
Indications and contraindications for shock wave lithotripsy and how to improve outcomes
2018-12-25 02:22:18LukeReynoldsTadKroczakKennethPace
Asian Journal of Urology 2018年4期
Luke F.Reynolds,Tad Kroczak,Kenneth T.Pace*
Division of Urology,St.Michael’s Hospital,Toronto,Canada
KEYWORDS Kidney calculi;Nephrolithiasis;Urolithiasis;Extracorporeal shock wave therapy;Lithotripsy
Abstract For over 35 years shock wave lithotripsy has proven to be an effective,safe and truly minimally invasive option for the treatment of nephrolithiasis.Various technical factors as well as patient selection can impact the success of the procedure.We used published work focusing on outcomes of shock wave lithotripsy,risk of complications,and strategies for improving stone fragmentation to create this review.Multiple patient and technical factors have been found to impact success of treatment.Skin to stone distance,stone density and composition,size and location of the stone within the urinary system all influence stone free rates.A slower rate with a gradual increasing voltage,precise targeting,proper coupling will improve stone fragmentation and decrease risk of complications.The selection of appropriate patients through a shared decision making process and attention to the technical factors that improve stone free rates is key to providing an effective treatment and patient satisfaction.
1.Introduction
Shock wave lithotripsy(SWL)has been a safe and effective non-invasive treatment option for nephrolithiasis since the early 1980s[1].Since then,lithotripter technology has been refined,and indications for SWL have expanded.It is an attractive option for patients as it provides a truly minimally invasive approach to achieve overall stone free rates(SFR)approaching 75%[2].As with any procedure,case selection and technique are critical to optimize outcomes,minimize morbidity and maximize SFR.
Before embarking on SWL treatment,it is vital to discuss the treatment options available(including endourologic options)with patients in order to help patients select their optimal management option.Patients need to be carefully selected for both reasons of safety and for appropriateness of treatment.A clinical history,physical exam,urinalysis,routine blood work and a coagulation profile are mandatory to assess for contraindications,risk factors of complications and suitability for treatment.While cross sectional imaging with non-contrast computed tomography is not a prerequisite to SWL treatment,it does provide valuable information that can affect the shared decision-making process and provides prognostic information on SWL outcomes.While overall success rates are high and complications are low,this can only be said for patients who are properly selected and their treatment optimized.
Although ureteroscopy and percutaneous nephrolithotomy(PCNL)have higher SFR especially for larger stones,it is important to consider the patient’s expectations and wishes.Patient satisfaction and preference of the various stone treatments have not been extensively studied,and thus far,studies do not demonstrate a clear preference of treatment[3-5].Whereas the treating urologist typically regards SFR as the most important factor in the decision making process,the requirement of ureteric stents,postoperative lower urinary tract symptoms,return to activity and the need for multiple treatments have all been shown to impact the patient’s experience.
The aim of this review was to describe the current indications and contraindications for SWL and to examine strategies that improve outcomes while minimizing potential risk.We used original researches,review articles and guidelines published on EMBASE,PubMed and MEDLINE to create this document.
2.Contraindications
Good outcomes are dependent on treating patients safely and without added risk.Commonly cited absolute contraindications to SWL include pregnancy,coagulopathy or use of platelet aggregation inhibitors,aortic aneurysms,severe untreated hypertension,and untreated urinary tract infections.
SWL in pregnancy has been associated with low birth weight,placental displacement,miscarriage,and therefore the procedure is contraindicated[6,7].Aortic aneurysms pose a bleeding risk for patients undergoing SWL and classically,are included in the list of contraindications.The literature,however,ismixed on the safety of SWL in patients with aneurysms,with some case reports outlining complications,while other documents safe treatment[8,9].
A more common risk factor for bleeding is patients with a bleeding diathesis and use of anti-platelet,antithrombotic or anticoagulant medications,particularly when the kidney is included in the blast-path of SWL treatment(i.e.for renal and upper ureteral stones)[10].Although no randomized studies have been performed to assess the safety of antithrombotic medications in the setting of SWL,there are a number of case reports that demonstrate bleeding complications in these patients[11-13].In order to decrease the bleeding risk associated with anti-platelet therapy it is necessary to withhold these medications well in advance to the procedure[14].Attention should be paid to renally excreted medications as patients with stone disease may have renal dysfunction and require a longer wash-out period before reaching a normal coagulation profile.Prior to holding any of these agents,it is important that it is safe to do so from a coronary stent,coronary artery disease,cerebrovascular disease or venous thrombosis perspective(depending on the indication).Some patients at particularly high risk may require bridging anticoagulation with heparin to minimize the period of time off anticoagulation[15].In high-risk patients,SWL should be deferred until it is safe to hold these agents or alternative treatment approaches(such as ureteroscopy)should be considered,since it can be performed safely while patients are anticoagulated(unlike SWL).
Hypertension is another significant risk factor for bleeding post-SWL.Untreated or severe hypertension is an absolute contraindication as multiple studies have linked this to increased bleeding and perinephric hematoma[16].Even patients with controlled blood pressure have increased bleeding risk[17].Diabetes,increased age,and obesity have also been associated with an increased bleeding risk[18-20].
Bacteriuria is a common finding among patients with infected stones,catheters,nephrostomy tubes and the elderly[21-23].Urinary tract infections are a common complication seen in up to 5%of patients undergoing SWL[24].Pyelonephritis or sepsis are more rare,but are possible,particularly if patients with untreated bacteruria(or untreated urinary tract infection)undergo SWL.A urinalysis is mandatory before undergoing SWL.If bacteriuria and pyuria are present(particularly with positive nitrites),patients should be treated based on urine culture sensitivities before undergoing lithotripsy.Particularly close attention needs to be paid to patients with a history of prior urinary tract infections, struvite stones, indwelling drainage tubes(foley catheter,ureteric stents,nephrostomy tubes),diabetes,the frail elderly,immunosuppressed or immunocompromised states[25].If patients are found to have bacteruria on the day of SWL,intravenous antibiotics based on local resistant patterns should be administered 1 h prior to treatment.Prophylaxis should be considered for patients with risk factors of infection(including indwelling tubes).Without bacteriuria or risk factors,routine antimicrobial prophylaxis for all patients is unnecessary[26].
3.Patient selection
3.1.Stone location and burden
Stone location and overall stone burden are two of the most important factors when counseling patients on the likelihood of a successful SWL treatment.Staghorn calculi and stones larger than 2 cm in size are better served with more invasive procedures(such as PCNL),and are generally not recommended for treatment with SWL[27,28].SWL success rates and SFR for stones larger than 2 cm are considerably lower than those for smaller stones.However,if patients are informed of this,are motivated to avoid more invasive procedures,and are willing to accept the risks of multiples treatments,failure and steinstrasse,SWL can be considered.This is also true for patients with greater stone burdens who are not optimal candidates for general anesthesia,since SWL can be performed under intravenous sedation or local anesthetic[29].Placement of a ureteric stent is an important consideration when treating larger stones(greater than 15 mm×15 mm)to minimize post-SWL colic and obstruction.
Stone location is another predictor of SWL outcomes.Lower calyceal(LC)stones can be fragmented just as well as those in other locations,but clearance of fragments after SWL is reduced due to the dependent nature of the lower pole and the width and length of the LC infundibulum.Lower pole stones>10 mm treated with SWL have lower SFR outcomes than PCNL.In a randomized trial comparing PCNL vs.SWL for stones 14 mm in size in the lower pole the SFR were dramatically superior with PCNL(95%vs.37%)[30].In this study,size was inversely related with SFR.Although PCNL had significantly higher SFR for stones<10 mm,63.6%of patients were successfully treated with SWL.Another randomized study found similar results with PCNL having superior SFR at 3 months for stones less than 20 mm(96.7%vs.54.8%)although the majority of the patients had calcium oxalate monohydrate stones.Again,as the size of the lower pole stone increased,the SWL SFR decreased[31].There are strategies available to facilitate the clearance of fragments from the LC after SWL:postural inversion,with diuresis and mechanical percussion can render about 60%of these patients stone free[32].
In contrast to PCNL,two randomized trials showed no difference in SFR between SWL and ureteroscopic lithotripsy(URS)[3,33].Sener et al.[34]did find an improvement with URS(100%success defined as fragments less than 3 mm post-URS,vs.a very respectable 91.5%post-SWL).As the size of lower pole stones increases,ureteroscopy outperforms SWL.Studies have found that for stones 10-20 mm located in the lower pole,treatment with SWL lead to increased retreatment rates[4,33,35]and lower SFR [4,35].Overall success rates of SWL for stones 10-20 mm in the lower pole range 34%-78%.
A recently published systematic review has demonstrated the effectiveness of SWL in the ureter.High rates of success can be achieved with both URS as well as SWL(Table 1).Compared to URS,single-treatment SWL has a lower SFR for ureteric stones with the exception of stones greater than 1 cm in the proximal ureter in which SWL and URS have comparable outcomes.In addition,stone-free status is faster with URS compared to SWL.SWL,however,remains the least morbid treatment,and can generally be performed without a ureteric stent(which is a major source of patient morbidity following URS)[2].
Another factor to consider is that while most studies demonstrate higher SFR with more invasive surgery,repeat SWL procedures can improve SFR by up to 10%-20%[36].This approach is a good option for patients who are motivated to proceed with SWL.Multiple treatments should be reserved for patients whose stones fragmented reasonably well during the first session[29].
3.2.Other indications
SWL treatment of nephrolithiasis within transplant kidneys has been reported.The procedure is safe and has acceptable SFR [37].Great care should be taken in thiscircumstance to control for any modifiable risk factors and to ensure the kidney does not become obstructed post procedure.
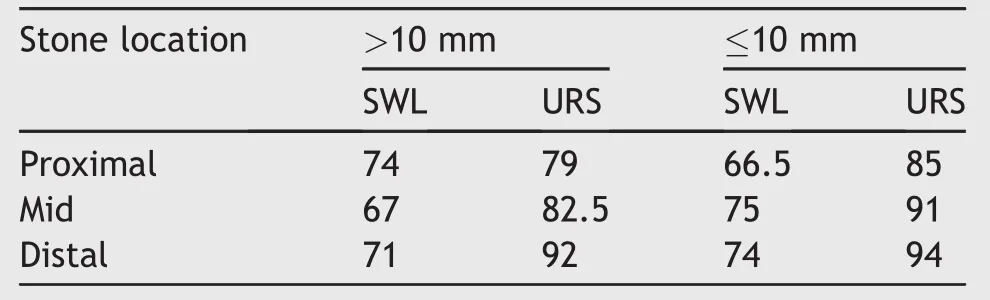
Table 1 Stone free rates(%)with single treatment of SWL and URS for ureteric stones[2].
4.Stone characteristics
In addition to stone factors,there are a number of patient factors that influence the success of SWL such as body habitus,unfavorable anatomic abnormalities and factors that put the patient at risk for complications.
4.1.Skin to stone distance
Obesity is increasing in the general population and is becoming more prevalent in stone formers.It can provide challenges with on-table positioning,radiographic quality and in severe cases it can exceed the focal distance of lithotripters.Skin to stone distance of less than 10-11 cm has been shown to be an independent predictor of SFR following SWL[38,39].Along the same lines,a higher body mass index(BMI,>30 kg/m2)was associated with decreased success[40].However,there is conflicting evidence that BMI is a strong predictor of SWL outcomes[41,42].Another factor to consider when managing patients with obesity is that it is linked to increased risk of post procedure hematoma[16].
4.2.Stone composition
Stone composition hasa significantimpacton SWL outcomes.Calcium oxalate monohydrate,cysteine,and calcium phosphate stones are relatively SWL-resistant[43,44].This effect is exacerbated with larger stones.Although these stones are typically thought to be resistant to SWL there are variations within the same composition[45,46]and often stones have a mixed composition making them more amendable to fragmentation.Uric acid stones are quite“fragile”for SWL,but can be challenging to target with fluoroscopy since they are radiolucent.Pyelography and ultrasound are options for real time targeting of radiolucent stones during SWL.Assessment of stone passage post procedure will require either a computed tomography or ultrasonography for these patients.
Whenever possible it is recommended to obtain stone fragments for analysis of composition.This information will help guide dietary and medication recommendations and may alter decision making if future treatments are required.Repeat stone analyses can be helpful as composition can change over time[47],potentially due to SWL treatment[47,48].
4.3.Stone density
Another useful factor to consider when assessing the stones susceptibility to fragmentation is the stone’s density as measured by the Hounsfield units(HU).Various studies have demonstrated that as the HU increases(>970 HU)the success of fragmentation and clearance of stones decreases[49-52].In a prospective clinical trial,a linear relationship was demonstrated between HU and SFR.Stones that had a density<970 HU were significantly more likely to be successfully treated with SWL compared to harder stones(98%vs.38%)[49].Patients should be counseled about lower SWL success rates for stones with a density>1000 HU[53].
More recently,investigators have suggested a new predictor for SWL outcomes:The variation coefficient of stone density(VCSD).VCSD=(standard deviation ofstone density)/(mean stone density)×100.It was found to be a stronger predictorofSWLsuccessthan mean stone density asmeasured by HU for upper urinary tract calculi,likely because it accountsfordifferencesin composition and crystalline lattice of stones better than simple HU density averages do[54].
4.4.Other patient factors to consider
For stones located in the lower calyx,assessment of the infundibulopelvic angle,and the length and width of the infundibulum to the lower pole can give helpful information for prognosis.Favorable features of the lower pole infundibulum that are associated with increased SFR are length<3 cm,width>5 mm and an infundibulopelvic angle greater than 90°[55].SWL should be used judiciously for patients with kidney fusion or malrotation anomalies as the calyceal anatomy and drainage is often altered leading to poor outcomes[56].Calyceal diverticuli also present a challenge for stones clearance after fragmentation and are often better served with PCNL or URS to render the patient stone free[57].The presence of hydronephrosis has also been associated with worse outcomes[58,59].The potential deleterious effect of hydronephrosis with stone passage is thought to be due to edema from stone impaction and decreased ureteral peristalsis and hydraulic pressure.
5.Improving outcomes and preventing complications
5.1.Shock rate
SFRs and risk of complications are linked to the shock rate of treatment.The rate of shock administration is typically between 60 and 120 per minute.A shock rate of 60 shocks/min has two major advantages:Improved efficacy as a higher frequency decreases the negative pressure of the shock wave[60,61],and potential decrease in the risk of renal injury.Clinical studies have demonstrated up to a 16%improvement treating smaller stones and up to a two-fold improvement treating larger renal stones(>100 mm2)using a rate of 60 shocks/min vs.120 shocks/min[62-64].A rate of 60 shocks/min has also been shown to be beneficial for treatment of ureteric stones with a 16%improved SFR and also decreased need for auxiliary procedures[65].A recent meta-analysis demonstrated that a rate of 60-70 shocks/min and 80-90 shocks/min had significantly higher success rates compared to a rate of 100-120 shocks/min(odds ratio 2.2 and 2.8 respectively)[66].If stone fragmentation is more effective,then patients may need less shocks overall which also leads to less parenchyma damage[67].
5.2.Number of shocks
As the number of delivered shocks per session increases,both the rate of stone fragmentation as well as risk of damage to tissues increases.The specifications of individual lithotripters limit the amount of shocks delivered per session but most range between 2 000 and 4 500 shocks/session.The location of the stone also influences the maximum number of shocks that can be delivered safely.Stones that are not within the shock blast of the kidney can be treated with 4000 or more shocks and for the majority of treatments of upper ureteral and renal stones the range is 2000-3500 shocks[68].The precise“optimal” number of shocks is not clear,but as the number of shocks delivered increase,the risk of damage to tissue increases[69].Other factors to consider are energy level,patient body habitus,as well as characteristics of the stone[39].Certainly once a stone has been adequately fragmented,treatment should be discontinued.Extra caution should be taken when treating patients that are at a higher risk for complications.
5.3.Ramping
In order to maximize treatment effect and limit surrounding tissue damage protocols of ramping up the energy voltage at the beginning of the treatment or a series of lowenergy pre-treatment shocks followed by a pause have been developed.By using a ramping protocol it allows for anesthesia to better manage pain which is important to prevent movement and subsequent decoupling of the shock head[70].When compared to a fixed voltage protocol ramping improves SFR,while renal damage as measured by urinary excretion of microglobulins is decreased[71-73].Recently,using a porcine model,it was shown that pretreatment(300-500 shocks)at a low voltage without a pause decreases damage to the kidney[74,75].A recent clinical trial supports these in vitro results;stepwise voltage ramping was associated with a lower risk of hematoma(odds ratio 0.39)when compared to a fixed maximal voltage protocol[76].Pretreatment and ramping is thought to cause a vasoconstriction of the parenchymal vessels which may be the mechanism behind the protect effects[77].
Stones should be treated at the maximum energy unless stone fragmentation is clearly seen at lower energy levels.When the shock blast is distal to the kidney the desired vasoconstrictive effect seen with ramping is less relevant as perinephric hematoma is unlikely.
6.Improving hit rate
6.1.Positioning
A simple and important factor to consider is if the shock is being impeded by skeletal structures.With shocks being delivered from the back the transverse processes,sacroiliac bone and the pelvic skeleton can all cause interference.Treatment in a modified supine position can provide a solution for upper ureteric stones,and stones in the mid ureter may be best treated in the prone position[78].When treating stones in the prone position care should be taken to assess for bowel gas that lies within the path of the shock wave.Bowel gas will absorb the energy of the shock and case reports of bowel perforation from prone treatment have been described[79].A trans-gluteal approach from the supine position can effectively target stones giving rates of success similar to upper ureteric stones[80].In patients with skeletal abnormalities such as scoliosis,spinal or pelvic hardware,etc.a simulation of lithotripsy can be helpful to assess if an unobstructed path for the shock wave can be achieved before sedating the patient.
6.2.Imaging and targeting
Regardless of the imaging modality used to target the stone,real time,in-line and frequent imaging is important to ensure the shocks are reaching their target.Increasedfluoroscopy time has been associated with increased SFR[81].Excessive stone motion can lead to the stone moving outside of the focal zone leading to decreased hit rate,therefore,it is important for repeat imaging to be performed throughout the treatment[82].In efforts to decrease stone motion caused by respiration,abdominal compression plates[83]or a compression belt[84]has proven beneficial.Interestingly,SWL performed in conscience patients has shown to have less stone motion compared to anesthetized patients[85].It can be helpful to target the stone on expiration to increase the duration of time stone is in the focal zone.
Ultrasound has become an increasingly important imaging modality for stone targeting as it reduces radiation exposure,allows for targeting of radiolucent stones and provides continuous real time monitoring of the procedure[86].Recently,a randomized control trial enrolling 114 patients to ultrasonography vs.fluoroscopy for visualization of the stone during SWL demonstrated that ultrasonography was non-inferior to fluoroscopy with the end points of SFR and asymptomatic residual fragment(<4 mm)rates at 3 weeks[87].
6.3.Coupling
In order for the shocks to be effectively delivered,the energy generated by the shock head must travel without impedance.With modern lithotripters,a common issue is that air bubbles can get trapped in the coupling zone either by patient movement or improper media application.Various studies have demonstrated that breaks in coupling lead to worse fragmentation in vitro[88,89].
To avoid acoustic interference care should be taken to ensure that patients have optimal pain control thus preventing movement,and subsequently air bubbles being introduced into the blast path.Applying a generous amount of low viscosity coupling medium[90]directly to the shock head[91]without using pumping devices can be beneficial.In efforts to improve detection of air bubbles which is typically not visible to the operator,surveillance cameras can be used[90].
7.Strategies to promote stone passage
7.1.Stenting
Following SWL various interventions have been implemented to try and improve passage of stone fragments.The use of stents in SWL can be useful as well as detrimental to stone passage.Circumstances where stenting can be helpful is for obstructing stones,a large stone in a solitary kidney,obstruction with infection,renal failure and intolerable pain[2].Routine stenting for ureteral stones has shown to decrease SFR by 15%-22%for stones less than 10 mm[92-94],and the negative effect may be amplified for larger stones[95].The role of ureteric stents for renal calculi has not been shown to be of any benefit for renal stone clearance and does not seem to have an obvious impact on the development of steinstrasse[96,97].A period of stenting pre-SWL may provide a benefit for stone clearance for larger renal stones[98].In addition to negative evidence for SFR,stenting creates a significant burden in terms of lower urinary tract symptoms and ancillary procedures[99].
7.2.Medications
Among various medications that have been theorized to improve stone passage following SWL only citrate and tamsulosin have been proven effective.Although there have been conflicting trials over the years,a recent meta-analysis that included 21 randomized controlled trials has demonstrated that the use of tamsulosin post-SWL improves stone passage with a risk ratio of 1.2 and appears to be more beneficial for stones located in the distal ureter as well as larger stones(11-24 mm)[100].Also,Chen et al.[100]demonstrated that the use of tamsulosin post-SWL shortened time to stone clearance,decreased colic episodes and pain medication requirements.In one study potassium citrate decreased calcium oxalate stone recurrence and decreased residual fragments post SWL at 1 year of follow-up[101].
8.Conclusion
The benefits of SWL include a fast recovery time,low risk of complications and that it is a minimally invasive day procedure that can be performed under sedation without ureteric stenting.SWL provides an excellent option for patients suffering from nephrolithiasis.With optimization of treatment and patient selection we can better prognosticate,prevent complications and improve outcomes.
Author contributions
Study Concept and Design:Luke F.Reynolds,Kenneth T.Pace.
Data Acquisition:Luke F.Reynolds,Tad Kroczak.
Data Analysis:Luke F.Reynolds,Tad Kroczak,Kenneth T.Pace.
Drafting of Manuscript:Luke F.Reynolds,Tad Kroczak,Kenneth T.Pace.
Critical Revision of the Manuscript:Luke F.Reynolds,Kenneth T.Pace.
Conflicts of interest
The authors declare no conflict of interest.
 Asian Journal of Urology2018年4期
Asian Journal of Urology2018年4期
- Asian Journal of Urology的其它文章
- Miniaturised percutaneous nephrolithotomy:Its role in the treatment of urolithiasis and our experience
- Present indications and techniques of percutaneous nephrolithotomy:What the future holds?
- Ureteral stents in urolithiasis
- Retrograde intrarenal surgery:An expanding role in treatment of urolithiasis
- Medical therapy for nephrolithiasis:State of the art
- Defining metabolic activity of nephrolithiasis-Appropriate evaluation and follow-up of stone formers