
Effects of a closed-loop system against SARS-CoV-2 at the Beijing 2022 Olympic Winter Games: a descriptive and modeling study
2023-11-27 10:51RongXiongJiepingZhouWenningLiJieLiuJingLouSijiaTianHuixinLianShengmeiNiuLuxiZhangWenhangLiJinjunZhang
Rong Xiong, Jieping Zhou, Wenning Li, Jie Liu, Jing Lou, Sijia Tian, Huixin Lian, Shengmei Niu, Luxi Zhang,Wenhang Li, Jinjun Zhang
1Emergence Medical Service Group for Beijing 2022 Winter Olympic Games, Beijing Emergency Medical Center, Beijing 100031, China
2Department of Neurology, Beijing Fuxing Hospital, Capital Medical University, Beijing 100038, China
3Aerospace Information Research Institute, Chinese Academy of Sciences, Beijing 100094, China
4Department of General Surgery, Beijing Tongren Hospital, Capital Medical University, Beijing 100730, China
5Games Services Department, Beijing Organizing Committee for the 2022 Olympic and Paralympic Winter Games
KEYWORDS: Olympic Winter Games; Emergency medical service; SARS-CoV-2; COVID-19;Infectious disease; Transmission
INTRODUCTION
During the COVID-19 pandemic, many international sporting events had to be postponed or canceled.[1]Despite the “bubble scheme” adopted in the 2020 Tokyo Olympic Games, 186,448 Tokyo residents became infected with SARS-CoV-2.[2]In the Euro 2020 championships, 2,472 participant infections were reported across seven host countries.[3]These statistics indicate that mass gatherings may facilitate or amplify viral infections to some extent.[2,4]Therefore, hosting the Olympics under the dynamic zero-COVID policy in China and implementing strategies to tackle both imported and domestic infections was a challenge for Beijing.Practical and scientific solutions are urgently required to allow sporting events to proceed safely and successfully during the ongoing COVID-19 pandemic.
The Beijing 2022 Olympic Winter Games(BOWG) was the first international sporting event held as scheduled since the onset of the COVID-19 pandemic, with the admission of accredited spectators into venues from February 4 to 20, 2022.More than 70,000 participants attended the events, including 13,690 foreign participants and 2,897 athletes from 91 national Olympic committees.The core risk mitigation strategy in the BOWG was a “closed-loop” system,[5]which was designed to keep the participants and residents of host cities relatively separate, thus to minimize the risk of SARS-CoV-2 transmission.[6]Within the closed-loop system, all participants were subject to daily health monitoring and polymerase chain reaction (PCR)testing and were allowed to move between permitted destinations in dedicated Games transport.Chinese personnel entering the closed-loop system had to be vaccinated and needed to isolate for 14 d prior to entry.In addition, daily PCR testing, social distancing, strict hygiene, and mask-wearing were mandatory for all participants in this system.
The aim of this study was to describe the characteristics of SARS-CoV-2-positive participants and evaluate the efficacy of a closed-loop system during the BOWG.A modified susceptibility-exposed-infectiousremove (SEIR) model, which is one of the most popular mathematical models of infection that can be used to evaluate the efficacy of various control measures, was set up to simulate the COVID-19 epidemic situation in Beijing (outside the closed-loop systems of the BOWG)during the period of the BOWG.We quantitatively evaluated the control measures implemented during the BOWG, providing a reference for mitigating infectious disease-related health risks at sporting events in the future.
METHODS
Study design
We retrospectively analyzed all SARS-CoV-2-positive BOWG participants who were transported by emergency medical service (EMS) from January 1, 2022,to February 20, 2022 in the BOWG.All SARS-CoV-2-positive cases were confirmed by PCR results, and then transported to dedicated isolation hotels or designated hospitals by the EMS.The study was approved by the Ethics Committee of the Beijing Emergency Medical Center (No.2022-4-003) and the requirement for written informed consent was waived because the transport by EMS was conducted as the mass event.
Data collection
The data were collected using an electronic medical record system by EMS staff of the BOWG.The form,designed by the Beijing Emergency Medical Center,included demographic information, epidemiological characteristics, entry information, vaccination data,laboratory test results for SARS-CoV-2, and disease severity.Two reviewers extracted the data and evaluated the eligibility of the original data independently.
The data were sourced from the BOWG based on the case and epidemiologic investigation data released by the Center for Disease Control and Prevention (CDC)of China, and the local epidemic transmission process in Beijing was reproduced during the BOWG (Figure 1).SARS-CoV-2-positive participants from other areas, or patients infected via contaminated packaging of imported products were considered to be cases that might initiate a COVID-19 epidemic.According to the COVID-19 local prevention and control measures in Beijing, patients were isolated in response to a positive PCR test at the hospital or after undergoing nucleic acid screening.Epidemiologic investigations were conducted based on SARS-CoV-2-positive cases, and some relevant close contacts and spatiotemporal interactions were quarantined.
Statistical analysis
Continuous variables were expressed as the means and standard deviations.Categorical variables were presented as counts and percentages.Differences of the categorical variables between imported and indigenous cases were assessed using the Chi-square test.All statistical analyses were performed using SPSS software version 22.0 (IBM, USA).P<0.05 was considered statistically significant.
Simulation models
The SEIR model is one of the common infectious disease models suitable for those with a certain period of latency.The standard SEIR epidemiological model has four components: susceptible, exposed, infected and removed (including recovery and death).‘Susceptible’refers to people who are not infected but can easily become infected after contact with an infected person.‘Exposed’ refers to asymptomatic people carrying the virus.‘Infected’ refers to obviously sick people.‘Removed’ refers to people who have recovered or died and are thus no longer involved in the infection process.In this paper, the SEIR model is modified in light of the known propagation characteristics of COVID-19 and government interventions during the BOWG.
The model (Figure 2) classified SARS-CoV-2-positive cases into three groups: imported infectious cases (I0), infectious cases (I), and quarantined infectious cases (IQ).Imported infectious cases refer to participants infected with SARS-CoV-2 from other areas or patients infected via contaminated packaging of imported products; infectious cases refer to infectious participants who were free to move outside of the closed-loop system of the BOWG in Beijing; and quarantined infectious cases refer to those who had a positive PCR test and were quarantined.Exposed (E) refers to patients in the incubation period including quarantined exposed persons who were isolated (EQ) as a result of the epidemiological investigation of associated COVID-19 patients.
The model parameters were set as follows: the susceptible population was set to 21.886 million people based on Beijing’s permanent population at the end of 2021.The total number of imported SARS-CoV-2-positive cases was 10 during the BOWG, comprising two sources (international mail and imported cold-chain products).These two outbreaks were caused by the VOC/Omicron strain (BA.1 evolutionary branch) and the Delta strain (AY.30 evolutionary branch).The data included the dates of diagnosis, which were derived from case data and gene traceability data released by the Beijing CDC.Additionally, Beijing adopted suitable epidemic prevention measures, such as compulsory mask-wearing indoors and in public places, so the infection rate was set at 0.3, the number of daily contacts was 6, and the incubation period was 3 d.Supplemental file displays the equations and parameters of this modified SEIR model.

Figure 1.Daily new confirmed SARS-CoV-2 positive cases during the Beijing 2022 Olympic Winter Games (BOWG).A total of 280 SARSCoV-2 positive cases within the closed-loop were enrolled in this study from January 1, 2022, to February 20, 2022, while 108 residents affected SARS-CoV-2 were detected in Beijing community.
RESULTS
Situation on the epidemic in Beijing during BOWG
A total of 280 SARS-CoV-2-positive participants transferred by Beijing EMS from January 1, 2022, to February 20, 2022, were enrolled in this study.Ninetythree (33.2%) cases were discovered by initial screening,and the others were identified by daily testing in the closed-loop system (Table 1).The median age of these cases was 37 years old (range: 29–47), and 207 cases(73.9%) were male.The positive cases originated from 47 countries and 4 continents.The majority cases included broadcasters, followed by athletes, team officials and so on.The vaccination rate among SARSCoV-2-positive cases was 93.5%, 96.4% cases were asymptomatic, while 10 cases showed mild COVID-19 symptoms.
The diagnostic time interval for all cases was reviewed and revealed that 274 (97.9%) cases were imported (i.e.,discovered within the first 14 d in the closed-loop system),while only 6 (2.1%) cases were infected in the loop (Figure 3).These results were significantly different from those reported for the 2020 Tokyo Olympic Games (55.9%within the 14-day quarantine and 44.1% after the 14-dayquarantine) (Z=11.67,P<0.0001).[2]The cases confirmed by initial screening and daily screening in the closedloop system within 14 d were regarded as imported infectious cases (I0).[9]

Table 1.Characteristics of the SARS-CoV-2-positive cases during the Beijing 2022 Olympic Winter Games
Most Olympic Games-related SARS-CoV-2 cases were identified before February 4, when the Games officially took place, and the number of cases fell rapidly after that time.In the local community outside of the closed-loop system, a new COVID-19 outbreak began on January 15 and ended on February 7.None of the 108 residents affected had interacted with personnel inside of the closed-loop system, and most confirmed cases were related to a cold storage business of imported aquatic products.[8]
Simulation of closed-loop or semi-closed-loop
conditions in Beijing
The simulation results of the closed-loop COVID-19 model for the BOWG determined using AnyLogic 8.7 University software are illustrated in Figure 2.This model was set up based on quarantine measures being implemented after 3 d, the fitted quarantine parameters were 88.5%, and the quarantine parameters reached 100% after 9 d.The simulation results of the local COVID-19 model in Beijing outside of the closed-loop system are displayed in Figure 4 and were consistent with the real data, and the R2value for the case data and simulation data is 0.997.The final cumulative number of confirmed cases was 108, and the simulation results depicted no widespread transmission of the virus as a result of the prevention and control measures in Beijing.
Assuming that the BOWG followed a semiclosed-loop management, similar to that of the Tokyo Olympic Games, and people in the original closedloop could enter downtown Beijing, then COVID-19-positive cases inside the loop may have transmitted the virus outside of the closed-loop system in Beijing.The scenario simulation results of the semi-closed-loop are presented in Figure 5, showing a cumulative number of confirmed cases of 1,137 for quick quarantine measures implemented 3 d later (1 d for confirmation PCR testing, 1 d for epidemiologic investigation, and 1 d for quarantine measures) and 5,530 for delayed quarantine measures implemented 9 d later (weekly PCR testing for persons in key positions in early 2022 may cause a 6-day delay).
DISCUSSION
This study describes the characteristics of 280 SARS-CoV-2-positive cases transported by the EMS during the BOWG.The majority of cases were imported,originating from four continents, with a similar distribution to the local spread of SARS-CoV-2.Europe was the continent that contributed most to the number of SARS-CoV-2-positive cases globally.[1]Personnel distribution analysis demonstrated that broadcasters accounted for the most positive cases, followed by athletes, and team officials, etc.Furthermore, most positive cases were vaccinated and asymptomatic.According to the epidemiological survey, there was no evidence to indicate cross-transmission between Beijing residents and participants inside of the closed-loop system during the BOWG.
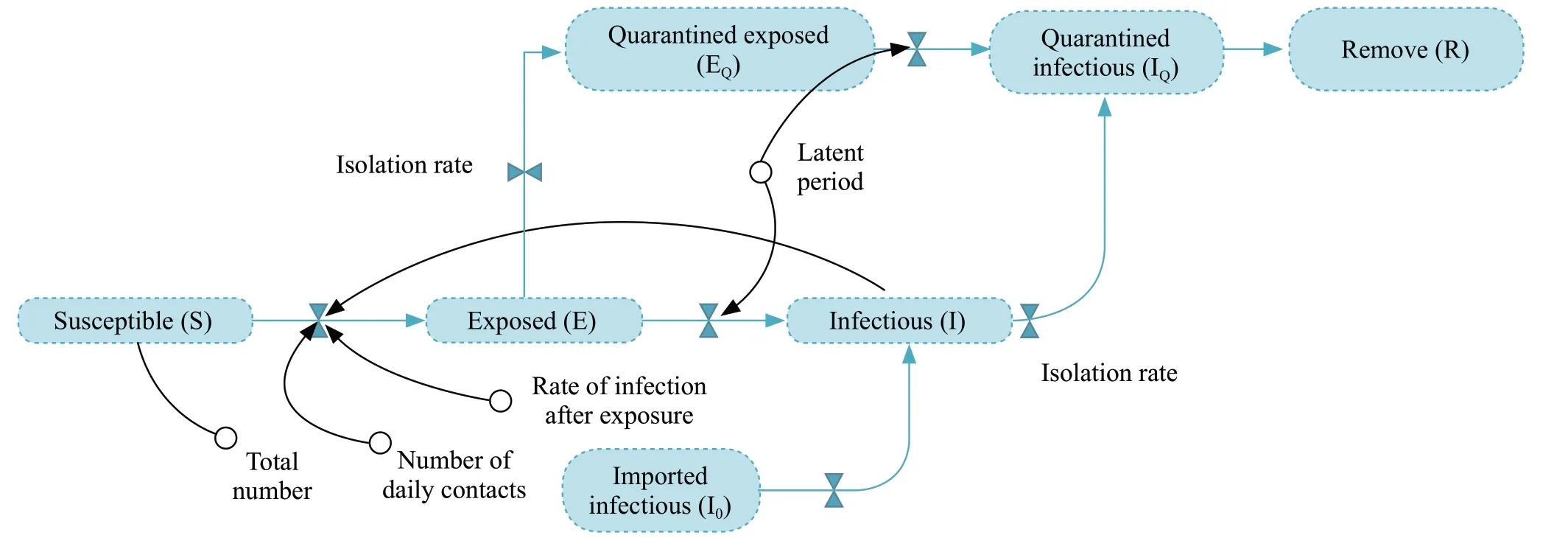
Figure 2.Modified SEIR model for COVID-19 outside the closed-loop system of the Beijing 2022 Olympic Winter Games.SEIR: susceptibilityexposed-infectious-remove.
A total of 142 foreign participants, regarded as imported cases (23.3%), were confirmed to be SARSCoV-2-positive in quarantine during the Tokyo Olympic Games,[2]compared with a much higher rate of 97.9%in the BOWG.Interestingly, a previous study depicted asymptomatic and pre-symptomatic cases as important infection sources of COVID-19.[10]In this study, 187 asymptomatic and pre-symptomatic cases entered the closed-loop system at least one day before being confirmed positive.However, only six cases were infected in the closed-loop system, demonstrating that comprehensive and rigorous preventive strategies,including vaccination, restricted social interactions, PCR tests, face mask-wearing, and the isolation of confirmed cases, effectively prevented SARS-CoV-2 from spreading inside the closed-loop system.The high proportion of asymptomatic participants in this study was mainly because all Games participants were subject to daily health monitoring and PCR testing within the closedloop system, and were PCR positive before the onset of symptoms, which was defined as asymptomatic.
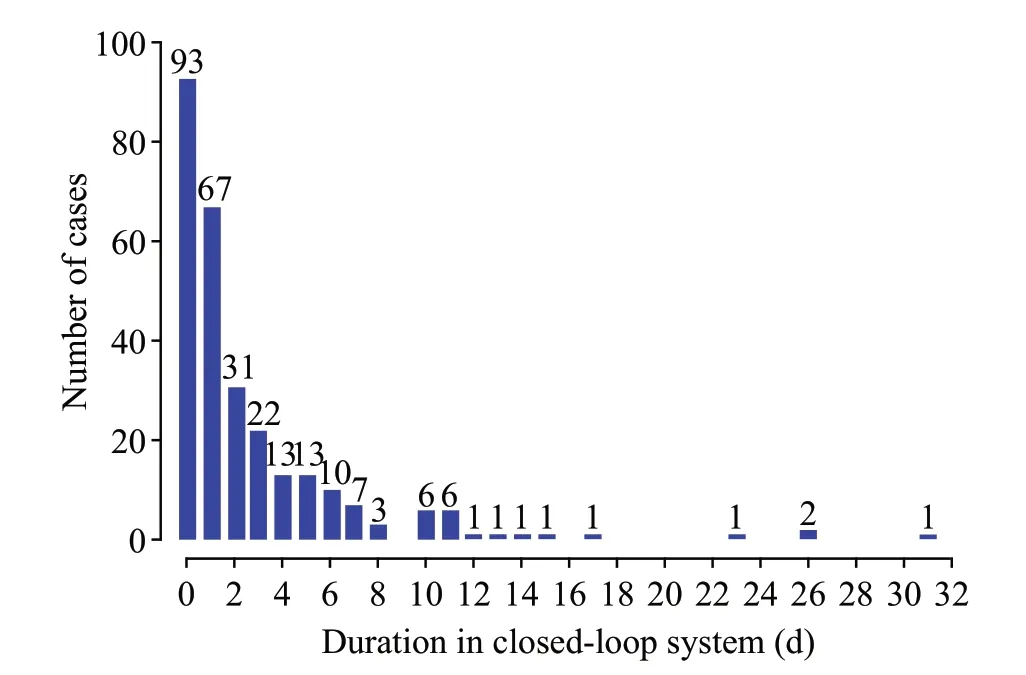
Figure 3.Diagnostic time interval of SARS-CoV-2 positive cases in the closed-loop system of the BWOG.
Non-athlete cases accounted for most of the SARSCoV-2-positive cases in Tokyo, possibly because the range of activities was not limited.Staff members were allowed to engage in normal social activities during the event, which may increase the infection rate to some Figure4.Simulation of COVID-19 outside the closed-loop system of the BWOG.extent.Similarly, non-athletes accounted for 83.2% of all cases in the BOWG, possibly reflecting the large number of non-athletes and the complexity of their social contact.In contrast, 47 athletes tested SARS-CoV-2-positive and thus could not participate in the competition.
An increase in SARS-CoV-2-positive cases among local residents was reported during the BOWG;[8]however, these cases were related to a cold storage facility and international mail.None of the infected residents had interacted with closed-loop personnel,suggesting that the closed-loop system prevented crossinfection between the Games participants and local residents, unlike the “bubble strategy”.[2]The simulation results of the closed-loop COVID-19 model for the BOWG showed that the exposure infection rate in the closed-loop system was much lower than average,indicating that the prevention and control protection measures within the closed-loop system reduced the probability of transmission.
During the BOWG, COVID-19 transmission in the community was initiated by international mail and the import of cold-chain products, which were both detected quickly by nucleic acid testing of key personnel.However, assuming that the BOWG adopted a semiclosed-loop management model, the original COVID-19 cases in the closed-loop system may cause a local COVID-19 epidemic in community.The simulation of the semi-closed-loop indicated that the cumulative number of confirmed cases would be 1,137 to 5,530 depending on whether the quarantine measures were implemented 3 d or 9 d later.

Figure 5.Scenario simulations for semi-closed-loop (Isolation measures were taken after 3 d or 9 d).
Because Chinese personnel entering the closed-loop system had to be vaccinated and needed to isolate for 14 d prior to entry, we did not simulate local patients entering semi-closed-loop and causing COVID-19 transmission in the loop.However, if a large-scale sporting event was held in another city where the local COVID-19 epidemic was more severe, transmission between the inside and outside of the loop would need to be considered.
This study had several limitations.First, all SARS-CoV-2-positive cases transported via the EMS were enrolled in our study, but cases in Zhangjiakou competition zones (a city hosting some of the competitive events outside of Beijing) were not included.Second,the infection route was assessed by the diagnostic time interval instead of by virology and epidemiology.Finally,departed participants who were potentially infected were not followed up.
CONCLUSION
The characteristics of SARS-CoV-2-positive cases during the BOWG were analyzed and revealed that imported cases were the main risk population in the closed-loop system.However, the comprehensive and rigorous preventive strategy implemented effectively contained the risk.The closed-loop system minimized the possibility of cross-infection between Games participants and local residents, and may therefore be a useful measure for the hosting of mass gatherings during the pandemic.
ACKNOWLEDGEMENTS
We thank all the Beijing EMS stafffor their efforts in transferring the confirmed SARS-CoV-2 positive cases.
Funding:National Key R&D Program of China (2022YFC3006201),and Beijing Public Health High-level Scholars Development Program (2022-1-001).
Ethical approval:The study was approved by the Ethics Committee of the Beijing Emergency Medical Center (No.2022-4-003) and the requirement for written informed consent was waived because the transport by EMS was conducted as the mass event.
Conflicts of interest:The authors declare that they have no competing interests.
Author contribution:RX and JPZ contributed equally to this work.JZ conceived the study idea for this article; RX and JL wrote the first draft; JL, LXZ, and HXL collected data; SJT and SMN analyzed data, and JZ suggested critical revisions.All authors were dedicated to the emergency medical services of the Beijing 2022 Olympic Winter Games.All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
All the supplementary files in this paper are available at http://wjem.com.cn.
 World journal of emergency medicine2023年6期
World journal of emergency medicine2023年6期
- World journal of emergency medicine的其它文章
- Tension urinothorax as a reversible cause of cardiac arrest: a case report
- A case of pulmonary mucormycosis presented with cardiac arrest
- Pyopneumothorax caused by Parvimonas micra and Prevotella oralis: a case report
- Hemorrhagic pancreatitis from fenofibrate and metformin toxicity: a case report
- The effect of prophylactic antibiotics in acute upper gastrointestinal bleeding patients in the emergency department
- The effects of hyperbaric oxygen therapy on paroxysmal sympathetic hyperactivity after cardiopulmonary resuscitation: a case series