore, in the event of prolonged nociception or maladaptive psychosocial factors negatively affecting the pain experience, a decreased functioning of descending nociception inhibiting pathways may contribute to a central nervous system sensitization[13]. This may further reduce nociceptive pain thresholds or lead to the persistence of pain without nociceptive stimulus[14].
Biochemical processes may even be influenced by prolonged tissue loading providing a pathway for tissue sensitivity and inflammation[15]. Staudet al[16]displayed that healthy individuals who have been repeatedly provoked by tissue stress can experience increased sensitivity and the persistence of the pain[16].
Research has shown that individuals with lumbar pain have lower pain thresholds than healthy individuals[17-20]. In these studies, pain thresholds in the lumbar spine are commonly measured using a pressure gauge indicating kilopascals per second(kPa/s) of increasing pressure application until pain is perceived by the subject[17-22].
Only one study, Imamuraet al[19], has investigated the interspinous pressure pain thresholds between the L1-L5 lumbar spinous processes. Gender differences have been observed in pressure pain thresholds[23,24], but no study has investigated possible gender difference regarding interspinous pressure pain thresholds. No study has previously investigated whether exposure to prolonged flexed sitting posture affects interspinous pressure pain thresholds for healthy young men and women without back pain, despite this being a suggested risk factor for LBP[2-4]. The purpose in this study is to investigate whether exposure to prolonged fully flexed lumbar sitting posture provokes discomfort and lowers interspinous pressure pain thresholds in the lumbar spine for healthy young men and women without previous lumbar pain. The hypothesis is that there is a significant decrease in interspinous pressure pain thresholds after exposure to prolonged fully flexed lumbar sitting posture provoking discomfort and that there is a significant difference between men and women.
MATERIALS AND METHODS
Research design
This is an observational study of pressure pain thresholds before and after exposure to discomfort from prolonged fully flexed lumbar sitting in health men and women.Therefore, cases are their own controls in a before and after exposure design.According to Swedish law (2003: 460) on the ethics of human research, it is described that all research performed and dealing with sensitive personal data should be ethically tested. Section 2 of this law states that regional ethical committee assessment is required for “Scientific experimental or theoretical work to acquire new knowledge or scientific quality improvement work, but not such work done in the framework of first or second cycle education[25]. Therefore, because this study was conducted as a part of a master's thesis, ethical approval was provided after assessment performed according to the Helsinki declaration by the ethics board of second cycle education at Linkoping University.
Participants
The recruitment of potential participants occurred between the dates of January 2017 to Mars 2017 through informing a convenience sample of students at Linkoping University, Sweden, about the study. Inclusion criteria for participation were healthy individuals without current or previous lumbar pain, aged between 20 to 35 years.Exclusion criteria included diagnosed medical conditions, current or previous lumbar pain, pregnancy, tolerance of ≥ 1000 kPA algometer lumbar interspinous pressure without provoking pain during the initial measurements. A a-priori sample size calculation was performed using GPower 3.1. This was based on the probability of detecting a significant difference (P= 0.05) between the pre and post pain pressure threshold measurement with 80% statistical power and a hypothesised effect size ofr= 0.5. The result of the calculation indicated that 26 participants were required. In order for the sample to be as representative as possible, 13 men and 13 women were recruited.
Measurements
The algometer used for the measurements was of the SOMEDIC Electronics brand(Solna, Sweden) (Figure 1).
In a study by Walleret al[26], intra- and inter-examiner reliability was examined regarding algometry on healthy young people, including the testing of locations such as the lumbar spine. The measurement method was found to have both good intraexaminer reliability (ICC = 0.94-0.99) and inter-examiner reliability (ICC = 0.90-0.98)[26]. Other studies also show good reliability[27,28].
Before each measurement, a quality control of the instrument was performed through calibration, to ensure it was functioning. This study used a 1 cm2 round rubber sheet ending on the algometer applying a pressure velocity of 50 kPA / s, like other studies such as Walleret al[26]. Measurement of pain thresholds was performed between the spinous processes from L1 to L5 (L1-L2, L2-L3, L3-L4 and L4-L5). These were identified through valid palpation methods using multiple bony landmarks[29,30].The measurement was thus performed on four points with three measurements at each point to calculate an average, resulting in 12 pressure final measures. Between each measurement time, a 10 s pause in testing occurred consistent with test protocols from previous studies[18,24,26,31]. The participants were tested in a prone position on a plinth where the interspinous areas between spinal processes from L1 to L5 were marked with a felt pen to ensure that the repeated application of the pressure was at the correct point. During the measurement, participants communicated verbally, by the word "stop", when the first sense of pain was detected. The pressure was then stopped. After the baseline algometry measures, the participants changed directly to a seated position, without rest, on a chair in a full flexed lumbar position (Figure 2).
Specific instructions guidance to the participants: Sit with 90 degrees flexion of the knee joint and ankle joint, while maintaining the lumbar spine in full flexion with posterior pelvic tilt[32-35]. Participants were also instructed to rest their upper body weight on the forearms in the slumped position to emphasis a passive fully flexed lumbar positioning rather than erector spinae activity. The author ensured the test position was consistent for all participants.

Figure 1 Algometer.
Participants were asked not to change position during the test. The participants either sat for a maximum of 15 min or until they experienced a 7/10 rating of discomfort (0 = no pain/discomfort - 10 = maximum pain/discomfort) in the lumbar spine according to Borg CR10[36]. The scale can be used for measuring different sensory sensations and experiences including pain and discomfort with good validity and reliability[36]. The time of 15 min for the test was determined on the basis of Solomonowet al[7], which found that 15 min in maximum flexed lumbar posture causes high strain on the supraspinal ligaments. Immediately after the test, a similar measurement procedure was performed as during the first measurement to determine whether there were differences between pressure pain thresholds before and after the prolonged lumbar flexion experiment.
Data analysis
The collected data was manually entered into IBM SPSS version 23 program, where all analytical calculation was performed. Non-parametric statistics have been used because none of the measurement variable data distributions fulfilled the assumptions of normality. Descriptive statistics are reported as median and interquartile range(IQR). To compare the measurements between pre-test and post-test differences within the group, a Wilcoxon signed ranks test has been performed. The test has been conducted to see if there was any significant difference between the pain threshold before and after prolonged fully flexed lumbar sitting posture in healthy individuals.To detect a possible difference between the sexes, a Mann-WhitneyUtest was used.Statistical significance was set at theP< 0.05 level. Rosenthal[37], proposes an alternative effect size measure when the general assumptions of Cohen'sdformula are violated. In this case, effect sizeris proposed for pre-test to post-test change in pressure pain thresholds, calculated by dividing the Z-standardised test statistic by the square root of the number of observations over the 2 time points (2 × 26 observations). Effect sizer= 0.10 is considered a small effect,r= 0.30 is a medium effect andr> 0.50 is a large effect size[37].
RESULTS
All 26 participants (13 men and 13 women) completed the study. The median age for the entire study population was 24.0 years (IQR = 3). By comparison, median age for women was 23 (IQR = 8) years and 24 (IQR = 3) years for men. There was a significant difference (P= 0.01) of age between the sexes. As a result of the fully flexed lumbar spine sitting posture, all participants experienced temporary discomfort in the lower back but the proportion with discomfort of 7/10 was 62%. Of those completing the full 15 min exposure (38%) without reaching up to 7/10 discomfort in the lower back,there was an even gender distribution. The median time for the seated flexion test was 12 min (IQR = 3). The median time for women was 11.5 min (IQR = 3s) and 12.5 min(IQR = 3) for men showing no statistically significant difference (P> 0.05).
The statistical analysis displayed that for all points tested, there was a significant difference between pre-test and post-test, with lower pressure pain thresholds posttest. The result demonstrated that exposure to prolonged static sitting in a fully flexed lumbar posture decreases pressure pain threshold of interspinous lumbar spine structures. Measurement points in the lumbar spine together had a pre-test pain threshold value of 359 kPa and post-test value of 312 kPa. Regarding pre-test and post-test effect size difference in pressure pain threshold, the result showed a larger=-0.56 total change for all points in the lumbar spine. (Table 1).

Figure 2 Seated position during the test.
The calculation of pre-test and post-test measurements for women also showed a significant difference with moderate effect size lowering of post-test pressure pain thresholds for all points. The pre-test pressure pain thresholds together for all points were 331 kPa and post-test 269 kPa in the lumbar spine (Table 2). The analysis performed for men also showed a significant difference with moderate effect size lowering of post-test pressure pain thresholds for all points except for L4-L5 (P=0.069). The pre-test pressure pain thresholds together for all points in the lumbar spine showed a measure of 366 kPa and post-test 322 kPa (Table 3).
There were no statistically significant differences between men and women for pressure pain thresholds measured at pre-test or post-test and with regards to change from pre-test to post-test (Table 4).
DISCUSSION
The results of the study show that interspinous pressure pain thresholds after exposure to prolonged fully flexed lumbar sitting posture (maximum of 15 min) were significantly lowered with moderate - large effect sizes in young men and women which supports our first hypothesis. These results add new objective knowledge regarding gender-based reference values for interspinous pressure pain threshold for healthy subjects and new knowledge that prolonged flexed lumbar posture increases interspinous tissue pain sensitivity. This could be a potential mechanism among other factors reported in previous literature suggesting that flexed lumbar posture may increase the risk of self-reported lumbar pain[2-4]. However, according to O'Neillet al[20]it is likely that lowered pressure pain threshold is associated with but does not constitute an independent risk factor for the development of persistent lumbar pain.
Previous research has shown that a tissue load applied for a longer period of time may trigger cytokines associated with nociceptor activation[13,38]. That can be considered as a potential physiological mechanism leading to lumbar pain experienced after prolonged fully flexed lumbar sitting posture. Previous research suggests a relationship between longer time periods of static sitting and pain in the lumbar spine[2,40]. Bakkeret al[3], suggests that intensive use of the lumbar spine in flexion has a strong connection to the development of lumbar pain. Therefore, in relation to the results of our current study, it is possible that both longer periods of static sitting as well as flexed lumbar posture are possible mechanisms of sensitization of lumbar spine structures. To compare importance of these potential mechanisms,future experimental trials should investigate variation of flexion in various degrees during long periods static sitting.
In previous studies, the pressure pain threshold for paraspinal and erector spinae muscles 2 cm lateral from spinous processes for young people without low back pain ranges between 536-910 kPa[18,23,24,26]. Furthermore, the normal values reported for spinous processes range between 316-450 kPa[23,26]and for interspinous areas 759 kPa[19]. Our findings however show lower interspinous pressure pain thresholds than Giesbrechtet al[18]in young people without low back pain and are more similar with previous reported thresholds for spinous processes[23,26]. The measurement process in our study was performed on four points in the lumbar spine and the choice of using the mean of 3 tests is based on previous reliability studies showing intra-raterreliability[27]. One may consider a potential limitation of repeated pain pressure threshold testing being that it may cause tissue sensitization, which may in turn decrease pain pressure thresholds. However, previous studies using up to 3 measurements at the same point to determine pain pressure threshold on lumbar spine structures as well as similar spatial distances between adjacent points and the time between repeated measurement (at least 10 min) have been shown to prevented spatial and temporal summation[20,41].
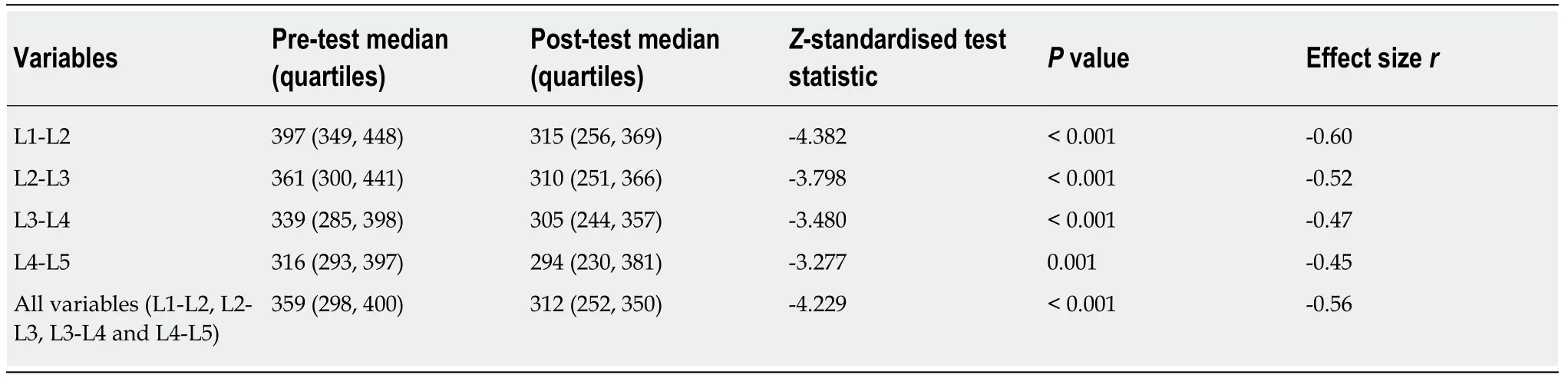
Table 1 The median value and quartiles, Wilcoxon signed rank test and effect size r for the whole study population regarding interspinous pressure pain thresholds before (pre-test) and after (post-test) exposure to prolonged flexed lumbar sitting posture
The result of the average duration to provoke discomfort in the low back of 7/10 was 12 min for exposure to the fully flexed lumbar spine sitting posture. It shows that the maximum 15 min may be considered an adequate limit of fully flexed lumbar sitting posture for the majority of health young adults. However, a potential limitation in our study is that 38 percent of the participants did reach 15 min in a fully flexed lumbar sitting posture without experiencing discomfort in the low back up to 7/10. Despite this, significant decreases in lumbar pain pressure thresholds were observed. If the maximum test time would have been set to 20 min, the average time to low back discomfort of 7/10 would however probably increase but probably not to a large extent.
The analysis of gender difference in pain pressure thresholds before and after prolonged fully flexed lumbar sitting posture showed that there were no significant differences. Hence, our secondary hypothesis that there is a significant difference between women and men regarding thresholds in the lumbar spine cannot be verified. These results are consistent with Farasyn and Lassat[24], who also concluded that there were no gender differences regarding pressure pain thresholds for lumbar spine erector spinae muscles. On the contrary, in a study by Binderupet al[23], a significant difference was found regarding the gender difference in pain pressure thresholds for erector spinae muscles and spinous processes in the lumbar spine.Their results showed that men had higher thresholds (506 kPa) than women (428 kPa),whereas our study on a similar sample showed a smaller gender difference (men =366 kPa, women = 331 kPa) without statistical significance. A limitation with our study was however that sample size was not specifically powered to minimize potential false negative results for gender subgrouping, but a trend was seen that healthy young adult men have higher lumbar thresholds than women. To investigate further, more studies with larger study populations are needed, which with good power can demonstrate and clarify whether there is really a gender difference or not.
There are several clinical implications of our research findings. For example, the Coin test is a pain provocation test for the interspinal ligaments[39]. The test has not been investigated in studies but nevertheless, the test is used in both teaching and clinical practice. As an algometer was applied in the lumbar interspinous areas in our study, the pain thresholds that were recorded can serve as a reference frame for physiotherapists who practice coin test in the lumbar spine examination of young adults. If the pressure activates early-stage pain indicating a low threshold, it may,along with other factors be a potential risk factor for a patient to have developed chronic lumbar pain[20]. The study′s results also support the inclusion of subjective assessment of postural sitting behaviors such as prolonged fully flexed lumbar sitting posture and the possible clinical utility as a physical test while conducting a patient interview. Future research could adapt the sustained lumbar flexion method as a novel experimental pain protocol for pain research.
In conclusion, the result showed that a fully flexed lumbar sitting posture for up to 15 min can provoke discomfort in the lower back in young health adults and significantly reduce lumbar interspinous pain pressure thresholds. The analysis does not show a significant gender difference for the pain thresholds before and after the test.
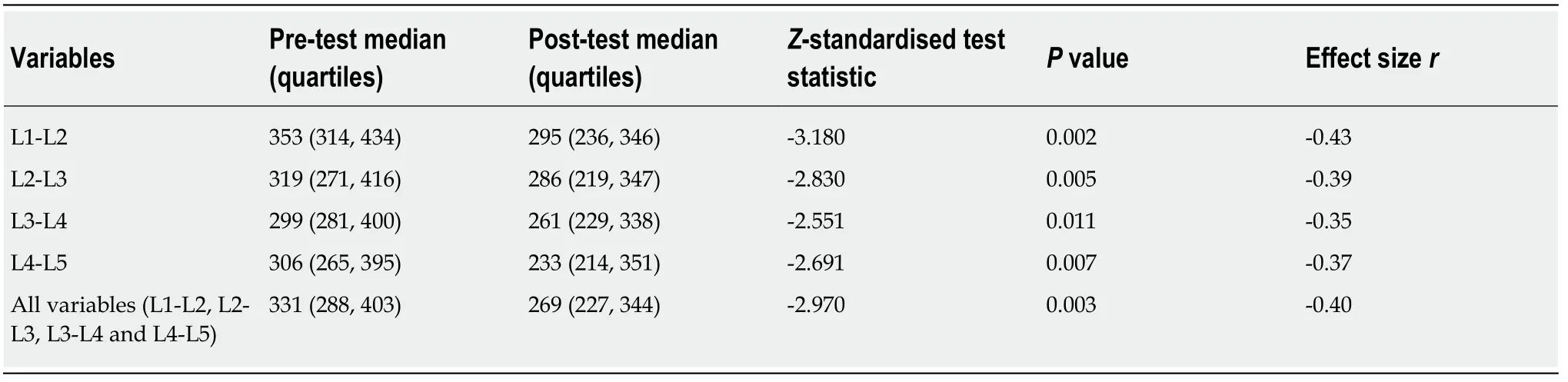
Table 2 The median value and quartiles, Wilcoxon signed rank test and effect size r for women regarding interspinous pressure pain thresholds before (pre-test) and after (post-test) exposure to prolonged flexed lumbar sitting posture
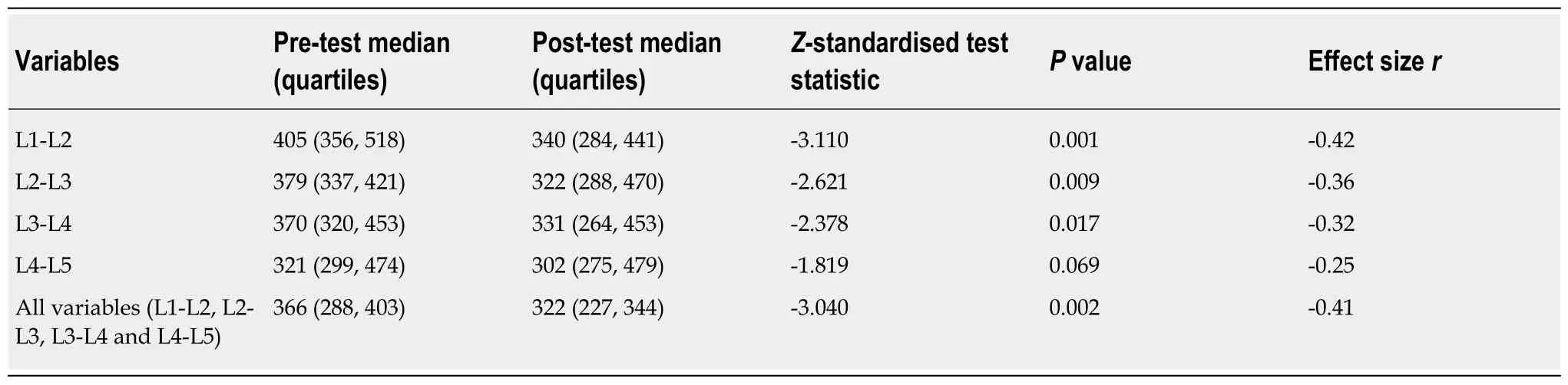
Table 3 The median value and quartiles, Wilcoxon signed rank test and effect size r for men regarding interspinous pressure pain thresholds before (pre-test) and after (post-test) exposure to prolonged flexed lumbar sitting posture
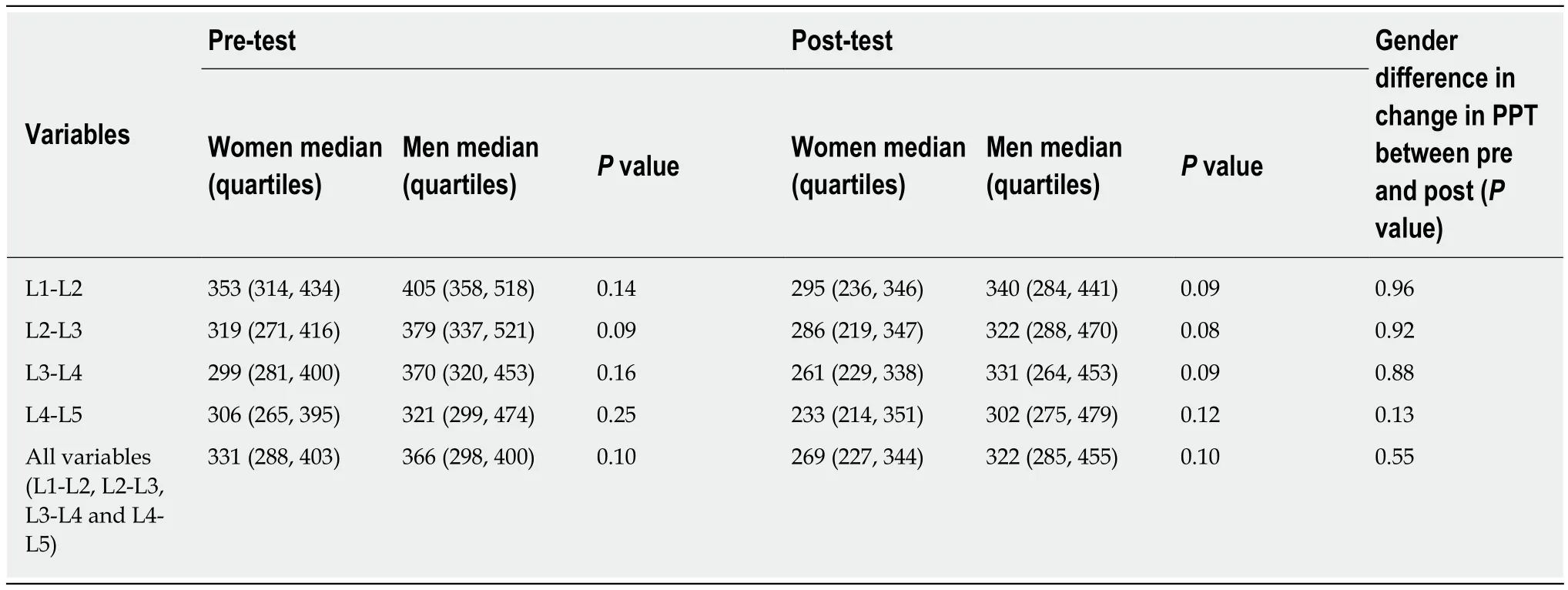
Table 4 The median value, quartiles and Mann-Whitney U test comparing men and women for pressure pain threshold measurement pre and post prolonged flexed lumbar sitting posture
ARTICLE HIGHLIGHTS
Research background
Exposure to prolonged sitting with a flexed lumbar posture has been suggested in previous literature to be a potential risk factor for self-reported Low back pain (LBP).
Research motivation
No study has previously investigated whether exposure to prolonged flexed sitting posture provokes discomfort in the low back and lowers interspinous pressure pain thresholds for healthy young men and women without previous back pain, despite this being a suggested risk factor for LBP.
Research objectives
To investigate whether sitting in a prolonged flexed lumbar posture provokes discomfort in the low back and lowers the interspinous pressure pain threshold in the lumbar spine for healthy young men and women without previous LBP.
Research methods
An observational study of lumbar interspinous algometry was conducted before and after 15 min of exposure to prolonged flexed sitting posture in 26 healthy participants (13 men, 13 women) between ages 20-35 years who have had no previous low back pain episodes.
Research results
Prolonged flexed sitting posture for up to 15 min provokes temporary discomfort in the lower back. There was a moderate-large decrease in lumbar interspinous pressure pain threshold after exposure for both men and women.
Research conclusions
Fully flexed lumbar sitting posture for up to 15 min provokes temporary discomfort in the lower back in most young health adults and significantly reduced lumbar interspinous pain pressure thresholds
Research perspectives
The study supports prolonged flexed lumbar posture as a potential mechanism provoking discomfort in the low back and lowering pain thresholds which may influence risk of future LBP episodes.
 World Journal of Orthopedics2020年3期
World Journal of Orthopedics2020年3期
- World Journal of Orthopedics的其它文章
- Atraumatic groin pain secondary to an aneurysmal bone cyst: A case report and literature review
- Systematic review of the etiology behind patellar clunk syndrome
- Analysis of electrocautery smoke released from the tissues frequently cut in orthopedic surgeries
- Observational study of a new modular femoral revision system
- Distraction arthroplasty in osteoarthritis of the foot and ankle