
Current status of laparoscopic and robotassisted nerve-sparing radical cystectomy in male patients
2016-04-26 03:17:15JianHuangXinxiangFanWenDong
Asian Journal of Urology 2016年3期
Jian Huang,Xinxiang Fan,Wen Dong
Department of Urology,Sun Yat-sen Memorial Hospital,Sun Yat-sen University,Guangzhou,China
Current status of laparoscopic and robotassisted nerve-sparing radical cystectomy in male patients
Jian Huang*,Xinxiang Fan,Wen Dong
Department of Urology,Sun Yat-sen Memorial Hospital,Sun Yat-sen University,Guangzhou,China
Nerve-sparing;
Radical cystectomy;
Laparoscopy;
Robot-assisted
laparoscopy;
Male
During radical cystectomy(RC),the neurovascular bundles are easily removed or damaged,leading to varying rates of incontinence and erectile dysfunction.The nervesparing technique was developed to preserve urinary and erectile function.The adoption of laparoscopic and robot-assisted technology has improved visualization and dexterity of pelvic surgeries,thus facilitate the nerve-sparing technique.Although nerve-sparing RC is technically similar with nerve-sparing radical prostatectomy,there are still some anatomical differences. There are mainly three different types of nerve-sparing techniques.Pelvic lymph node dissection(PLND)is another important factor to influence erectile function and urinary continence. Nerve-sparing laparoscopic radical cystectomy(LRC)and robot-assisted radical cystectomy (RARC)may be an optimal treatment choice in well-selected younger patients with lowvolume,organ-confined disease.We should attempt to do,whenever possible,a nerve-sparing cystectomy at least on oneside.However,due to the need of a well-refined surgical technique, nerve-sparing LRC and RARC is now being performed only by experienced urological surgeons. ?2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.Ltd. This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
1.Introduction
Radical cystectomy(RC)with neobladder reconstruction still represents the first choice of treatment for both muscleinvasive and high-risk non-muscle invasive bladder cancer.In recent years,minimally invasive surgery such as laparoscopic radical cystectomy(LRC)and robot-assisted radical cystectomy(RARC)are performed more commonly at many centerswith the technologicaladvancements.The safety andpotential advantages in terms of blood loss,analgesic requirements,improved cosmesisand quick recovery ofLRCand RARC compared to open RC(ORC)have been well established [1-3].At present,the ultimate goal of LRC and RARC is to remove the tumor completely while still maintaining erectile function and urinary continence at the same time.
During RC,particularly ORC,the neurovascular bundles are easily removed or damaged.Varying rates of continence and erectile function have been described after RC in the literatures as the degree of injury to the neurovascular bundles differed from technique to technique[4-6].RC was then modified on the basis of this information to avoid injury to the neurovascular bundles and thus better preserve erectile function and urinary continence in patients undergoing this operation.
Although nerve-sparing RC has been proposed in the 1980s,progress of this procedure actually remained limited over the years[7].However,nerve-sparing radical prostatectomy(RP),which is widely applied formore than 20 years, has achieved a consolidate position in routine clinical practice of every urologic unit[8].Whether the nerve-sparing technique in prostatectomy could be applied in RC is still controversial.Firstly,the innervations of the neobladder after RCisdifferentfrom originalbladderafter RP.Secondly, the voiding pressure of neobladder is much lower than original bladder as the former does not have detrusor muscle.In addition,the pelvic lymph node dissection(PLND)is much more extensive during RC than RP,thus higher branches of pelvic plexus may be injured.Moreover,as urothelial carcinoma is considered to be a potential lethal disease,nervesparing surgery may compromise the oncological safety.
Nevertheless,the adoption of laparoscopic and robotassisted technology has improved visualization and dexterity of pelvic surgeries.Several studies with varying results after nerve-sparing LRC have been published[8-10]. Herein we review the current available literatures concerning the anatomic basis,nerve-sparing techniques,and therapeutic effects of nerve-sparing LRC and RARC in male patients.We aim to clarify the rational nerve-sparing techniques and establish the proper patient selection criteria.
2.Evidence acquisition
A literature search was performed in February 2016,using the PubMed and the Web of Science databases.The following terms and their combinations were searched in Title/Abstract:“nerve-sparing”,“l(fā)aparoscopic”,“robotassisted”,“radical cystectomy”and“male”.Case reports and non-English articles were excluded.Full text case series and their references were reviewed.
3.Evidence synthesis
3.1.New insights of the anatomical basis of nervesparing radical cystectomy
In 1982,Walsh and Donker[11]suggested that erectile dysfunction(ED)was caused by damage to the neurovascular bundles(NVB),which supply the corpora cavernosa.In 1983, Walsh et al.[12]found that the branches of pelvic nerve plexus which dominate corpora cavernosa locate laterally of the prostate capsule and Denonvillier’s fascia.They spread along the post lateral part of the prostate and the urethra, the anteriorwallofthe rectum.These delicate nervesspread along with the blood vessels supplying prostate,seminal vesicle,bladder neck and urethra,and together they form the NVBs which are embedded in the dense fibrous connective fat tissue[12].NVBs play an important role in erectile function and urinary control.By using cadaver models, Costello et al.[13]further detailed the precise anatomy of the NVBs because of their close relationship to the prostate and seminal vesicles.They identified three functional components of the NVBs.The first posterior and posterolateral component runs within Denonvillier’s fascia and the pararectal fascia and innervates the rectum.The second lateral component supplies the levator ani.The third component cavernosal nerves and prostatic neurovascular supply,originally described by Walsh and colleagues[11,12],lie along the posterolateral surface.
Takenaka et al.[14]confirmed that branches of the hypogastric nerve and the pelvic splanchnic nerve are likely to interdigitate at multiple levels,showing spray-like arrangement without clear bundle formation.In addition, Lunacek et al.[15]demonstrated that during the growth of the prostate,the cavernous nerves running along the prostate are displaced more anteriorly and spread,thus forming a concave shape(like a“curtain”)of the NVBs. Therefore,dissection of the NVBs has to start anteriorly to preserve all the nerve fibers that are spread along the surface of the lateral lobes of the prostate.
Although nerve-sparing RC is technically similar with nerve-sparing RP,there are still some anatomical differences.During RC,the lateral portion of each bladder vascular pedicle is stapled with a vascular staple load,and a second staple load is used to divide the proximal portion of the posterior pedicle.Clips and athermal dissection are used to divide the distal portion of the posterior pedicle, staying close to the seminal vesicles,thereby avoiding undue damage to the erectile nerves that are in close proximity lateral to the seminal vesicles[9,16].In addition, a more extended PLND should be performed in RC compared with RP,and the erectile nerves are at risk of injury when the lymph nodes in the presacral and internal iliac area are being removed[17].
3.2.Different techniques of nerve-sparing radical cystectomy
There are mainly three different types of nerve-sparing techniques.Their main features and relative reports are described below(Table 1).
3.2.1.Nerve-sparing cysto-vesicle prostatectomy(NSCVP)
This technique,adopted according to that initially described by Schlegel and Walsh[18]in 1987,includes the“en bloc”removal of bladder,prostate and seminal vesicles only leaving the NVBs intact.This is the most commonly used nerve-sparing procedure which was mainly carried out by a transperitoneal approach,using a combined ante-retrograde bladder dissection in combination with an inter fascial prostatectomy[8].
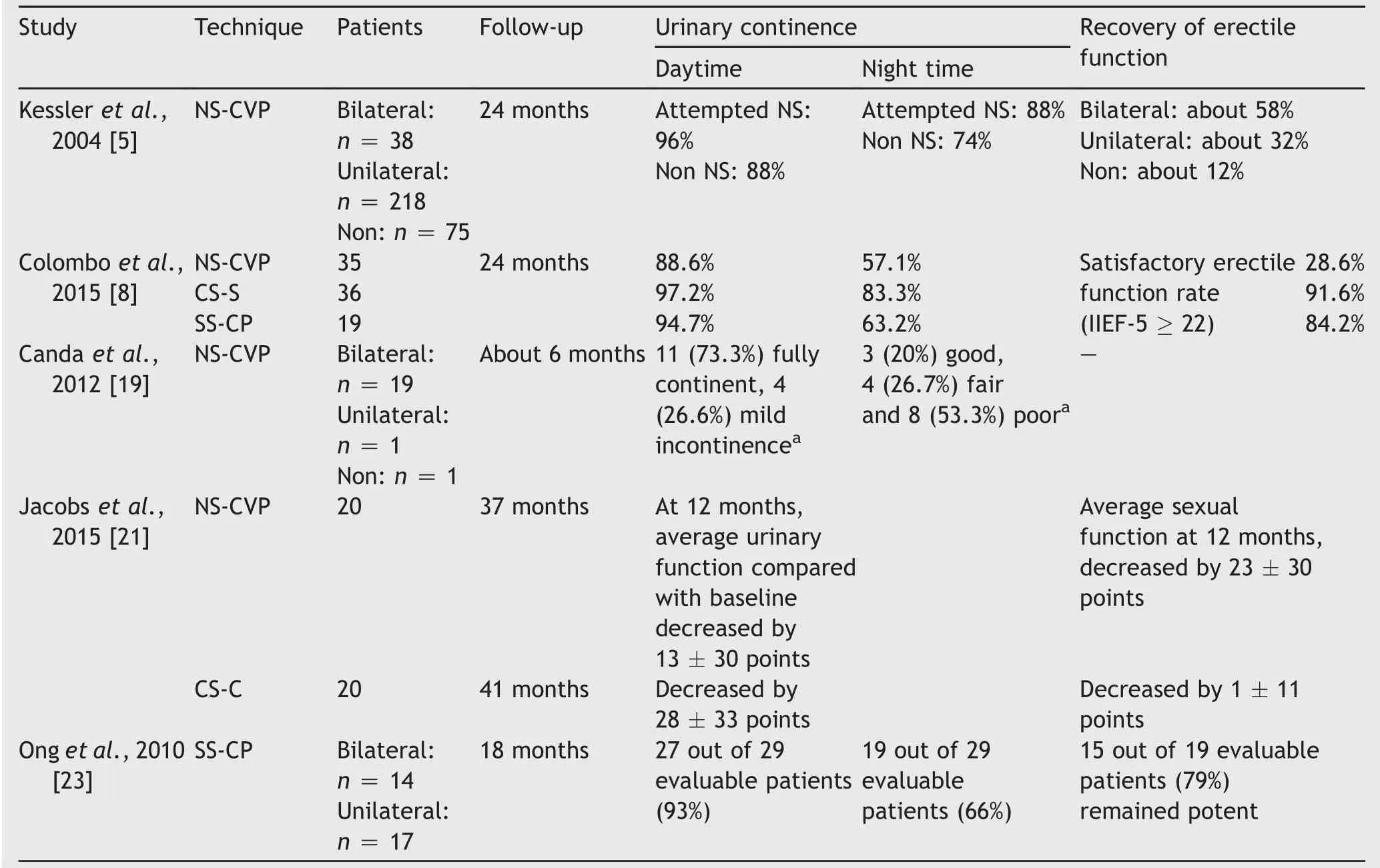
Table 1 Functional outcomes of different techniques of nerve-sparing radical cystectomy.
Kessler et al.[5]assessed factors influencing urinary continence and erectile function after RC and ileal orthotopic bladder substitution in 381 consecutive male patients. These patients were classified into three groups,without attempted nerve-sparing(n=75),attempted bilateral nerve-sparing(n=38)and attempted unilateral nervesparing(n=218).After 2 years of follow-up,58%patients in bilateral nerve-sparing group could achieve recovery of erectile function,32%in unilateral nerve-sparing group,whereas only 12%in without attempted nervesparing group.This study also demonstrated that attempted nerve sparing and age younger than 65 years are associated with improved urinary continence[5].Another study by Colombo et al.[8]reported 35 patients underwent NSCVP,and their functional outcomes showed that 88.6%patients could achieve complete daytime urinary continence, and 28.6%patients could achieve satisfactory erectile function at 24 months after surgery.Canda et al.[19]reported 21 male patients underwent robot-assisted nervesparing RC with bilateral PLND and intracorporeal urinary diversion for BCa,15 were available for postoperative urinary continence evaluation(four died and two were lost to follow-up).Among those,11(73.3%)were fully continent and four(26.6%)had mild urinary incontinence during the daytime.Therefore,daytime urinary continence seems to be very promising in male patients,although the follow-up is currently very limited in this study.On the other hand, for nighttime continence outcomes,three(20%)had good, four(26.7%)had fair and eight(53.3%)had poor UI.Patients with preoperative erectile function(IIEF score>7,n=11) were instructed to use oral phosphodiesterase type 5(PDE-5)inhibitors after removal of the urethral catheter postoperatively.However,only one patient used an oral PDE-5 inhibitor and clearly benefited from its use.Most of the present patients had a decreased libido postoperatively. Additionally,the follow-up is limited;therefore it is not easy to comment on postoperative erectile functional outcomes.The authors suggested that in longer term follow-up increased use of PDE-5 inhibitors and an increase in libido will result in better functional outcomes reflected by increased IIEF scores[19].
3.2.2.Capsule-sparing cystectomy(CS-C)
This technique,described by Colombo et al.in 2001[20], includes a preliminary transurethral resection of prostate (TURP)and then entire removal of the bladder while leaving the prostate capsule,vas deferens,seminal vesicles and NVBs intact.Biopsies of bladder neck and prostatic urethra were obtained at the time of previous transurethral resection of bladder tumors.TURP is carried out togetherwith systematic prostate biopsies before RC in order to exclude prostate cancer[8].
Colombo et al.[8]reported 36 patients underwent CS-C, and their function outcomes showed that 97.2%patients could achieve complete daytime urinary continence,and 91.6%patients could achieve satisfactory erectile function at 24 months after surgery.Another randomized controlled trial by Jacobs et al.[21]compared CS-C vs.NS-CVP,with 20 patients in each cohort.Neither sexual function nor urinary continence could achieve significant differences between the two groups.
3.2.3.Seminal-sparing cysto-prostatectomy(SS-CP)
This procedure was firstly described by Puppo et al.[22] in 2008 and subsequently by Ong et al.[23]and Hautmann et al.[4]in 2010.The main steps include a blunt extraperitoneal antegrade dissection between the posterior bladder wall and the seminal vesicles up to the ejaculatory ducts and a retrograde intrafascial prostatectomy. With this procedure,seminal vesicles,vas deferens and NVBs were left intact into the pelvis.
Colombo et al.[8]reported 19 patients underwent SS-CP, and their functional outcomes showed that 94.7%patients could achieve complete daytime urinary continence,and 84.2%patientscould achieve satisfactory erectile function at 24 months after surgery.Ong et al.[23]reported 31 patients (17 unilateral and 14 bilateral)underwent SS-CP.At last follow-up(median 18 months),27 out of 29 evaluable patients(93%)had daytime continence and 19 out of 29(66%) had nighttime continence.In terms of postoperative potency,15 out of 19 evaluable patients(79%)remained potent.Hautmann et al.[4]reported nine patients underwent SS-CP,and four out of nine patients maintained spontaneous complete tumescence,and five patients had partial tumescence using sildenafil as a successful erectogenic aid.
3.3.The in fluence of PLND on erectile function and urinary continence
In the male,the inferior hypogastric plexus,or pelvic plexus, is responsible for the mechanisms of erection,ejaculation, and urinary continence[17].The pelvic plexus lies within a fibrofatty, flat,rectangular,sagittally oriented plate between the bladder and the rectum[13].PLND might be extended into thisarea.So,PLND isanotherimportantfactor to in fluence erectile function and urinary continence.The pelvic plexus and particularly the erectile nerves are at risk of injury in a standard PLND during the medial dissection in the area of the internal iliac area and towards the bladder wall.A more extended PLND may damage branches of the pelvic plexus providing the cavernous nerves which contribute to erectile function.During extended PLND,the nerves are also at risk ofinjury at their origin in the presacral area and medial to the common iliac vessels[17].In fact, signi ficantly better recovery of erectile function was reported in men with negative lymph nodes compared to those with positive lymph nodes[5].
Studies have shown that extended PLND provides additional survival bene fits for patients with pT3-4 disease,but not for patients with≤pT2 disease[24].In addition,super extended template up to the inferior mesenteric artery dose not provide survival benefit compared with extended PLND [25].Nerve-sparing RCisusually restricted to≤cT2 patients, for whom standard PLND is enough.So para-aortic lymph nodes and presacral lymph nodes should not be removed during nerve-sparing RC,unless there is suspected lymphatic metastasis or palpable lymph nodes during surgery.
3.4.Surgical skills for nerve-sparing radical cystectomy
Many of the NVBs fibers are microscopic and cannot be identified during surgery.Those nervesare located postero-lateral to the seminal vesicles and very close to their tips.Gentle dissection of the seminal vesicles during RC may reduce the risk of injury to these nerves and,in consequence,may improve postoperative potency rates[26].A high intrafascial release of the NVB is performed with a strict athermal technique using Hem-o-Lok clips and metalclips for hemostasis.It is important to not accidentally transect the NVBs during dissection close to the vesicles and the base of the prostate, where the dissection is in close proximity to the NVBs[16].
In addition to a nerve sparing technique,the management of the urethral sphincter mechanism at surgery is of utmost importance.The less damage done to tissue related to the sphincteric mechanism,the more likely patients will be continent.For rapid achievement of continence after surgery,the urethral supporting structures and a maximum of membranous urethral length should be preserved[5].
3.5.Surgical indications for nerve-sparing radical cystectomy
According to the above considerations,the nerve-sparing technique is important for both preservation of sexual function and urinary continence.Men with good erectile function and preferring to preserve their potency after RC may be candidates for preservation of NVBs.However, nerve-sparing RC requires dissection close to the bladder, exposing patients to the risks of positive surgical margins, which may compromise tumor control.Thus,patient selection is critically important when performing nervesparing cystectomy.The risks and benefits of nerve sparing should be assessed according to preoperative sexual function and disease burden.
Firstly,age plays a significant role in the recovery of erectile function after RC.Schoenberg et al.[27]demonstrated that the overall potency of their cohort was 47%. Afterbroken down by decades,men in their40s,50s,60s,and 70s had potency rates of 62%,47%,43%,and 20%,respectively.Kessler et al.[5]also showed significantly better effects of the open nerve-sparing approach on men younger than 65 years compared with those who were older.Patient with a younger age may achieve better outcomes in term of sexual function.In addition,the clinical tumor stage should be restricted within T2 without evidence of disease at bladder neck and a negative urethral margin at the time of surgery is mandatory.Thirdly,we should exclude patients probably with prostate cancer.Prostate specific antigen (PSA)<4.0 ng/mL with normal digital rectal examination (DRE)and normal transrectal ultrasound (TRUS)are required.Additional pre-operative criteria include sexuallypotent before surgery and suitable for orthotropic neobladder.
With the purpose of preservation of sexual function, rectalfunction,and improving urinary continence in patients with or thotopic bladder substitutes,we should attempt to perform at least one side nerve-sparing cystectomy[28]. Unilateral nerve-sparing should be considered on the nontumor-bearing side.Bilateral nerve-sparing may be considered in patients with high risk non-muscle invasive disease or invasive tumors at anterior wall or dome of the bladder[28].
4.Conclusion
Nerve-sparing RC is beneficial for both preservation of sexual function and urinary continence according to current studies.Nerve-sparing LRC and RARC may be an optimal treatment choice in well-selected younger patients with low-volume,organ-confined disease.We should attempt to do,whenever possible,a nerve-sparing cystectomy at least on one side.However,due to the need of a well-refined surgical technique,nerve-sparing LRC and RARC is now being performed only by experienced urological surgeons.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
This review is supported by Yat-sen Clinical Trail Project (No.200501).
[1]Nix J,Smith A,Kurpad R,Nielsen ME,Wallen EM,Pruthi RS. Prospective randomized controlled trial of robotic versus open radical cystectomy for bladder cancer:perioperative and pathologic results.Eur Urol 2010;57:196-201.
[2]Parekh DJ,Messer J,Fitzgerald J,Ercole B,Svatek R.Perioperative outcomes and oncologic efficacy from a pilot prospective randomized clinical trial of open versus robotic assisted radical cystectomy.J Urol 2013;189:474-9.
[3]Lin T,Fan X,Zhang C,Xu K,Liu H,Zhang J,et al.A prospective randomised controlled trial of laparoscopic vs open radical cystectomy for bladder cancer:perioperative and oncologic outcomes with 5-year follow-up T Lin et al.Br J Cancer 2014; 110:842-9.
[4]Hautmann RE,Hautmann O,Volkmer BG,Hautmann S.Nervesparing radical cystectomy:a new technique.Eur Urol Suppl 2010;9:428-32.
[5]Kessler TM, Burkhard FC, Perimenis P, Danuser H, Thalmann GN,Hochreiter WW,et al.Attempted nerve sparing surgery and age have a significant effect on urinary continence and erectile function after radical cystoprostatectomy and ileal orthotopic bladder substitution.J Urol 2004;172: 1323-7.
[6]Zippe CD,Raina R,Massanyi EZ,Agarwal A,Jones JS, Ulchaker J,et al.Sexual function after male radical cystectomy in a sexually active population.Urology 2004;64: 682-5.discussion 5-6.
[7]Pritchett TR,Schiff WM,Klatt E,Lieskovsky G,Skinner DG. The potency-sparing radical cystectomy:does it compromise the completeness of the cancer resection?J Urol 1988;140: 1400-3.
[8]Colombo R,Pellucchi F,Moschini M,Gallina A,Bertini R, Salonia A,et al.Fifteen-year single-centre experience with three different surgical procedures of nerve-sparing cystectomy in selected organ-confined bladder cancer patients. World J Urol 2015;33:1389-95.
[9]Haberman K,Wittig K,Yuh B,Ruel N,Lau C,Wilson TG,et al. The effect of nerve-sparing robot-assisted radical cystoprostatectomy on erectile function in a preoperatively potent population.J Endourol Endourol Soc 2014;28:1352-6.
[10]Hekal IA,El-Bahnasawy MS,Mosbah A,El-Assmy A,Shaaban A. Recoverability of erectile function in post-radical cystectomy patients:subjective and objective evaluations.Eur Urol 2009; 55:275-83.
[11]Walsh PC,Donker PJ.Impotence following radical prostatectomy:insight into etiology and prevention.J Urol 1982;128: 492-7.
[12]Walsh PC,Lepor H,Eggleston JC.Radical prostatectomy with preservation of sexual function:anatomical and pathological considerations.Prostate 1983;4:473-85.
[13]Costello AJ,Brooks M,Cole OJ.Anatomical studies of the neurovascular bundle and cavernosal nerves.BJU Int 2004;94:1071-6.
[14]Takenaka A,Leung RA,Fujisawa M,Tewari AK.Anatomy of autonomic nerve component in the male pelvis:the new concept from a perspective for robotic nerve sparing radical prostatectomy.World J Urol 2006;24:136-43.
[15]Lunacek A,Schwentner C,Fritsch H,Bartsch G,Strasser H. Anatomical radical retropubic prostatectomy: ‘curtain dissection’of the neurovascular bundle.BJU Int 2005;95: 1226-31.
[16]Collins JW,Tyritzis S,Nyberg T,Schumacher M,Laurin O, Khazaeli D,et al.Robot-assisted radical cystectomy: description of an evolved approach to radical cystectomy.Eur Urol 2013;64:654-63.
[17]Walz J,Epstein JI,Ganzer R,Graefen M,Guazzoni G,Kaouk J, et al.A critical analysis of the current knowledge of surgical anatomy of the prostate related to optimisation of cancer control and preservation of continence and erection in candidates for radical prostatectomy:an update.Eur Urol 2016 Feb 2.pii:S0302-2838(16)00128-7.
[18]Schlegel PN,Walsh PC.Neuroanatomical approach to radical cystoprostatectomy with preservation of sexual function.J Urol 1987;138:1402-6.
[19]Canda AE,Atmaca AF,Altinova S,Akbulut Z,Balbay MD. Robot-assisted nerve-sparing radical cystectomy with bilateral extended pelvic lymph node dissection(PLND)and intracorporeal urinary diversion for bladder cancer:initial experience in 27 cases.BJU Int 2012;110:434-44.
[20]Colombo R,BertiniR,Salonia A,Naspro R,GhezziM,MazzoccoliB, et al.Overall clinical outcomes after nerve and seminal sparing radical cystectomy for the treatment of organ confined bladder cancer.J Urol 2004;171:1819-22.discussion 22.
[21]Jacobs BL,Daignault S,Lee CT,Hafez KS,Montgomery JS, Montie JE,et al.Prostate capsule sparing versus nerve sparing radical cystectomy for bladder cancer:results of a randomized,controlled trial.J Urol 2015;193:64-70.
[22]Puppo P,Introini C,Bertolotto F,Naselli A.Potency preserving cystectomy with intrafascial prostatectomy for high risk superficial bladder cancer.J Urol 2008;179:1727-32.discussion 32.
[23]Ong CH,Schmitt M,Thalmann GN,Studer UE.Individualized seminal vesicle sparing cystoprostatectomy combined with ileal orthotopic bladder substitution achieves good functional results.J Urol 2010;183:1337-41.
[24]Bi L,Huang H,Fan X,Li K,Xu K,Jiang C,et al.Extended vs non-extended pelvic lymph node dissection and their in fluence on recurrence-free survival in patients undergoing radical cystectomy for bladder cancer:a systematic reviewand meta-analysis of comparative studies.BJU Int 2014;113: E39-48.
[25]Zehnder P,Studer UE,Skinner EC,Dorin RP,Cai J,Roth B, et al.Super extended versus extended pelvic lymph node dissection in patients undergoing radical cystectomy for bladder cancer:a comparative study.J Urol 2011;186: 1261-8.
[26]Walz J,Burnett AL,Costello AJ,Eastham JA,Graefen M, Guillonneau B,et al.A critical analysis of the current knowledge of surgical anatomy related to optimization of cancer control and preservation of continence and erection in candidates for radical prostatectomy.Eur Urol 2010;57: 179-92.
[27]Schoenberg MP,Walsh PC,Breazeale DR,Marshall FF, Mostwin JL,Brendler CB.Local recurrence and survival following nerve sparing radical cystoprostatectomy for bladder cancer:10-year follow-up.J Urol 1996;155:490-4.
[28]Kessler TM,Burkhard FC,Studer UE.Clinical indications and outcomes with nerve-sparing cystectomy in patients with bladder cancer.Urol Clin N Am 2005;32:165-75.
Received 5 April 2016;received in revised form 28 April 2016;accepted 28 April 2016 Available online 27 May 2016
*Corresponding author.
E-mail address:urolhj@sina.com(J.Huang).
Peer review under responsibility of Second Military Medical University.
http://dx.doi.org/10.1016/j.ajur.2016.04.004
2214-3882/?2016 Editorial Office of Asian Journal of Urology.Production and hosting by Elsevier B.V.Ltd.This is an open access article under the CC BY-NC-ND license(http://creativecommons.org/licenses/by-nc-nd/4.0/).
 Asian Journal of Urology2016年3期
Asian Journal of Urology2016年3期
- Asian Journal of Urology的其它文章
- Robot-assisted laparoscopic radical cystectomy with complete intracorporeal urinary diversion
- Stents for malignant ureteral obstruction
- Percutaneous resection of upper tract urothelial cell carcinoma:When,how, and is it safe?
- Techniques to resect the distal ureter in robotic/laparoscopic nephroureterectomy
- Thulium laser treatment for bladder cancer
- Narrow band imaging for bladder cancer