
Magnetic Resonance Urography and X-ray Urography Findings of Congenital Megaureter
2011-11-22 02:36:04TianranLiXiangkeDuandTianlongHuo
Chinese Medical Sciences Journal 2011年2期
Tian-ran Li*,Xiang-ke Du,and Tian-long Huo
Department of Radiology,Peking University People’s Hospital,Beijing 100044,China
MEGAURETER is a general concept,referring to any huge dilatation of ureter but not specific to any particular disease.1However,congenital megaureter is mainly caused by congenital abnormality and is extremely rare in clinical practice.2Preoperative imaging diagnosis is very important for determining the scope of the lesion and the relationship with surrounding structures,and distinction from other diseases.Modern medical imaging techniques,particularly magnetic resonance imaging (MRI),may directly reflect the scope and extent of disease,and facilitate differential diagnosis.3Due to the rareness of the congenital malformation in megaureter,there are few studies on its imaging characteristics,in particular,with the use of MRI technology.The main purpose of this study is to observe the imaging findings of congenital megaureter to enhance the understanding of this disease.In this process,advantages and disadvantages of conventional X-ray urography and MRI techniques were compared.
PATIENTS AND METHODS
Patients collection
A total of 7 patients were included in this study from June 2000 to December 2008.According to pathological results,5 of the 7 patients with congenital megaureter were confirmed,and the other two were found misdiagnosed in imaging.The imaging data of all the patients were collected.The major clinical symptom was abdominal pain associated with urinary tract infection in 4 cases,urinary tract calculi in 2 cases,and hematuria in 1 case.
Imaging examination method
The 7 patients underwent X-ray urography and magnetic resonance urography (MRU).Two patients were examined by X-ray retrograde pyelography (RGP),but successful only in one patient.
The equipment applied in MRU was Elscint Prestig 2.0 T superconductive magnetic resonance scanner,Elscint OmniPro workstation (Elscint LTD,Haifa,Israel).Using spin-echo sequences for coronal scout images and axial T1-weighted images (560 ms/16 ms),then fast spin-echo sequences for axial T2-weighted images (9600 ms/96 ms)and coronal heavy T2-weighted image (9600 ms/120 ms).Other parameters for imaging included:echo train length 10-14,flip angle 110°-150°,slice thickness and space 3.0 mm,field of view 24 cm×32 cm-40 cm×45 cm,matrix 192×256,number of excitations 2,scan time 4-7.5 minutes,and pre-saturation range covering four directions(upward,downward,left,and right).Finally,three-dithree-dimensional reconstruction was processed with the maximum intensity projection in the workstation,using heavy T2-weighted coronal images as the raw images,and the MRU images of the best quality were selected as the basis for diagnosis.
Intravenous pyelography (IVP) was performed with intravenous injection of 100 mL contrast agent (Iohexol 300 mgI/mL) at ulnar vein.X-ray films were taken 7 minutes,15 minutes,and 30 minutes after the injection of contrast agent.However,in two patients,the films were taken with delay (60 to 90 minutes) after agent injection.
RGP was conducted through the lower urinary tract catheter.Contrast agent (15 mL) was injected through the catheter,and X-ray films were taken simultaneously.
Pathological examination
Conventional hematoxylin-eosin staining method was adopted in the pathological test. Briefly,ureter tissues were taken half an hour after surgery,fixed in formalin for 24 hours,and embedded with paraffin.The tissues were sectioned into 4-μm slices,stained with hematoxylin for 5-10 minutes,bleached with alcohol,and stained again with eosin for 3 minutes.After washing with water and drying,the tissues were examined under microscope.
Image analysis
According to postoperative pathologic results,image data of the patients were judged as right or wrong diagnoses.
All the images of the patients were analyzed,and image characteristics of congenital megaureter were summarized by 3 radiologists blind to this study.Comparison between MRU and X-ray urography was conducted in five aspects,namely the demonstrations of lesion,kidney complication,urinary tract malformation,surrounding structure,and stone or calcification.The lesions were evaluated in terms of renal morphology and function,association with other malformations,impact on the surrounding structures,and the existence of calcification and calculi.
RESULTS
MRU findings
With conventional MR scanning sequences,the dilated ureter was hypointensive on T1-weighted images and hyperintensive on T2-weighted images.The dilated ureter was with intact wall,uniform in thickness,with no mural nodules,exhibiting hypointensity on T1-weighted images and hyperintensity on T2-weighted images (Fig.1A,B).The scanning showed dilated calices and renal pelvis,pelviureteric obstruction,and renal duplication in 3 patients.The mass was located retroperitoneal,and the surrounding structure was clearly shifted in all the patients.For instance,the kidney may appear shifted upward and outward,and the intestine shifted to the front.No infiltration to the surrounding structure was found.The retroperitoneal mass was shown in MRU as a long tubular cystic structure spreading from the kidney to the pelvis and reaching the bladder (Fig.1C,Fig.2A).The MRU images can be observed in three-dimensional rotation without background disturbance (Fig.3A,B).
X-ray urography findings
The main direct sign of megaureter in X-ray IVP was a significant dilatation of ureter in 5 patients.Compared to the direct sign,however,the indirect signs were more common,including normal renal pelvis with dilated ureter,hydronephrosis,malformation,and displacement of the urinary system.Calcifications and stones were visible on the plain films in 2 patients.In addition,congenital megaureter was found in concurrence with other urinary tract malformations,such as the double renal pelvis and ureter in 2 patients (Fig.1D,E).Because of ectopic ureter entrance with stenosis,RGP failed in one patient.The successful RGP in the other patient showed upward shifted left kidney and mild hydronephrosis.Despite the mild left renal pelvis and calyceal dilatation,the right ureter appeared normal in the image (Fig.2B,C).
Pathology results
Pathology results confirmed that 5 patients had congenital megaureter,including a patient accompanied by ureteropelvic junction stenosis,and another by ectopic ureter and ureterocyst.In the 5 patients,the lesion was on the left side in 4 cases,and on the right side in the other one.As for the remaining 2 patients originally diagnosed as congenital megaureter by imaging examination,pathology results showed no ureter epithelial tissue in the wall of the lesion,but fibrous tissue in one case and lymphatic epithelial tissue in the other,therefore confirming them as simple retroperitoneal cyst and retroperitoneal lymphangioma,respectively.
The ureter of congenital megaureter was obviously but unevenly dilated with thin wall,and the fluid in ureter was as clear as that in bladder in macropathology (Fig.3C).Pathological observations revealed that the ureteral mu cosa was mainly gray,dark red,or white,with chronic inflammatory changes,and proliferation of fibrous tissue (Fig.3D).
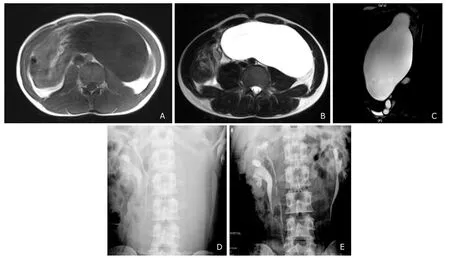
Figure 1.Megaureter with bilateral ureteropelvic duplication malformation in one patient.
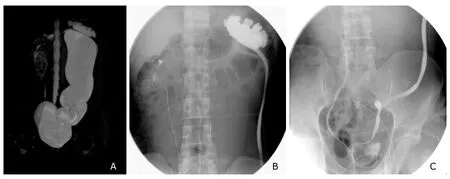
Figure 2.A retroperitoneal simple cyst misdiagnosed as megaureter.
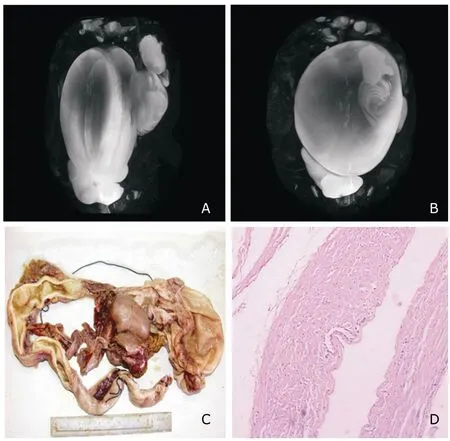
Figure 3.MRU images and pathological findings of a left megaureter of one patient.
Image analysis
Seven patients were all diagnosed as megaureter by MRU,in which two patients were misdiagnosed.Three patients were correctly diagnosed as megaureter by X-urography and four patients were diagnosed as retroperitoneal spaceoccupying lesion.
Comparison between the two techniques showed that MRU technique beat X-urography examination in four aspects,including lesion,kidney complication,urinary tract malformation,and surrounding structure.But the performance of MRU in the evaluation of stone or calcification was inferior to X-ray urography,and stone or calcification can be detected with conventional X-ray plain films before X-ray urography.
DISCUSSION
Congenital megaureter was first described in 1923 by Caulk and its characteristics were described as:no elongation,no twists,no obstruction,dynamic change,persistent infection,ureteral orifice relaxation,etc.4Mackinnon et al5and Tanagho et al6indicated that a short segment of ureter near the bladder wall retains circular muscles and lacks longitudinal muscles,which is caused by functional obstruction.It was accepted by many as the pathogenesis of megaureter.But other researcher believed that megaureter is due to the lack of ganglion in ureter caused by a variety of neuromuscular disorders.7Megaureter was divided into three categories by Pfister:refluxing megaureter;obstructive megaloureter;no-reflexing and no-obstructive megaloureter.8The first two are relatively common,while the third category is very rare.
X-urography,including IVP and RGP,is the most common examination method for urinary system diseases,and widely accepted as an effective screening and diagnostic method of the urinary system malformation.In the present study,X-urography findings in the patients are as follows:full or segmental dilatation of ureter,upper pyelocaliectasis,hydronephrosis,and kidney deformities.In addition,renal imaging delay,ureter emptying delay,and weakened peristalsis may also be demonstrated.IVP can be used to specifically identify the area of obstruction and to determine the presence of duplex collecting systems.RGP may better facilitate the determination of the stenosis site,better define the obstructing area,and document the normality of the underlying tract.1In this procedure,the valvular flaps appear convex upward.
MRI has advantages of non-invasiveness,absence of X-ray radiation,no contrast agent,no bowel preparation,and no dependence on renal function.A study showed that MRI scanning can demonstrate anatomic structure better than IVP,particularly the renal parenchyma,ectopic ureters,and poorly functioning dilated systems.9On the basis of the conventional MRI,MRU three-dimensional reconstruction method correctly depicts anatomy and allows assessment of the whole urinary tract.MR imaging is not suitable for general screening,but efficiently reveals anatomic details and enhances diagnostic specificity.7MRU can demonstrate ectopic extravesical ureteric insertions,thereby providing a global view of the malformation.10The advantages of MRU allow accurate assessment of the obstruction location in ureter deformity.MRU images can be rotated to meet the needs of diagnosis on the MR workstation.This technique can be applied in combination with conventional MRI examination for more accurate judgments,and to a certain extent compensates the deficiency of X-urography.
However,MRU also has its limitations:it is a virtual imaging technique,achieving a strong image contrast through strengthening free water MR signal.Spatial resolution of reconstructed image may thus be declined,failing to detect some small lesions,and stones can only be determined based on indirect sign because calcium shows low signal intensity.11For the cases with upper ureter dilatation but lower ureter stenosis,X-ray urography is a better imaging method than MRU.Furthermore,MRU can not distinguish vesicoureteric reflux from obstructive megaureter.12Given the advantages and efficiency of MRU,it might replace IVP for imaging of many conditions,though its clinical use is yet to be validated.
A previous study has shown that urinary tract infections were the most common complications of megaureter,13consistent with the pathological results of the present study.A study on obstructive and refluxing megaureters revealed the different pathogenesis of these two types of megaureters in human urinary tract.10The proportion of smooth muscle was significantly lower in the segments of refluxing megaureter than in those of obstructive megaureter.In addition,the number of apoptotic cells was significantly increased in obstructive megaureter compared with refluxing megaureter.14Further distinction could be identified in the future study.
The pathological findings revealed two misdiagnosed cases.One cause of misdiagnosis was the location of lesions along the running area of the normal ureter,and another reason was the similar shape of the lesions to megaureter.Third,the indirect imaging signs suggest derivation from the abnormal ureter.These reasons may cause mistaking a retroperitoneal space-occupying lesion for congenital megaureter.Combined application of different imaging techniques may help to improve the accuracy of diagnosis.
In patients with high-grade urinary tract obstruction where the contrast agent of IVP can not pass to fill the cystic lesion,multi-slice CT pyelography could be an alternative imaging technique to CT urography.It enables accurate diagnosis of the level of obstruction as well as its etiology,including urothelial tumors,primary congenital megaureter,ureteropelvic junction stenosis,ureteral stricture,retroperitoneal fibrosis,and pelvic lymphadenopathy.15Abdominal ultrasound is recommended in all children with structural abnormalities of the urinary tract.16
With respective advantages,MRU and X-ray urography techniques in congenital megaureter can complement each other and provide more detailed anatomical or functional information,which is conducive to disease diagnosis.Compared with X-ray urography,MRU can show more direct and indirect signs of the disease.The combination of the two techniques may improve the accuracy of preoperative diagnosis and better guide surgery.
1.Rosenblatt GS,Takesita K,Fuchs GJ.Urolithiasis in adults with congenital megaureter.Can Urol Assoc J 2009;3:E77-80.
2.Hodges SJ,Werle D,McLorie G,et al.Megaureter.ScientificWorldJournal 2010;10:603-12.
3.Goto H,Kanematsu A,Yoshimura K,et al.Preoperative diagnosis of congenital segmental giant megaureter presenting as a fetal abdominal mass.J Pediatr Surg 2010;45:269-71.
4.Caulk JR.Megaloureter:the importance of the ureterovesical valve.J Urol1923;9:315-9.
5.Mackinnon KJ,Foote JW,Wiglesworth FW,et al.The pathology of the adynamic distal ureteral segment.J Urol 1970;103:134-6.
6.Tanagho EA,Smith DR,Guthrie TH.Pathophysiology of functional ureteral obstruction.J Urol 1970;104:73-88.
7.Abid SS,Aslam M,Khan S,et al.Complicated megaureter with aganglionosis in an adult lady.J Coll Physicians Surg Pak 2010;20:629-30.
8.Pfister PC,Hendren WH.Primary megaureter in children and adults.Clinical and pathophysiologic features of 150 ureters.Urology 1980;12:160-76.
9.Wille S,von Knobloch R,Klose KJ,et al.Magnetic resonance urography in pediatric urology.Scand J Urol Nephrol 2003;37:16-21.
10.Kang,HJ,Lee HY,Jin MH,et al.Decreased interstitial cells of Cajal-like cells,possible cause of congenital refluxing megaureters:histopathologic differences in refluxing and obstructive megaureters.Urology 2009;74:318-23.
11.Cerwinka WH,Kirsch AJ.Magnetic resonance urography in pediatric urology.Curr Opin Urol 2010;20:323-9.
12.Goto H,Kanematsu A,Yoshimura K,et al.Preoperative diagnosis of congenital segmental giant megaureter presenting as a fetal abdominal mass.J Pediatr Surg 2010;45:269-71.
13.Gimpel C,Masioniene L,Djakovic N,et al.Complications and long-term outcome of primary obstructive megaureter in childhood.Pediatr Nephrol 2010;25:1679-86.
14.Berrocal T,López-Pereira P,Arjonilla A,et al.Anomalies of the distal ureter,bladder,and urethra in children:embryologic,radiologic,and pathologic features.Radiographics 2002;22:1139-64.
15.Ghersin E,Brook OR,Meretik S,et al.Antegrade MDCT pyelography for the evaluation of patients with obstructed urinary tract.AJR Am J Roentgenol 2004;183:1691-6.
16.Jothilakshmi K,Vijayaraghavan B,Paul S,et al.Radiological evaluation of the urinary tract in children with urinary infection.Indian J Pediatr 2001;68:1131-3.
 Chinese Medical Sciences Journal2011年2期
Chinese Medical Sciences Journal2011年2期
- Chinese Medical Sciences Journal的其它文章
- Risk Factors Analysis on Traumatic Brain Injury Prognosis
- Erythropoietin Receptor Positive Circulating Progenitor Cells and Endothelial Progenitor Cells in Patients with Different Stages of Diabetic Retinopathy△
- Inhibition of SIRT1 Increases EZH2 Protein Level and Enhances the Repression of EZH2 on Target Gene Expression△
- Immediate Surgical Intervention for Penile Fracture:a Case Report and Literature Review
- Clinical Treatment and Anatomy Study of Maxillary First Molars with Five Root Canals
- Changes of Nerve Growth Factor in Amniotic Fluid and Correlation with Ventriculomegaly△