
Relationship between Carotid Atherosclerosis and Cerebral Infarction
2010-11-22 02:36:32GuangwenLiGuanyiZhengJinguoLiandXudongSun
Chinese Medical Sciences Journal 2010年1期
Guang-wen Li,Guan-yi Zheng*,Jin-guo Li,and Xu-dong Sun
Department of Geriatrics,Union Hospital,Fujian Medical University,Fuzhou 350001,China
CEREBROVASCULAR diseases seriously threaten human health.Following malignant tumors,stroke is the second leading cause of death in Chinese population and one of the most important risk factors for disability.1Carotid atherosclerosis(CAS) is one of the major risk factors for cerebrovascular diseases,especially ischemic cerebrovascular diseases.The characteristics of carotid plaque are closely related to the type of ischemic cerebrovascular diseases.2,3The Asymptomatic Carotid Atherosclerosis Study (ACAS) showed that carotid endarterectomy reduced the aggregate risk over 5 years for ipsilateral ischemic stroke by 53% compared with medical therapy (aspirin) (11.0%vs.5.1%) in patients with asymptomatic carotid stenosis of 60% or greater reduction in diameter.4Therefore,to determine whether ischemic stroke patients suffer from CAS is of important clinical significance.For patients with ischemic stroke,carotid ultrasonography can measure the degree of carotid stenosis,intima-media thickness (IMT),and plaques,providing the basis for evaluating the prognosis of cerebral infarction (CI) and effect of drug treatment.5
The present study compared the severity of CAS,characteristics and location of plaques,and inner diameter of carotid arteries between CI patients and patients with non-cerebrovascular diseases based on the results of carotid color Doppler ultrasonography,with the aim of revealing the relationship between CAS and CI.
PATIENTS AND METHODS
Patients
Between November 2008 and March 2009,147 CI patients(CI group) and 48 patients with non-cerebrovascular diseases (control group) were enrolled from inpatients of Neurology Department of Union Hospital affiliated to Fujian Medical University.The CI group included 34 patients with atherosclerotic CI and 113 patients with lacunar infarction.The diagnostic criteria for CI were in accordance with the revised diagnostic criteria of 1995 Fourth National Conference for Cerebrovascular Diseases.6All cases were confirmed by cranial magnetic resonance imaging (MRI) or computed tomography (CT) scan.The exclusive criteria were:(1) patients with cerebral hemorrhage;(2) patients with cardiogenic cerebral embolism (such as atrial fibrillation and rheumatic heart disease);(3) patients with cerebral arteritis-induced CI.
Color Doppler ultrasonography
Color Doppler ultrasonic diagnostic equipment (Vivid 7,GE,USA) was applied in this study.The measurement was carried out when the condition of the CI patients was steady,roughly one week after onset of the disease.Each patient was asked to lie in the supine position in a dark room.A pillow was put under the shoulder of the patient,with his/her head extending back and towards the contralateral side.The linear array transducer with frequency of 5-10 MHz was adopted.First,the probe was placed at the cervical root,scanning along the lateral margin of sternocleidomastoid longitudinally to show the proximal,middle,and distal segments of common carotid artery (CCA),carotid bifurcation (BIF),the beginning of internal carotid artery(ICA),and the external carotid artery (ECA).Then the probe was rotated by 90° to scan along the cross section of carotid arteries.Two-dimensional ultrasound was used to observe the structure of arterial wall,morphology and location of plaques,measure the size of plaques,and determine the natures of these plaques (soft or hard).The inner diameter of CCA was measured at the site 2.0 cm proximal to the BIF,the inner diameter of ICA was measured at the site 1.0 cm distal to the BIF,and the IMT was measured at the posterior wall of CCA proximal to the bulb.The Doppler spectrum was used to measure peak velocity (maximum velocity,Vmax)and end-diastolic velocity (EDV,Vmin).Mean velocity (Vmean)and resistance index (RI) were calculated with the following formulas:Vmean=integration of flow velocity/cardiac cycle time;RI=(Vmax-Vmin)/Vmean.7
CAS severity evaluation
The IMT and carotid plaque were applied as CAS severity index.IMT is the distance between the intima-lumen interface and the media-adventitia interface,which displays as the "dual-line sign" in the two-dimensional longitudinal ultrasound image of the carotid wall,that is,two parallel hyperechogenic lines separated by a hypoechoic line.8The diagnostic criterion of thickened carotid intima was set as 1.0 mm ≤ IMT < 1.5 mm;and the diagnostic criterion of carotid plaque was:a focal structure that encroaches into the arterial lumen for at least 0.5 mm or 50% of the surrounding IMT value or demonstrates a thickness ≥ 1.5 mm at any segment of the carotid.9According to the characteristics of ultrasound echo,the carotid plaques were divided into hard plaques(displayed as hyperecho or with acoustic shadowing) and soft plaques (displayed as isoecho or hypoecho).10
Statistical analysis
The SPSS 16.0 statistical software was applied for statistical analysis.The univariate numerical data with orderly response variable was tested by Wilcoxon rank sum test;and the constitution of two independent samples was tested by fourfold tableχ2test and 2×C table χ2test.The measurement data were expressed as mean±SD,and two-samplettest was applied when two independent samples’ variances were homogenous.A value ofP<0.05 indicated significant difference.
RESULTS
Baseline characteristics
The CI group involved 83 males and 64 females,with an average age of 66.96 (range,37-91) years.The control group involved 26 males and 22 females,with an average age of 64.27 (range,40-83) years.There was no difference in gender or age between the two groups (bothP>0.05).The prevalence of hypertension was higher in the CI group than the control group (P=0.012).The prevalence of diabetes was not significantly different between the two groups (P>0.05) (Table 1).
Comparison of CAS severity between two groups
In the CI group,22 (15.0%) patients had thickened carotid intima and 89 (60.5%) had carotid plaque.In the control group,4 (8.3%) patients had thickened carotid intima and 22 (45.8%) had carotid plaque.The severity of CAS in the CI group was significantly higher than that in the control group (P=0.022) (Table 2).
Comparison of constitution of carotid plaques between two groups
There was significant difference in the constitution of carotid plaque between the two groups (χ2=10.842,P=0.001).The CI group mainly had soft plaques (61.8%),whereas the control group mainly had hard plaques(77.3%) (Table 2).
Comparison of location of carotid plaques between two groups
The first three common locations of carotid plaque in both groups were BIF,CCA,and ICA.The plaques can be single and bilateral.Among 89 cases with carotid plaques in the CI group,71 cases had plaques existed in one of the above three sites;15 cases had plaques existed in two of the three sites,and 3 cases had plaques existed in all of the three sites.The total number of plaques in the CI group was 152.Among 22 cases with carotid plaques in the control group,18 cases had plaques existed in one of the above three sites,and 4 cases had plaques existed in two of the three sites.The total number of plaques in the control group was 39.There was no significant difference in the location of carotid plaques between the two groups (P=0.438) (Table 2).
Comparison of inner diameters and resistance indices of carotid arteries between two groups
The inner diameters of CCA and ICA were not significantly different between two groups (allP>0.05).Meanwhile,the resistance indices of CCA and ICA were not significantly different between two groups (allP>0.05) (Table 3).

Table 1.Comparison of baseline characteristics between CI group and control group
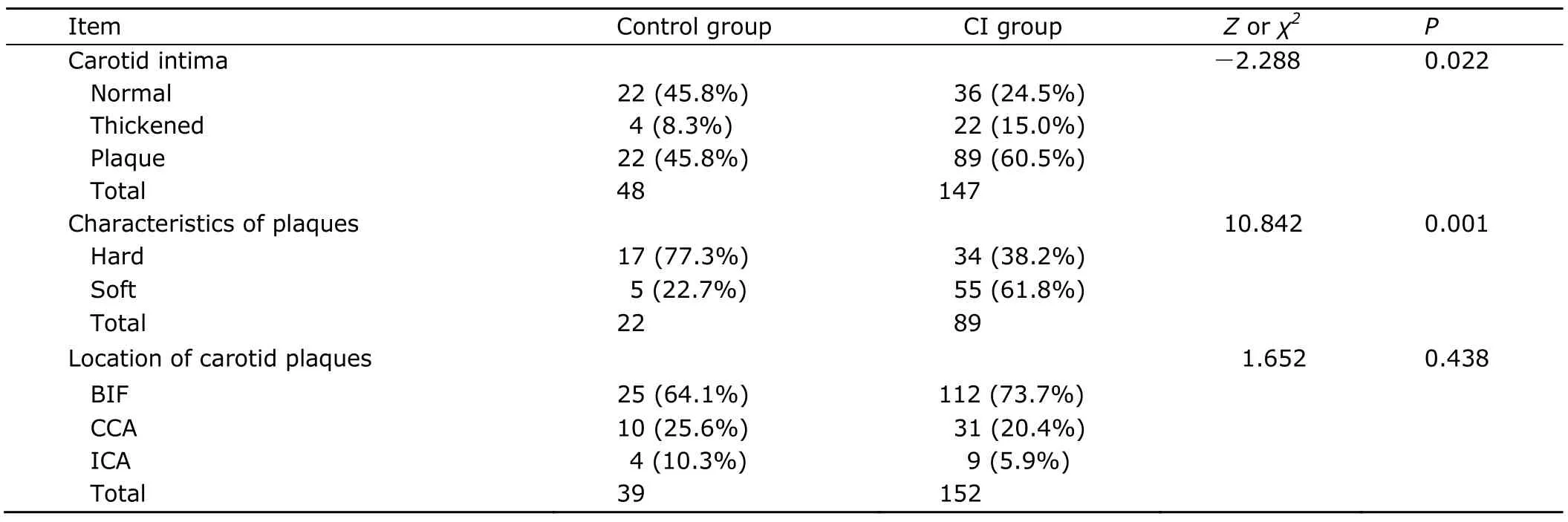
Table 2.Comparison of CAS severity,constitution of carotid plaques,and location of carotid plaques between CI group and control group
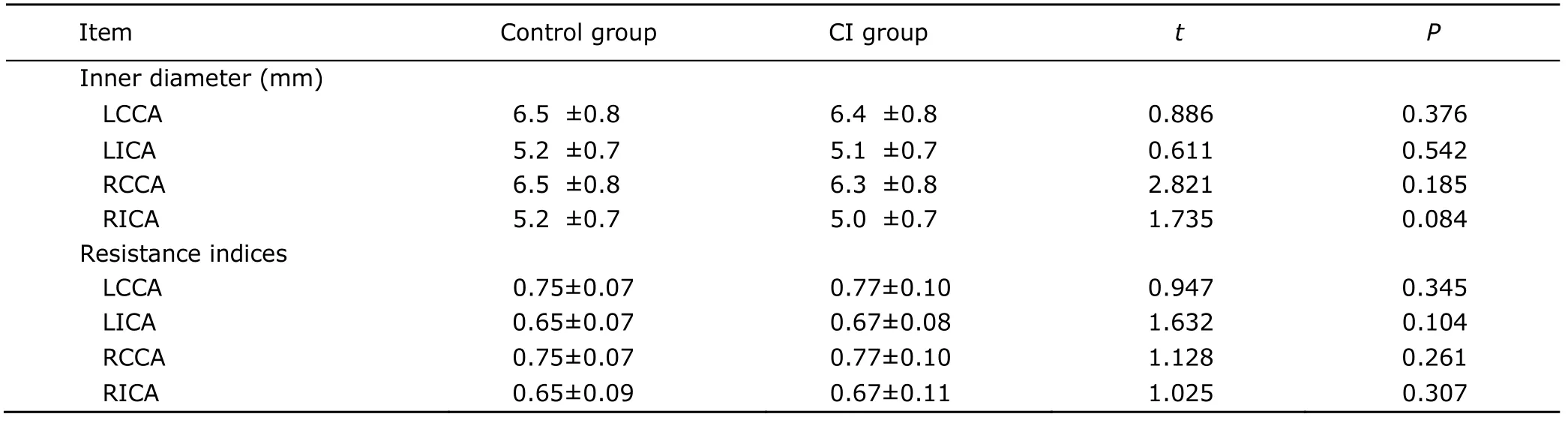
Table 3.Comparison of inner diameters and resistance indices of carotid arteries between CI group and control group
DISCUSSION
CI,mainly caused by cerebral atherosclerosis,is common in the elderly.Therefore,more and more attention should be paid to the diagnosis and treatment of atherosclerotic CI.However,the condition of cerebral atherosclerosis is hard to obtain due to the location of the cerebral arteries.Thus,it is important to find an indicator of the condition of cerebral atherosclerosis.This study showed that the CAS severity of the CI group was significantly higher than the control group,suggesting that as part of systemic atherosclerosis,CAS could be an indicator that reflects the condition of cerebral atherosclerosis.Nagai et al11reported that the sensitivity and specificity of carotid plaque predicting the cardio-and cerebrovascular diseases was 84% and 79%,respectively.Therefore,the diagnosis of CAS in clinic is attracting more and more attention.
Atherosclerosis is the important pathological basis of cardio-and cerebrovascular diseases,and it takes a few decades from atherosclerosis genesis to cardio-and cerebrovascular diseases occurrence.In fact,the pathological changes may begin from adolescence or even childhood,but the clinical symptoms only manifest in the elderly.The present study also showed that different degrees of CAS existed in both the CI group and the control group.
About 70%-85% of blood in cerebral circulation is supplied by carotid arteries.The CAS can also lead to CI directly because the carotid artery is one of the upstream of the cerebral arteries.However,it was reported that only about 10% of all CI directly result from CAS.12CAS results in CI through the following mechanisms:(1) the atherosclerotic plaque enlarges and obstructs the carotid directly;(2) the embolus coming from the ulceration or rupture of plaque results in embolization of the distal arteries;8(3)the thrombus formed by the coagulation factors and platelet activation on the rough surface of the plaques blocks the carotid.13
The study found that the CI group mainly had the soft plaques (61.8%),whereas the control group mainly had the hard plaques (77.3%).There was significant difference between the two groups in the constitution of carotid plaque (P=0.001).It is generally believed that arterial stenosis of <50% reduction in diameter will not cause significant hemodynamic abnormity.In recent years,some study found that significantly narrow lumen resulting from carotid plaque is not common.Zhang et al14reported that carotid stenosis of >50% reduction in diameter with hemodynamic significance existed in only 13.5% of CI patients,while the prevalence of carotid plaque was 81.2%.Therefore,CI was correlated not only with carotid lumen stenosis,but also with the characteristic of carotid plaque more closely.15The hypoechoic soft plaque,containing more lipids with loose texture,is vulnerable to the hemodynamic effects and is likely to rupture,shed,hemorrhage,and form the thrombus,therefore is the main cause of CI.Whereas the hyperechoic hard plaque,constituted mainly by fibrous tissue,has more stability due to the surface calcification and it is not prone to broke or drop,therefore having less relation to CI.16
The present study found that the first three common locations of carotid plaque in the CI group and the control group were BIF (73.68%;64.10%),CCA (20.39%,25.64%),and ICA (5.92%;10.26%),with no difference between the two groups.It was consistent with Hayashi et al’s report17that carotid plaque was mostly seen at BIF,followed by the CCA trunk and the original segment of ICA.This might be related to hemodynamics.The fundamental research has confirmed that when blood flows into the anatomical expansion areas,such as carotid BIF,or when the surface is not smooth,turbulence would form.Because of the pressure increase in the center of the turbulence,the erythrocyte is prone to be injured,releasing out procoagulant substances such as adenosine diphosphate (ADP) to promote platelet aggregation and coagulation,forming micro-thrombosis which organizes as plaque eventually.In addition,the high-frequency oscillation of turbulent flow slows the blood velocity,increases the local shear stress,injures the endothelial cells,and gradually develops into atherosclerotic plaque.
The present study showed that the inner diameters of CCA and ICA of the CI group were slightly smaller than the control group,but the differences were not statistically significant.It was consistent with Fang et al’s study,18in which no difference was found in the inner diameters of carotid arteries between the CAS group and the control group.In that study,there were only 3 cases with at least one carotid stenosis≥50%;17 cases with at least one stenosis≥20%;most cases showed only carotid plaque formation but no significant stenosis.The carotid stenosis of the CI group in the present study may be similar to that.Turkenburg et al19reported that after the first onset of symptoms,12%-13% of the patients with severe carotid stenosis bore the risk of complete stroke in one day and up to 30%-35% in five days.Handa et al20held the view that the risk of recurrence of CI in patients with severe carotid stenosis was 21 folds higher than patients without carotid stenosis.The results of multi-center prospective studies showed that carotid endarterectomy at an early stage could significantly reduce the risk of the occurrence and recurrence of CI in patients with serious CAS and stenosis.21
Bradshaw et al22found that about 5%-7% of females and 7%-10% of males have carotid stenosis > 50% in a population older than 65 years.CAS from intima thickens to plaque formation or even lumen stenosis,and the blood flow velocity increases,accompanied by the remodeling of atherosclerotic arteries.At the early stage of atherosclerosis,the artery expands outwards compensatorily when vessel wall thickens in order to maintain the inner diameter,which is called the“positive remodeling”.When the lesion develops,the artery can no longer expand compensatorily and the plaque encroaches into the lumen resulting in lumen stenosis or even occlusion,this is called the“negative remodeling”.23This was consistent with the conclusion drawn by Glagov et al24that the expansion of artery was a kind of vascular remodeling adapting to the progress of atherosclerosis,rather than a degenerative change with increasing age.Glagovs et al24found in the study on the relationship between lumen area and plaque area in coronary atherosclerosis that the lumen area did not decrease in relation to the percentage of stenosis (lesion area/internal elastic lamina area) for values between zero and 40 percent but did diminish markedly and was in close relation to the percentage of stenosis for values above 40 percent.
The results of our study also showed that the resistance indices of CCA and ICA of the CI group were slightly larger than the control group,but the difference was not statistically significant.This was also consistent with the results of the study by Fang et al.18According to the formula of resistance index:RI=(Vmax-Vmin)/Vmean,RI was correlated with the blood flow velocity,and the blood flow velocity was correlated with the stenosis degree.The narrower the lumen,the greater the blood flow velocity,but the flow velocity would increase significantly only when the lumen narrowed severely,and resulting in significant RI increase.25However,in the present study,severe carotid stenosis in the CI group was scarce,and the case number (48) in the control group was small,so it could not reveal difference between the two groups.
There were some limitations in this study that needed to be pointed out.Firstly,the measurement depended on the subjects’ consciousness greatly,therefore the measurement data varied greater among different measuring times than an auto-measuring software could have achieved.Secondly,in view of the safety of the CI patients,the measurement was carried out when the condition of the patients was steady,roughly one week after the onset of the disease,therefore the lesion state at the measurement might be different from the state at the onset of the disease.
The imaging techniques of carotid arteries,including digital substraction angiography (DSA),computed tomography angiography (CTA),and magnetic resonance angiography (MRA),all have limitations.They may be traumatic,expensive,or have contraindications and complications.The carotid color Doppler ultrasound imaging,however,is low-cost,non-invasive,and has significant diagnostic value.It can show the structure of carotid wall clearly,detect the atherosclerotic plaques and thrombi,identify soft plaque and hard plaque,and determine the degree of carotid stenosis accurately,thus it has important clinical significance for understanding the condition of cerebral atherosclerotic lesions and predicting the occurrence and recurrence of CI.
1.Xu YG,Zhou DB.The carotid disease and ischemic stroke.Chin J Neurosurg,2003;19:238-40.
2.Iannuzzi A,Wilcosky T,Mercuri M,et al.Ultrasonographic correlates of carotid atherosclerosis in transient ischemic attack and stroke.Stroke 1995;26:614-9.
3.Nagai Y,Kitagawa K,Sakaguchi M,et al.Significance of earlier carotid atherosclerosis for stroke subtypes.Stroke 2001;32:1780-5.
4.Executive Committee for the Asymptomatic Carotid Atherosclerosis Study.Endarterectomy for asymptomatic carotid artery stenosis.JAMA 1995;73:1421-8.
5.Pauletto P,Palatini P,Da Ros S,et al.Factors underlying the increase in carotid intima-media thickness in borderline hypertensives.Arterioscler Thromb Vasc Biol 1999;19:1231-7.
6.The Chinese Society for Neuroscience,Chinese Neurosurgical Society.The diagonostic essentials of cerebrovascular diseases.Chin J Neuro 1996;29:379-80.
7.Zhou YC,Guo WX,editors.Ultrasound Medicine.4th ed.Beijing:Scientific and Technical Documents Publishing House;2003.p.792-805.
8.Inoue K,Matsumoto M,Shono T,et al.Increased intima media thickness and atherosclerotic plaques in the carotid artery as risk factors for silent brain infarcts.J Stroke Cerebrovasc Dis 2007;16:14-20.
9.Touboul PJ,Hennerici MG,Meairs S,et al.Mannheim intima-media thickness consensus.Cerebrovasc Dis 2004;18:346-9.
10.Gr?nholdt ML.Ultrasound and lipoproteins as predictors of lipid-rich,rupture-prone plaques in the carotid artery.Arterioscler Thromb Vasc Biol 1999;19:2-13.
11.Nagai Y,Kitagawa K,Sakaguchi M,et al.Significance of earlier carotid atherosclerosis for stroke subtypes.Stroke 2001;32:1780-5.
12.Fauci AS,Braunwald E,Kasper DL,editors.Harrison's Principles of Internal Medicine.16th ed.New York:McGraw-Hill Companies,Inc;2005.p.2377.
13.Zhou J,Fang X,Lu XP,et al.The carotid atherosclerosis and cerebral infarction.J Apoplexy Nerv Dis 2004;21:275.
14.Zhang CG,Zhang HQ,Xie J,et al.Relationship between carotid atherosclerosis and ischemic cerebrovascular disease.Chin J Neurol 2006;39:832-5.
15.Wang X,Lu LH,Zhou JF,et al.The diagnostic value of color Doppler sonography of carotid atherosclerosis plaque in patient with cerebral stroke.Chin J Ultrasound Med 2000;9:685.
16.He YS,Li P.Preliminary study on the correlation between carotid atherosclerosis and cerebral infarction.J Tongji Med Univ 2003;24:43-5.
17.Hayashi K,Kitagawa N,Takahata H,et al.Endovascular treatment for cervical carotid artery stenosis presenting with progressing stroke:three case reports.Surg Neurol 2002;58:148-54.
18.Fang P,Zhou QC,Shu H,et al.Use of ultrasonography to evaluate carotid atherosclerosis and hemodynamics.Hunan Yi Ke Da Xue Xue Bao 1999;24:354-6.
19.Turkenburg JI,Otayen JA,Olen WI.Role of carotid sonography as a first examination in the evaluation of patients with transient ischemia attacks and strokes:benefit in relation to age.J Clin Ultrasound 1999;27:65-9.
20.Handa N,Matsumoto M,Maeda H,et al.Ischemic stroke events and carotid atherosclerosis.Results of the Osaka follow-up study for ultrasonographic assessment of carotid atherosclerosis (the OSACA Study).Stroke 1995;26:1781-6.
21.Yan PJ,Liu JX,Niu LC,et al.The relationship between carotid arteriostenosis and cerebral infarction.Stroke Nerv Dis 2006;13:23-4.
22.Bradshaw PJ,Wilkes ET,Thompson PL.Determinants of carotid intima-medial thickness in an urban Australian aboriginal population.Atherosclerosis 2007;192:218-23.
23.Benedetto FA,Tripepi G,Mallamaci F,et al.Rate of atherosclerotic plaque formation predicts cardiovascular events in ESRD.J Am Soc Nephrol 2008;19:757-63.
24.Glagov S,Weisenbery E,Zarins CK,et al.Compensatory enlargement of human atherosclerotic coronary arteries.N Eng J Med 1987;316:1371-5.
25.Hallerstam S,Rosfors S.Blood flow and flow resistance in the vertebral arteries of patients with and without carotid atherosclerosis.Clin Physiol Funct Imaging 2004;24:96-102.
 Chinese Medical Sciences Journal2010年1期
Chinese Medical Sciences Journal2010年1期
- Chinese Medical Sciences Journal的其它文章
- Sex Hormones and Androgen Receptor:Risk Factors of Coronary Heart Disease in Elderly Men△
- Comparison between Ophthalmologists and Community Health Workers in Screening of Shallow Anterior Chamber with Oblique Flashlight Test△
- Factors Influencing Pleural Effusion after Fontan Operation:an Analysis with 95 Patients
- Expression of FLICE-inhibitory Protein in Synovial Tissue and Its Association with Synovial Inflammation in Juvenile Idiopathic Arthritis△
- A Case of Large“Silent”Extra-adrenal Retroperitoneal Paraganglioma Resected Laparoscopically
- Revascularization for Iliac-femoral Artery Pseudoaneurysm with Greater Saphenous Vein