
Frailty and acute coronary syndrome: does gender matter?
2019-03-22 09:09:52LourdesVicentManuelMartnezSell
Journal of Geriatric Cardiology 2019年2期
Lourdes Vicent, Manuel Martínez-Sellés,2
1Servicio de Cardiología, Hospital General Universitario Gregorio Mara?ón, CIBERCV, Madrid, Spain
2Universidad Europea, Universidad Complutense, Madrid, Spain
Abstract There are important sex-related differences in elderly patients with acute coronary syndrome (ACS). Women are older, more frequently frail, and present more comorbidities than men. Atypical symptoms at presentation are also more common in female patients, they are leaded to a delayed diagnosis and treatment. Coronary angiography and subsequent revascularization are frequently underused in elderly women and they tend to receive less guidelines-recommended therapies. The prognosis in elderly frail women with ACS is poor, and it is with high mortality and readmissions rates. Bleeding is recurrent ischemic events in which it is more frequent in women than in men. Recovery time might be long, and a multidisciplinary approach is desirable to improve prognosis and quality of life. Further studies are needed in order to clarify the benefit of the different therapies in the group of frail women, and this is particularly true for revascularization, as scientific evidence in this group is very scarce.
Keywords: Acute coronary syndrome; Frailty; The elderly; Women
1 Introduction
Elderly patients represents near a third of the cases of acute coronary syndrome (ACS),[1]and most of them are women who frequently have a different clinical profile and a poorer prognosis than men.[2]Therefore, it is crucial to study the influence of sex on diagnosis, management, and outcome of patients with advanced age that suffer an ACS.
2 Sex and cardiovascular aging
Cardiovascular aging leads to an atherosclerosis phenomenon that it can be modulated by the presence of multiple genetic and environmental factors. Coronary artery disease occurs almost a decade earlier in men than in women.[3]Hormonal factors, lifestyle behavior, and differences in cardiovascular risk factors may partially explain this sex gap.[3,4]When coronary disease manifests, women are frequently elderly,[2,3]and they are with substantial comorbidities.[5]It has also been suggested that there could be a male-female health-survival paradox, as men have usually better health but mortality among men was highe, while women live longer but they are with more disabilities.[4]
2.1 Frailty, sex, and acute coronary syndromes
Frailty is a devastating condition what it will lead to increased vulnerability,[6]due to changes in three dimensions that are closely interrelated (Figure 1). Frailty is associated with a poor outcome and a high risk of dependence.[7,8]About a third of elderly patients with ACS has frailty,[9]near half of those ≥ 75 years are frail, and almost a quarter are severely frail.[8]Frailty is a dynamic state that it can be reversible,[7]but the prevalence of frailty in the elderly is about twice in women than in men.[7,10]Several differences could explain this sex-related disparity (Table 1).
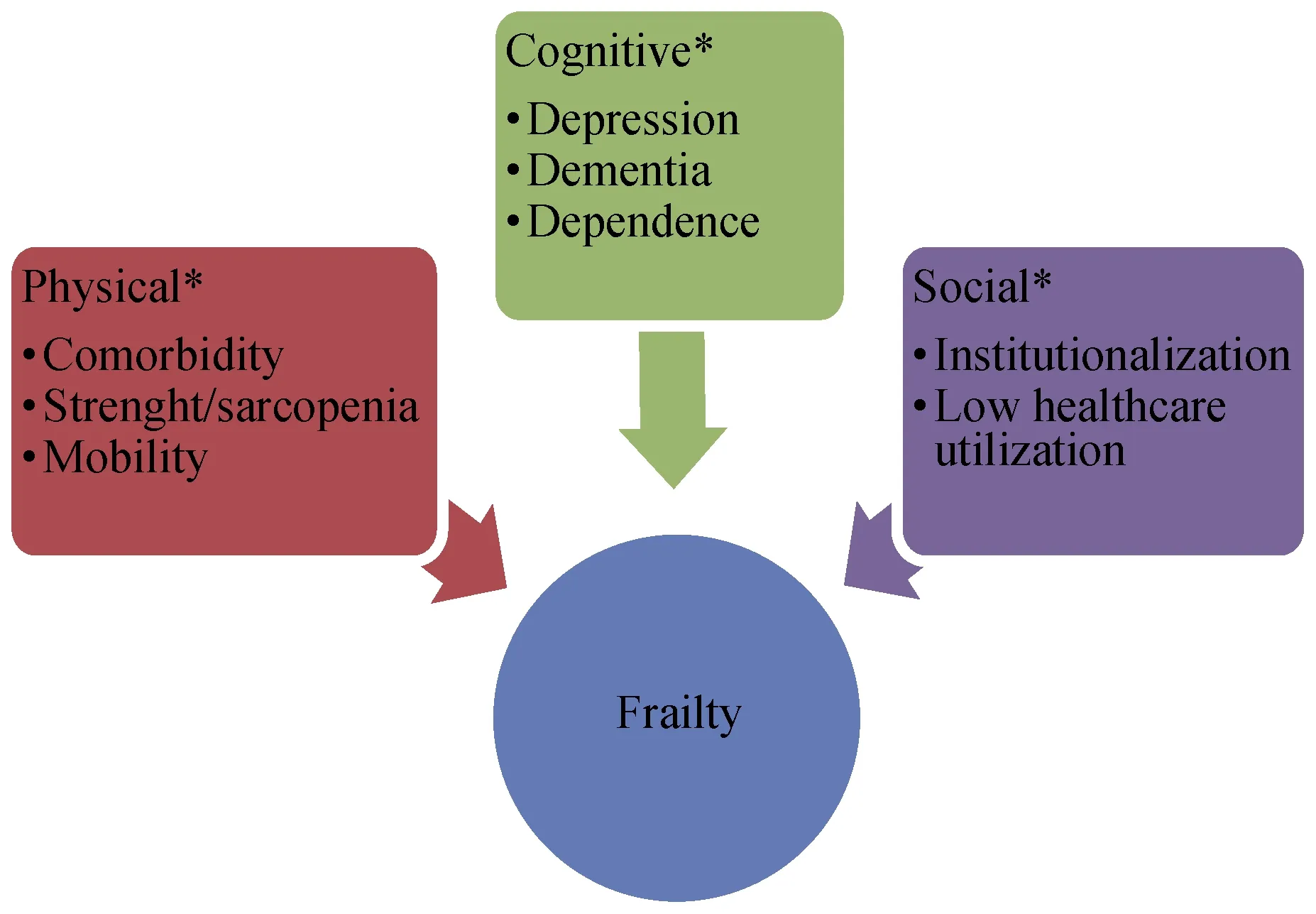
Figure 1. Frailty dimensions. *These barriers are more marked in frail women.
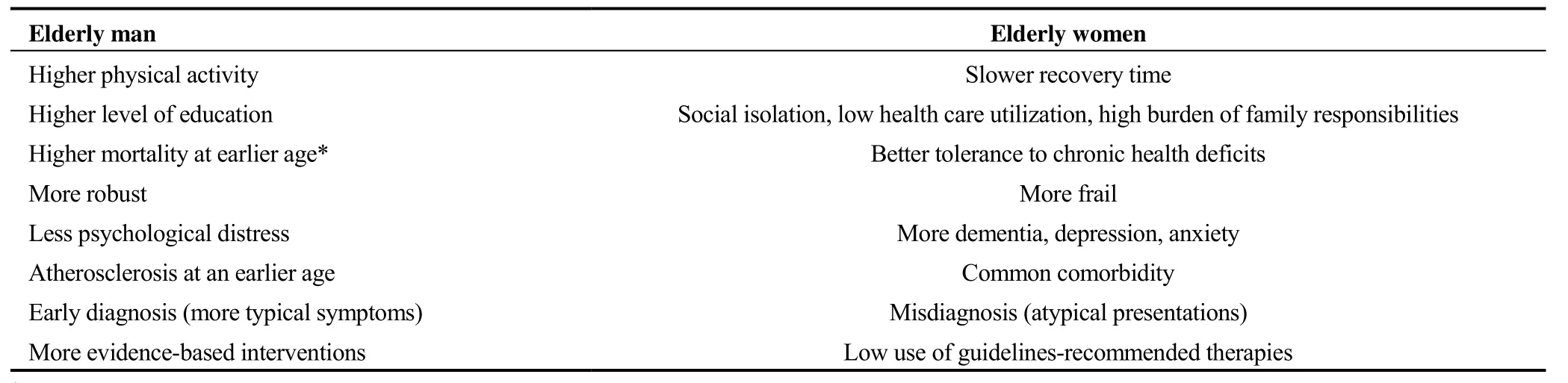
Table 1. Differences in the clinical profile of elderly men and women with acute coronary syndrome.
Frailty has crucial implications in ACS,[8]as it has been associated with an increased risk of mortality,[11,12]longer hospital stay, resources consumption,[13]and specific complications such as delirium and dependence.[14]Female sex is an independent predictor of frailty in elderly patients with ACS,[15]and it is also associated with higher mortality, so frail elderly women constitute an especially high-risk group(Figure 2).[10,16]
The diagnosis of frailty needs a comprehensive geriatric assessment,[17]it should be incorporated in the routine risk stratification to add to classical risk scores (GRACE and CRUSADE).[18-20]It is noticeable that female sex is an important predictor of bleeding, such as contemplated in the CRUSADE score for post-myocardial infarction bleeding risk estimation. However, female sex is not included in the GRACE score for risk estimation.[21]GRACE score has a good predictive accuracy, although this accuracy is lower in women than in men.[22]
Frail scale is a simple and reliable tool that it has an acceptable discriminative capacity in patients with ACS.[19]Elderly women more frequently frail than men.[16,23]This consideration is of interest, as frailty is associated with worse outcomes after percutaneous coronary intervention,[24]it is with higher mortality and longer hospital admission; but further studies are needed in order to establish if a conservative management could be a better option in frail patients.
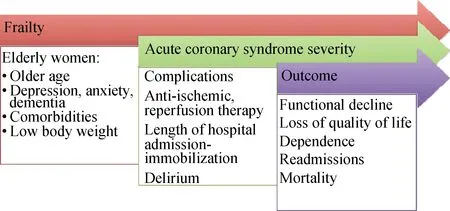
Figure 2. Initial evaluation of frail elderly patients and important considerations.
2.2 Sex, symptoms and diagnosis
The most common form of presentation of ACS in the elderly is non-ST segment elevation myocardial infarction or unstable angina, as it is less than 30% present with ST segment elevation.[11,14]Symptoms in patients with advanced age are frequently atypical, it may be masked by the existing comorbidity, and both factors are more frequent in women than in men. The association of female sex with more atypical symptoms,[16,25,26]it frequently leads to delays in diagnosis and treatment that partially explain the poor prognosis seen in females. In fact, elderly women with ACS an no typical chest pain are commonly underdiagnosed and mistreated,[26]and they have a higher risk of mortality. The most common atypical symptoms are shown in Table 2.Physiopathology of ACS in elderly women is also different,as type 2 myocardial infarction caused by oxygen supply-and-demand mismatch is more common in females than in males.[27]
2.3 Frailty, sex, and treatment
Elderly frail women are severely underrepresented inACS clinical trials. Due to this reason, there is great uncertainty for regarding their ideal therapeutic approach. Current guidelines recommend an invasive management in all ACS,[20]but the initial evaluation should include frailty and dependence assessment.[28]A small study showed a reduction in hospital admissions when an invasive approach was performed in frail elderly patients.[29]However, only a third of the patients were women in this observational study. In fact, the superiority of an invasive intervention in this type of patients is unclear,[30]and in case coronary angiography is performed, its ideal timing is also uncertain.
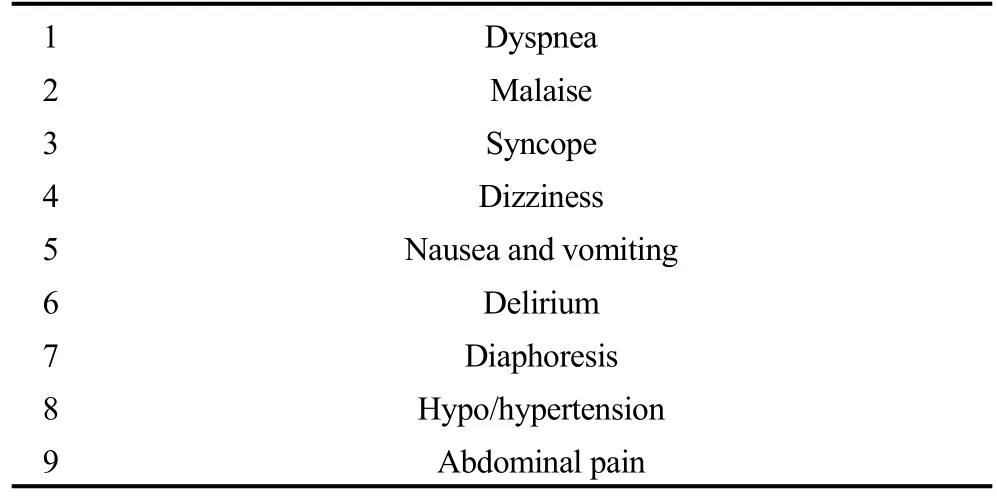
Table 2. Common atypical presentations of acute coronary syndrome in frail elderly women.
A study without frailty measurements showed that women have lower revascularization rates than men,[31]and that patients who do not undergo coronary angiography and revascularization seem to have worse prognosis.[31]Invasive therapies are probably underused in frail elderly patients,but revascularization alone may not be sufficient to improve prognosis, and it is associated with procedure complications.[32]The randomized comparison between the invasive and conservative strategies in elderly frail patients with non-ST elevation myocardial infarction (MOSCA-FRAIL)clinical trial is currently evaluating the effect of an invasive approach in frail elderly patients with non-ST segment elevation ACS.[33]
Antithrombotic therapy is mandatory after ACS. However, there is frequently a major concern regarding the risk of bleeding resulting from double antiplatelet therapy in patients with advanced age. This is even more true in women, as female sex is associated with a high bleeding risk.[34]For this reason, elderly patients, and particularly frail women less frequently receive double antiplatelet therapy.[18]However, in the targeted platelet inhibition to clarify the optimal strategy to medically manage ACS (TRILOGYACS) trial, even though frailty was a marker of poor prognosis, it was not associated with bleeding.[18]Due to the coexistence of atrial fibrillation (it is very common in these elderly patients), the need for chronic anticoagulation is another important point that must be taken into account.This situation is particularly challenging among women,because female sex is a well-known risk factor for thromboembolic events, as it has been reflected in CHA2DS2-VASc score,[35]although it is also an important predictor of bleeding.[36,37]The risk of bleeding associated with triple therapy (double antiplatelet therapy and anticoagulation) is very high, and the triple therapy period should be shortened as much as possible.[38]Alternatives that include a novel direct oral anticoagulant and a single antiplatelet agent seem safe,[20,38]although there are no studies specifically designed for elderly women and frail patients. Table 3 shows the existing evidence about the usual therapies in acute coronary syndrome, applied to frail elderly and women.
Cardiac rehabilitation is an intervention of great interest for frail patients, given the potential reversibility of this condition and the importance of muscle strength and fitness.[39]So, it is paradoxical that women and frail patients are frequently excluded from cardiac rehabilitation programs. In fact, elderly females probably would benefit more than other groups, given the proven effects of cardiac rehabilitation on mobility regain, strength, balance, medical therapy optimization and nutrition.[40]
2.4 Complications
Complications of ACS are more frequent in the elderly,and their severity is also increased in patients with advanced age.[41]Complications can be divided into those related to ACS, comorbidity, and geriatric syndromes. Mechanical complications incidence has declined during the last decades, as reperfusion therapy has become widespread, particularly primary percutaneous coronary intervention. However, they are associated with age, and their mortality is still high.[42]As we have seen, revascularization is less commonly performed in elderly and frail women, so this group is at special risk of this complication.[43]
Elderly patients have a high risk of thrombotic and bleeding complications. Frailty by itself is not associated with an increased bleeding risk,[44]however, female sex is a clear predictor of bleeding.[45]In fact, female sex is included in the classic scores to estimate bleeding risk like the CRUSADE score.[20]Some of this excess risk is due to a relative overdose of antiplatelet and antithrombotic medications in relation to lower weight and lower lean mass.[36]In elderly patients, comorbidity is also associated with major bleeding, especially patients with a history of chronic kidney disease, low body weight, malnutrition, anemia, chronic anticoagulation, and malignancies.[44]
Delirium is an important complication in elderly frail patients with ACS. Women are older, and they have a more common history of dementia and cognitive decline,[16]so they are highly predisposed to this complication.[46]Mortality and length of hospital stay are higher in patients with delirium, so it should be prevented and treated.[46]There are several factors associated with delirium during hospital admission, such as polypharmacy, illness severity, previous cognitive impairment, dehydration and sleep disorders.[14,46]Anti-psychotic drugs may be associated with an unacceptable rate of adverse effects and they are not efficacious for delirium prevention. Physical restraint should also be avoided. Encouraging early mobility, providing calendars and clocks, nocturnal resting and family support are useful alternatives.

Table 3. Evidence-based interventions applied to elderly frail patients after an acute coronary syndrome and reported sex-related differences.[11,45,52]
2.5 Prognosis
Frail elderly women have increased mortality after an ACS.[16,32]Figure 3 shows the interaction between the differential characteristics of elderly women with ACS and the poor prognosis. Hospital readmissions are common in patients with advanced age. A previous multicenter registry showed that female sex was a strong predictor of readmission for recurrent ACS and revascularization.[47]As we have already pointed out, there are important inequalities between the sexes after an ACS, and women are less likely to undergo revascularization therapy and receive less potent antiplatelet agents. These differences may explain the higher frequency of re-admissions of ischemic causes in women.
A previous study showed that frail patients had a higher risk of all-cause mortality,[32]but cardiovascular mortality was similar to non-frail patients. This excess in non-cardiovascular deaths may be attributed to extra-cardiac comorbidities[28,48]and complications, that they have implications in therapeutic management and clinical decisions. Bleeding is a vital adverse outcome, and women are at high risk of presenting this adverse event.[36]
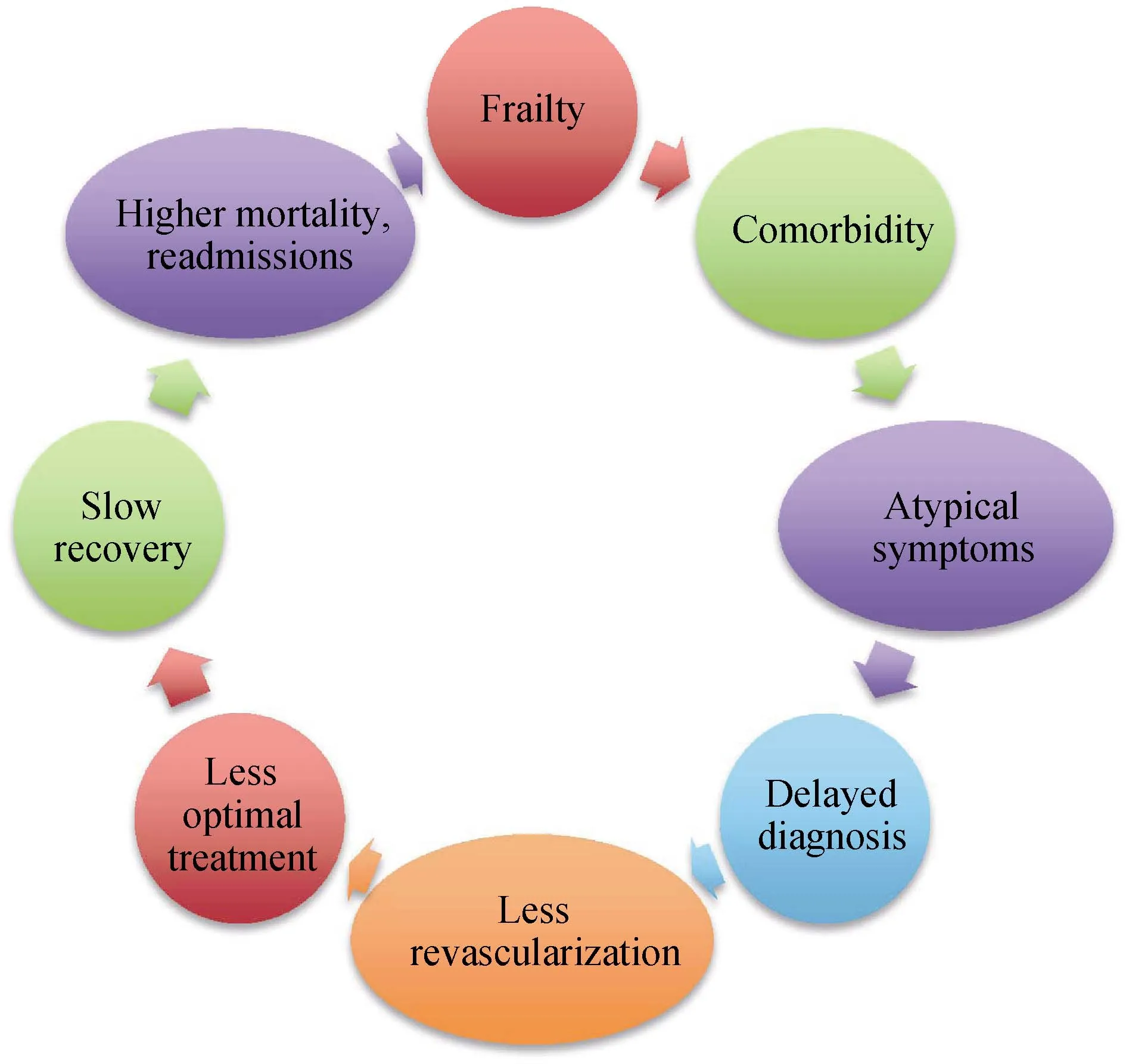
Figure 3. Special characteristics of acute coronary syndrome in elderly women.
Quality of life is a very important aspect, above life expectancy. It has been described that elderly women have a poorer quality of life than men.[49]Therefore, considering that frailty implies a social isolation and dependence of the patient, the interventions should be specifically directed to their prevention and treatment; at the same time, the patient and family preferences should be taken into account. A multidisciplinary approach is advisable to ensure the continuity of patient care.
Taking into account the social isolation and low use of health resources in elderly frail women,[50]it is important to raise awareness among family members and health personnel to promote participation in rehabilitation and multidisciplinary programs,[51]it is also important for improving outcomes and quality of life.
3 Conclusions
Frailty is common among elderly patients with ACS.Women present a greater degree of frailty and they have a poor prognosis. Most elderly women seem to benefit from guideline-recommended medical therapies, although undertreatment is frequent. Bleeding is more common in women than in men, but frailty itself is not associated with an increased bleeding risk. Further studies are needed in order to elucidate the optimal management of frail elderly women with ACS.
 Journal of Geriatric Cardiology2019年2期
Journal of Geriatric Cardiology2019年2期
- Journal of Geriatric Cardiology的其它文章
- Removal of refractory thrombus by 5F child catheter in patients with subacute myocardial infarction
- A rare case of primary well-differentiated angiosarcoma of the right atrium
- Impact of main vessel calcification on procedural and clinical outcomes of bifurcation lesion undergoing provisional single-stenting intervention:a multicenter, prospective, observational study
- Bleeding risk assessment in elderly patients with acute coronary syndrome
- Frailty in patients admitted to hospital for acute coronary syndrome: when,how and why?
- Clinical and prognostic implications of delirium in elderly patients with non–ST-segment elevation acute coronary syndromes