
Primary mucinous carcinoma of the thyroid:case report and review of the literature
2023-01-11 09:44:44NengLiangZhangJianHuaWangWeiChengZhengJingLiJieTangTaoWangYiChen
Cancer Advances 2022年8期
Neng-Liang Zhang,Jian-Hua Wang,Wei Cheng,Zheng-Jing Li,Jie Tang,Tao Wang,Yi Chen
1Clinical Medical College of Dali University,Dali 671000,China.2Department of Oncology,The First Affiliated Hospital of Dali University,Dali 671000,China.3Department of Surgery,The First Affiliated Hospital of Dali University,Dali 671000,China.
Abstract Primary mucinous carcinoma of the thyroid gland which is more difficult to diagnose than common thyroid cancer is an extremely rare disease.It is a malignant tumor that can secrete mucus.A 45-year-old Chinese man came to seek medical care because he found a lump in his right side.Tomography showed that there was a space-occupying lesion on the right thyroid gland which compressed the tracheal.After the operation of total thyroidectomy and lymph node dissection in the right central area,the pathological examination showed that tumor cells existed,showing a small nest-like and cribriform distribution characteristics.There were broad fibrous tissues,a large amount of mucus around the tumur cell that had no obvious amyloid deposition.The tumor cells were positive for thyroid transcription factor-1 and paired box gene-8,while they were focally positive for thyroglobulin.Considering the histological features and immunohistochemical profile and ruling out mucinous cancers originating from other organs.The patient was diagnosed with primary mucinous carcinoma of the thyroid gland.This patient is still alive at present.Prognosis of primary mucinous carcinoma of the thyroid gland is usually poor.The best way to improve the prognosis of these patients maybe to do surgery of complete tumor+lymph node resection as soon as possible.
Keywords:mucinous carcinoma;thyroid cancer;immunohistochemistry;surgery
Introduction
The first primary mucinous carcinoma of the thyroid gland was reported by Diaz-Perez in 1976[1].To date,only 9 cases have been reported in the literature[1–9].Mucinous carcinoma has a high incidence in the digestive system.It can occur in all organs containing mucus-producing substances,such as the digestive tract,lungs,breasts,ovaries,and other parts.A retrospective study based on the SEER database of the National Cancer Institute showed that the incidence of gastrointestinal mucinous carcinoma accounts for approximately 5.3–8.7% of all gastrointestinal malignant neoplasms[10].There are fewer mucinous carcinomas in the thyroid.It is described as a mucinous variant of thyroid follicular cell carcinoma in the World Health Organization tumor classification,consisting of neoplastic follicular cells surrounded by a large amount of extracellular mucin deposits[11].This is an aggressive tumor.Thyroglobulin(TG),thyroid transcription factor-1(TTF-1),paired box gene(PAX)-8,etc.are positive on immunohistochemical staining.Calcitonin,carcinoembryonic antigen,epithelial membrane antigen,CD19,CD56 etc.,they are not generally expressed.TG,TTF-1 and PAX-8 positive,indicating that the tumor cells originated from the thyroid gland.Considering the histological features and immunohistochemical profile and ruling out mucinous cancers originating from other organs,the patient was diagnosed with primary mucinous carcinoma of the thyroid gland.It is shown that the early surgical procedure is essential according to the reported cases.The phenomenon of tumor recurrence and metastasis are often caused by incomplete resection.
Case presentation
The 45-year-old Chinese man found a mass on his right neck before 20 days ago with no progressive enlargement or pain in the discomfort,such as choking or breathing difficulties.The patient had a long-term smoking history(30 years),no history of neck radiotherapy,and no family history of thyroid disease.Computed tomography(Figure1)shows that the right lobe of the thyroid gland has a low density of about 2.6 cm×3 cm,and the internal density is uneven,and the internal density was uneven.After the enhancement,the uneven enhancement was obvious.Many plaques were necrotic,with clear boundaries,and the tumor oppressed the trachea.There were no obvious abnormalities in the left lobe of the thyroid and no obvious swollen lymph nodes in the neck.The patient’s routine blood counts and routine biochemical indicators were normal.His thyroid-stimulating hormone was 3.010(normal range=0.27–5.6 IU/mL),T3,thyroxine,F-T3 and free thyroxine were normal levels(T3 1.55 nmol/L,thyroxine 84.7 nmol/L,FT3 4.02 pmol/L,free thyroxine 14.8 pmol/L).Antithyroglobulin and anti-thyroperoxidase antibodies were also normal(antithyroglobulin 1.00%,anti thyroperoxidase 0.88%).The remaining parameters were calcitonin(24 pg/mL),parathyroid hormone(33.97 pg/mL),calcium(8.7 mg/dL),carcinoembryonic antigen(2.16 ng/mL),carbohydrate antigen(CA)125(11.33 U/mL),CA15-3(5.66 U/mL),CA199(9.91 U/mL),alpha-fetoprotein(1.97 ng/mL).Free prostate-specific antigen/total prostate-specific antigen dropped to 18.11%(normal range=25–100%).No metastatic carcinoma was found in the whole-body examination.Intraoperative pathological examination revealed poorly differentiated thyroid cancer and macroscopically no metastases in lymph nodes.He underwent total thyroidectomy and right central lymph no-de resection.The tissue can be seen by the naked eye as dark red irregular tissue with a partial envelope,and the cut surface was off-white,solid,tough,and lobulated.Pathological examination(Figure 2)revealed that tumor cells seemed to float in the abundant extracellular mucus pool,and the cells were atypical,with eosinophilic cytoplasm and nucleoli.A large amount of mucus was a characteristic of this disease.The tumor cells showed focally immunoreactive for HBME-1 and TG,and immunoreactive for PAX-8,TTF-1,and calectin-3,CD56,CD5,CD19,Syn,BRAF,etc.are not expressed.The KI-67 index was approximately 20%.After the operation,the parathyroid hormone decreased to 11 pg/mL.Considering the hypoparathyroidism caused by the operation.His free prostate-specific antigen/total prostate-specific antigen decreased to 14.53%.Color Doppler ultrasound showed that there were many swollen lymph nodes in the left groin,and the cortex and medulla were clearly demarcated.We will check this area regularly.
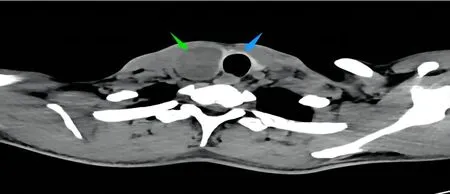
Figure 1 Computed tomography of thyroid.The green arrow points to the tumor and the blue arrow points to the airway compressed by the tumor.
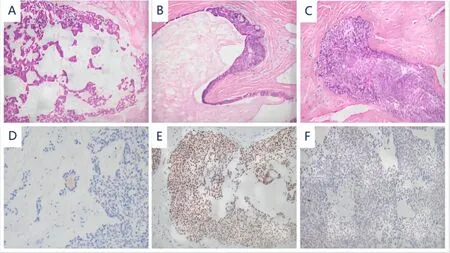
Figure 2 Pathological examinations.A,Proliferation of poorly differentiated carcinoma under the microscope,tumor cells are small nest-like with cribriform distribution characteristics,there is abundant extracellular mucus and small follicular structures(paraffin section,magnification×200;B,cytoplasm is eosinophilic,with mitotic figures,and nucleoli are visible(paraffin section,magnification×200);C,squamous metaplasia,tumor cell arrangement disorder,“pushing”invasion normal organization and destruction of the structure of the thyroid gland,and large atypical cells can be seen(paraffin section,magnification×200);D,tumor cells focally immunoreactive for TG;E,tumor cells immunoreactive for PAX-8;F,tumor cells immunoreactive for TFF-1.
Discussion
The origin of primary mucinous thyroid carcinoma is still controversial.Some scholars hypothesized that these mucin-producing cells came from the remnants of the thyroglossal canal,ectopic salivary gland,or the remnants of the last branchial cleft,especially through mucin-containing follicles[11].The latest findings have shown that mucinous cancers originating from different organs have similarities in transcriptome and genome.Over-expression of mucin-2 can lead to the production of a large number of mucins.The expression of mucin-2 upregulation regulation is a multicancer biomarker of mucinous histology and is regulated by DNA methylation[12].In addition,a mucous appearance alone is not enough to diagnose the disease,and sometimes mucus appearance can also be found in thyroid adenocarcinoma and adenomas.Primary thyroid carcinomas resembling neoplasms characteristic of the salivary glands, including mucoepidermoid carcinoma, sclerosing mucoepidermoid carcinoma with eosinophilia,produce mucin,the mucin is located in intracellular and focal areas[13].Immunohistochemistry is a reliable criterion for the diagnosis of primary mucinous thyroid carcinoma.Immunomarkers for follicular cells(TG,TTF1 and PAX-8)can assist in the correct diagnosis[14].This is a common characteristic of all known reported cases.In immunohistochemistry,the expression of TG indicates the origin of thyroid follicular,but the intensity and type of immunostaining are highly dependent on the tumor type.TG expression is relatively decreased in poorly differentiated thyroid carcinomas,and rare cases of thyroid carcinomas may have TG antibody focal immunostaining[15].This is consistent with the TG staining characteristics of this case,and it is considered to be the cause of the destruction of the thyroid parenchyma.TTF1,PAX-8 and low-molecular-weight cytokeratins assist in the distinction of mucinous thyroid carcinomas from metastatic mucinous carcinomas[14].Most mucinous carcinomas of the digestive tract,breast,and ovary do not express TG,TTF-1 and PAX-8,and they are helpful in identifying secondary mucinous thyroid carcinoma.It should be noted that mucoepidermoid carcinoma is a rare tumor that can also express TG and TTF-1[16].However,observation of pathological sections of mucoepidermoid carcinoma shows that malignant epidermal cells/squamous cells and mucous cells are mixed,which is not found in mucinous carcinoma of the thyroid[13].
Although the tumor had the ability to grow rapidly,most patients had no obvious pain,fever,weight loss,or other physical symptoms.However,most imaging findings show that the patients with tracheal compression had normal blood routine,biochemical examination,and thyroid function.It is not uncommon for cervical lymph nodes to be involved in the early stage.In the reported case,it was also observed that the patient came to the doctor because of a neck mass,and tomography showed that the tumor was compressing the trachea.The patient underwent total thyroidectomy,and lymph node removal in the right central area, postoperative complications of hypoparathyroidism occurred in this patient.Hypoparathyroidism is the most severe risk of thyroid surgery,and it causes disorders of calcium and phosphorus regulation in the body due to damage to the parathyroid glands.The more intensive and aggressive the surgery,the higher the risk of hypoparathyroidism development[17].Another study found that when compared with subtotal thyroidectomy,total thyroidectomy is safer and produces fewer complications in the long run[18].For mucinous carcinomas of the digestive tract,lungs,and breasts,surgery combined with radiotherapy,chemotherapy,and targeted molecular therapy are conventional treatments.However,in the case of reports of primary mucinous carcinoma of the thyroid,the effects of radiotherapy and chemotherapy are not good.Considering that the disease is prone to recurrence and metastasis,patients should undergo early total thyroidectomy and pay attention to preventing and treating any complications caused by the surgery.Table 1 summarizes the reported cases of primitive mucinous carcinomas of the thyroid.We discuss treatment choice in the context of reviewing previous case reports.In these 10 cases,the oldest patient was 82 years old,the youngest age was 32 years old,the median age was 59 years old,and the ratio of males to females was 1:1.Seven cases received total thyroidectomy plus neck regional lymph nodes resection,one case received hemithyroidectomy plus neck regional lymph node resection,and one case received hemithyroidectomy.Two patients underwent hemithyroidectomy,and the tumor recurred.Then a total thyroidectomy was performed.The disease had a high rate of recurrence and metastasis.In the known follow-up records,six patients died of recurrence and metastasis within 6 months to 4 years after diagnosis.The recurrence rate of patients who received early total thyroidectomy plus neck regional lymph node dissection is about 50%,and that of patients who received incomplete thyroidectomy,including incomplete lymph node dissection is 100%.Patients who underwent complete surgical resection early have a relatively good prognosis.Age and early cervical lymph node metastasis may be independent related factors of the subsequent progression.Four relapsed patients chose radiotherapy,chemotherapy,and iodine treatment to varying degrees,and none of them got obvious benefits.A female patient had a good prognosis after thyroid-stimulating hormone suppression therapy.However,a cohort study including 867 patients with intermediate-and high-risk differentiated thyroid cancer showed that thyrotropin suppression was not associated with the improvement of progression-free survival rate and overall survival rate.Patients with suppressed thyrotropin levels who survived 3 years were characterized by shorter overall survival than patients whose levels were not suppressed[19].Therefore,we still need to be cautious about the choice and timing of this treatment.The prognosis of this disease varies greatly among the first patient reported in 1976who underwent total thyroidectomy plus excision of the cervical regional lymph nodes.No recurrence or metastasis was found after 8 years of follow-up.At that time,the author believed that the disease was a type of benign tumor.However,subsequent case reports confirmed that this is a malignant thyroid tumor.Although the treatment effect is not good,with the current lack of treatment experience,early complete surgical resection may be the best choice for treatment.
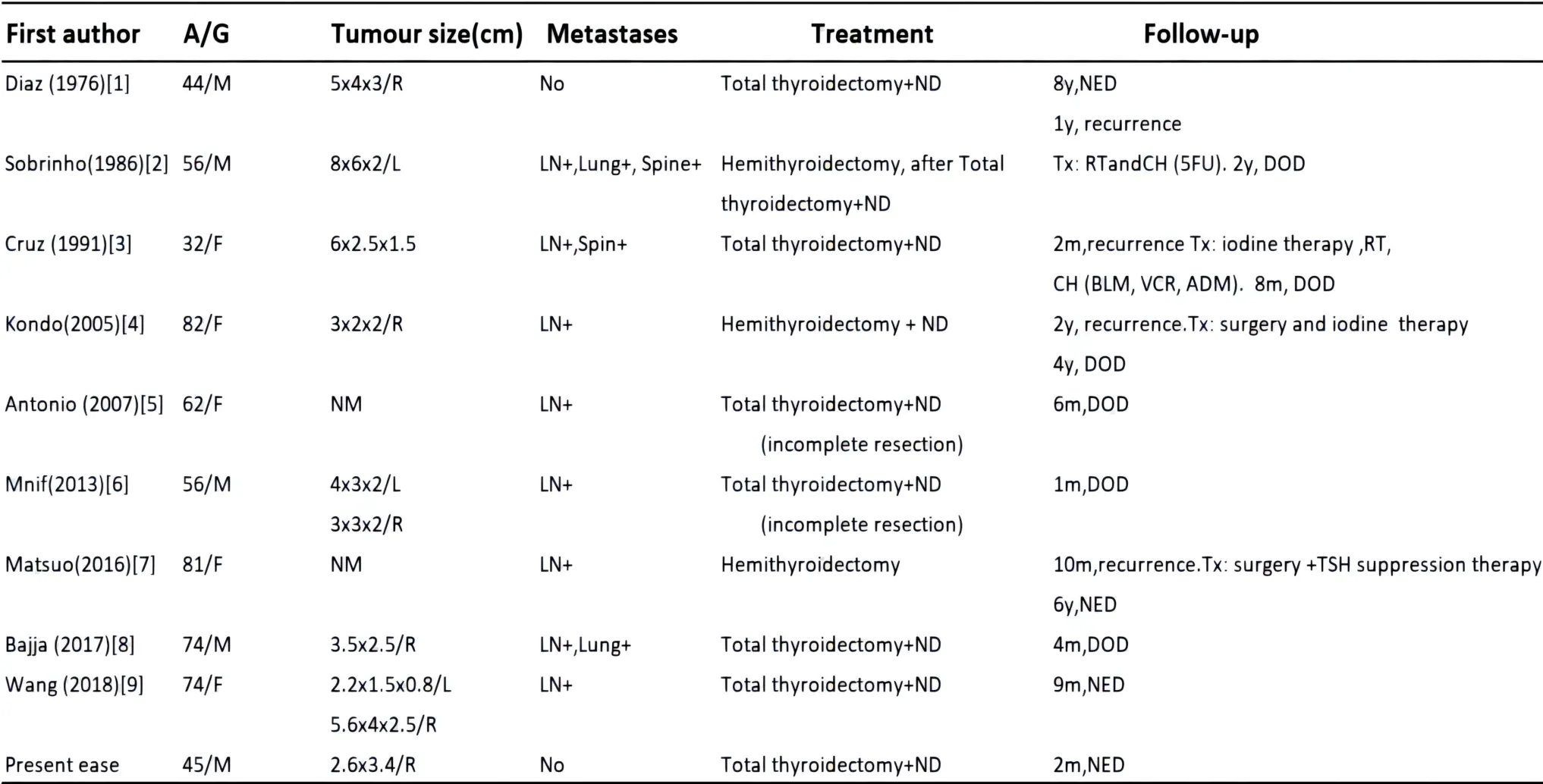
Table 1 summary of clinical data of reported primary mucinous carcinoma

- Cancer Advances的其它文章
- Advancing oncology nursing practice:a vital and changing role
- Research progression on immunotherapy biomarkers of peripheral blood in non-small-cell lung cancer
- Advances in the exploration of adjuvant therapy of colon cancer with Chinese medicine
- Research progress of uremic myopenia in traditional Chinese and western medicine
- Effect of Chinese herbal medicine on lung disease:an updated review
- Meta-analysis of therapy of Kang’ai injection combined with chemotherapy in the treatment of non-small cell lung cancer