
Clinical Treatment and Anatomy Study of Maxillary First Molars with Five Root Canals
2011-11-22 02:36:04KuoWanShunyunLuoJizhiZhaoHaiyunWangLinMaandWendongYang
Chinese Medical Sciences Journal 2011年2期
Kuo Wan,Shun-yun Luo,Ji-zhi Zhao,Hai-yun Wang,Lin Ma,and Wen-dong Yang*
1Department of Stomatology,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences &Peking Union Medical College,Beijing 100730,China
THE purpose of root canal treatment is to thoroughly clean the root canal system and fill it in all its dimensions.1To achieve this goal,the entire root canal system must be adequately debrided and completely filled.In clinical practice,variations in the canal morphology pose a constant challenge to endodontists in deciding on accurate diagnosis and appropriate management.Knowledge of these variations is crucial for a successful endodontic treatment,especially in absence of an operating microscope or cone-beam computered tomography (CBCT).
The maxillary first molar generally has three or four canals,with one canal in each of the palatal and distobuccal(DB) roots,and the other one or two in the mesiobuccal(MB) root.Examination of the configuration of the canals located in the MB root showed that most cases had treatable second canals and lesser had two separate apical foramina,and in other cases with five canals,three of them were located in the MB root.In recent years,with the development of operating microscope and CBCT,several different morphological variations in root canals have been detected.Albuquerque et al2reported 3 cases of maxillary first molar with six root canals,two in each root.Kottoor et al3reported the endodontic management of a maxillary first molar with 7 root canals.
In the present case report,we described a permanent maxillary first molar with 5 root canals (2 MB,1 DB,and 2 palatal),in which two palatal and two MB root canals merged at the apical third,respectively.We also studied the anatomical stracture of a maxillary first molar with the similar morphology (2MB,1DB,and 2 palatal root canals),with each canal located in a distinct root.
CASE DESCRIPTION
Clinical observation and treatment
A 48-year-old Chinese male patient was referred to Department of Stomatology (Peking Union Medical College Hospital) for root canal treatment of his right maxillary first molar.The tooth was tender to percussion and the mesiopalatal cusp was missing.A fistula was detected close to the buccal gingiva of the tooth.After probing the fistula with a #15 gutta percha and X-ray check,we found that the gutta percha was connected with the mesial root of the tooth and there was a small periapical radiolucent area around mesial root and palatal root.The clinical diagnosis was chronic periapicitis.
The tooth was isolated with rubber dam and conventional coronal access was performed.After cleaning the pulp chamber,we noticed that the instrument in the palatal root appeared to be in a position more distal than normal,thus suspected the existence of an additional palatal root canal.As expected,a second palatal root canal orifice was located after careful inspection of the pulp floor.Two orifices were observed in the MB root,and one was found in the DB root (Fig.1).A manual instrument of size 10 was used for apical patency.The canal was negotiated to the working length,as indicated by an apex locator (Root ZX,J.Morita MFG Corp,Kyoto,Japan).Root canal pre-paration was performed using nickel-titanium rotary instruments(HERO642,Micro-Mega,Besancon,France) with crown-down technique.When the preparation was completed,the tooth was medicated with calcium hydroxide followed by temporization.
The patient returned asymptomatically after one week and the fistula disappeared.The root canals were repeatedly irrigated with saline and 3% sodium hypochlorite.The whole root canal system was obturated with sealer(Cortisomal,Piere Rolland,Merignac,France) and gutta percha using lateral condensation technique (Fig.2).
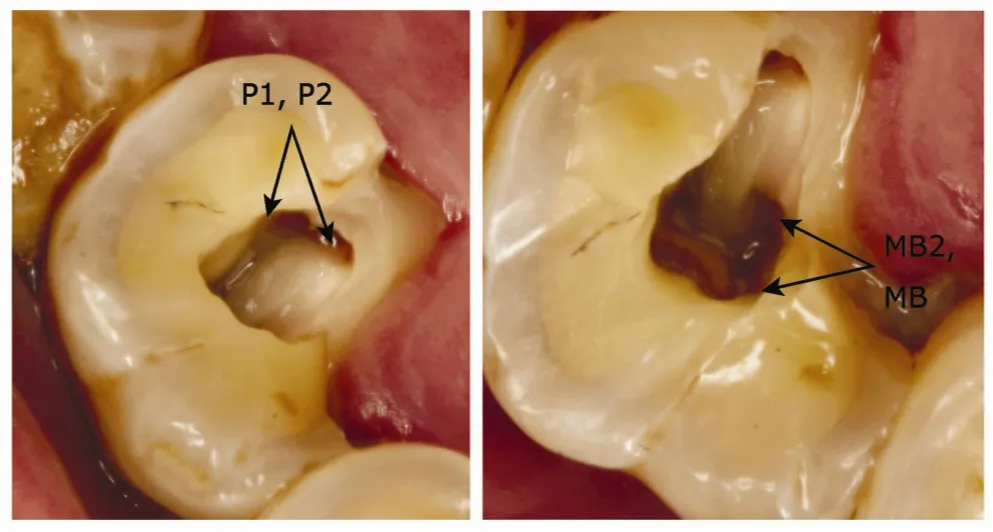
Figure 1.Occlusal view showing 2 palatal orifices (P1,P2) and 2 mesiobuccal orifices (MB,MB2) before obturation.

Figure 2.The five orifices in the pulp floor after obturation.DB:distobuccal orifice.
Anatomical study
Anatomic study was conducted with a maxillary first molar extracted from a 45-year-old Chinese female patient due to recurrent periapical infection.That tooth had five distinct roots (2 MB,1 DB,and 2 palatal).Conventional access cavities were performed and root canals were explored using FlexoFiles of sizes #15 to #30 (Dentsply Maillefer,Tulsa,OK,USA).Microscopic and radiographic features of the tooth were carefully recorded (Fig.3).It was showed that each root contained one canal;hence there were totally five canals in this molar.
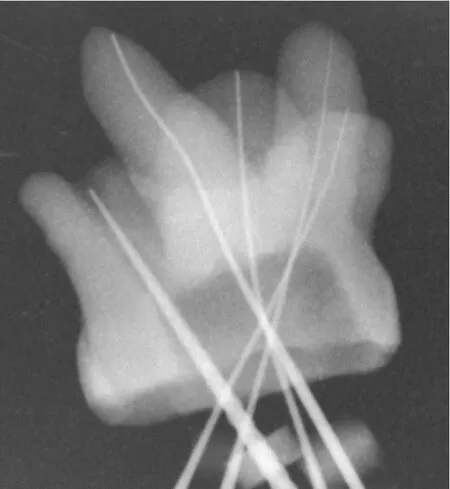
Figure 3.A maxillary first molar with five root canals demonstrated in radiography.
DISCUSSION
Most maxillary first molars have 4 canals.The second MB canal (MB2) is usually found 0.5-5 mm palatal to the main MB canal and often hidden under a cervical ledge.In most cases,the second MB canal can be located clinically by carefully exploring the pulp floor and removing a small amount of tooth structure that may occlude the canal orifice.Single palatal root canal is common,but there are also morphological variations detected.Baratto-Filho et al4reported a maxillary first molar with two palatal roots with distinct canals and foramen.Maggiore et al5reported a case of a maxillary first molar with the palatal canal trifurcating at the apical level with three separate foramina.There have also been more recent reports discussing the variations in root configuration and number of root canals of maxillary first molar.2,3,6,7
In order to avoid omitting additional root canals in maxillary first molar,several methods during examination and treatment are recommended.First,it is of crucial importance for endodontists to keep in mind different anatomic morphologies1by updating knowledge from newly published literatures and studying extracted teeth.Second,imaging techniques (e.g.dental film,CBCT)should be applied before and during treatment.Multiple angulated preoperative radiographs may be valuable in detecting abnormal structures.If endodontic files are not well centered in the canal on the radiograph,additional canals might exist.8Third,modifications to the normal access opening,removal of calcified debris,and careful examination of the pulp floor are recommended to identify additional canals.The traditional triangular access opening of maxillary first molar sometimes is limited in achieving a straight-line access and exploring all root canals of the teeth with anatomic variations.Enlarged access opening of the tooth to a trapezoidal shape is recommended so that the mesial outline can be parallel to the mesial marginal ridge.9A DG-16 endodontic probe as a path finder is useful to determine the angle at which the canals depart from the main chamber.Last,using an operating microscope with adequate illumination has also been shown to increase the chance of locating extra canals in maxillary molars.10
The reports of variations in root canal system allow us to better understand the complexity of each opened chamber.Considering that the operating microscope or CBCT are not available in most private clinics or dental departments of general hospitals in China,it is important for endodontists to be aware of unusual root canal morphologies and always be ready to closely search for additional root canals with bare eyes,which can avoid incomplete canal obturation and treatment failure.
2.Albuquerque DV,Kottoor J,Dham S,et al.Endodontic management of maxillary permanent first molar with 6 root canals:3 case reports.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:79-83.
3.Kottoor J,Velmurugan N,Sudha R,et al.Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning:a case report.J Endod 2010;36:915-21.
4.Baratto-Filho F,Fariniuk LF,Ferreira EL,et al.Clinical and macroscopic study of maxillary molars with two palatal roots.Int End J 2002;35:796-801.
5.Maggiore F,Jou YT,Kim S.A six-canal maxillary first molar:case report.Int End J 2002;35:486-91.
6.Adanir N.An unusual maxillary first molar with four roots and six canals:a case report.Aust Dent J 2007;52:333-5.
7.de Almeida-Gomes F,Maniglia-Ferreira C,Carvalho de Sousa B,et al.Six root canals in maxillary first molar.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e157-9.
8.Johal S.Unusual maxillary first molar with 2 palatal canals within a single root:a case report.J Can Dent Assoc 2001;67:211-4.
9.Aggarwal V,Singla M,Logani A,et al.Endodontic management of a maxillary first molar with two palatal canals with the aid of spiral computed tomography:a case report.J endod 2009;35:137-9.
10.G?rduysus MO,G?rduysus M,Friedman S.Operating microscope improves negotiation of second mesiobuccal canals in maxillary molars.J Endod 2001;27:683-6.
1.Cohen S,Burns RC.Pathways of the pulp.8th ed.St Louis:Mosby.2002.p.73-229,258-368.
 Chinese Medical Sciences Journal2011年2期
Chinese Medical Sciences Journal2011年2期
- Chinese Medical Sciences Journal的其它文章
- Risk Factors Analysis on Traumatic Brain Injury Prognosis
- Erythropoietin Receptor Positive Circulating Progenitor Cells and Endothelial Progenitor Cells in Patients with Different Stages of Diabetic Retinopathy△
- Inhibition of SIRT1 Increases EZH2 Protein Level and Enhances the Repression of EZH2 on Target Gene Expression△
- Immediate Surgical Intervention for Penile Fracture:a Case Report and Literature Review
- Magnetic Resonance Urography and X-ray Urography Findings of Congenital Megaureter
- Changes of Nerve Growth Factor in Amniotic Fluid and Correlation with Ventriculomegaly△