
Expanding utility of cardiac computed tomography in infective endocarditis:A contemporary review
2022-07-30 07:52:30DiarmaidHughesRichardLinchangcoRezaReyaldeenBoXu
World Journal of Radiology 2022年7期
INTRODUCTION
Infective endocarditis(IE)is an infection of the endocardium,heart valves or intra-cardiac devices.It remains a challenging disease to diagnose and manage with high rates of morbidity and mortality[1,2].Echocardiography remains the main imaging modality used in IE;more recently,however,there is an increasing evidence base for a multimodality imaging approach for IE.Complementary imaging modalities including cardiac computed tomography(CCT)now play increasingly important roles in diagnosis,risk stratification and management of IE.CCT has certain advantages compared to echocardiography in being able to investigate for perivalvular extension,extra-cardiac complications of IE,including metastatic spread and planning for surgery including assessing for coronary artery disease.Advancements in CT technologies,including the use of dedicated cardiac gated four-dimensional CCT,have expanded the applications of CT in IE,demonstrating good sensitivity and specificity for diagnosing the complications of IE.This article aims to review the available evidence for the use of CCT in IE.
CLINICAL CONSIDERATIONS
The incidence of IE in the United States is estimated to be approximately 15 per 100000 persons annually[3,4],with Staphylococcus aureus(SA)being the most common pathogen followed by Viridans group Streptococci[5].A number of risk factors have been identified for acquiring IE,including the presence of a prosthetic valve,a previous episode of IE,patients with untreated cyanotic congenital heart disease,injection drug use,poor dentition and pre-existing valvular heart disease[6].The clinical presentation of IE can vary significantly from an acute life threatening illness to a more indolent chronic disease[7].The most common presenting symptoms are:fever,cardiac murmur,heart failure or complications from septic emboli[8].
The Duke criteria were developed in 1994 to assist in the risk stratification of patients with suspected IE into definite,possible and rejected cases of IE[9].These criteria have been since validated by a number of retrospective analyses,and underwent further modification in 2000 to reflect changing clinical practice and the emergence of SA as the most common pathogen encountered[10-12].Despite the updated clinical criteria for diagnosis of IE,there often remains a delay in diagnosis for many patients,commonly due to a lack of microbiological criteria from impropriate antibiotic use,with worse outcomes seen in these patients[13,14].Advances in CT technologies including improvements in both temporal and spatial resolution have enabled greater use of CCT for the diagnosis of IE.The European Society of Cardiology guidelines for the management of infective endocarditis reflect these advances in imaging techniques and include paravalvular lesions detected by CCT to be a major imaging criterion[15].The 2020 American College of Cardiology / American Heart Association Guideline for the management of patients with valvular heart disease also recommend the use of CCT as an adjunctive imaging modality for IE[16].
Echocardiography
Echocardiography,including transthoracic echocardiography(TTE)and transesophageal echocardiography(TEE)where appropriate,remain the first line imaging modality for the diagnosis and monitoring of IE[17,18].There are three main echocardiographic findings that are considered major criteria for the diagnosis of IE:vegetations,abscesses/pseudoaneurysms and new dehiscence of a prosthetic valve[15].In native valve endocarditis,the sensitivities for the diagnosis of a vegetation are approximately 70% for TTE and 96% for TEE,respectively[17].For prosthetic valve endocarditis(PVE),the sensitivities for diagnosing a vegetation are approximately 50% for TTE and 92% for TEE,respectively[17].There are many challenges in the diagnosis of IE with echocardiography,including small vegetations or embolization of the vegetation prior to imaging,difficulty visualizing the lesion in the setting of pre-existing valvular disease or with prosthetic valves.Small abscesses may also be challenging to diagnose,especially by TTE[19].There are also many mimics of IE that could result in a false positive diagnosis,such as Lambl’s excrescence,fibroelastomas,thrombus,degenerative lesions,prosthetic material/sutures or marantic lesions[20].CCT can therefore be helpful to assist in the diagnosis of IE,when there are equivocal findings by echocardiography or in challenging cases involving prosthetic valves[21].
Dedicated cardiac CT protocol for endocarditis evaluation
For evaluation of cardiac valves,multiphase imaging using a retrospectively ECG-gated acquisition is required to obtain an isotropic data set.Images are acquired in spiral mode utilizing a low pitch of 0.16 to 0.5 during 5-10 R-R intervals with a section thickness of 0.60 mm.Thin collimation is used for optimal visualization of the valve leaflets,typically 64 mm × 0.6 mm.The tube voltage used is adapted to the patient’s weight,and can vary between 100 to 120 kV.Gantry rotation time of 0.28 s to 0.35 s is used[22-27].The scan is typically performed in a limited field of view from the level of the carina to the cardiac apex.
Timing of the iodinated contrast bolus is important to optimize visualization of the involved cardiac valves.A monophasic contrast injection is most commonly used,with timing of the contrast bolus chosen for optimal visualization of the expected involved valve and cardiac chambers.Alternatively,biphasic contrast injection may be performed,which allows evaluation of all cardiac chambers and valves[28].Premedication with beta blockers may be used to regulate heart rate to less than 65-70 bpm if not contraindicated.This improves image quality by reducing artefacts related to cardiac motion and valvular motion.
The isotropic data set acquired from the retrospectively gated acquisition allows for reconstruction in any desired plane.In addition to static images,imaging at multiple points during the cardiac cycle also allows for creation of 4D cine images,allowing for evaluation of valve leaflet motion and planimetry.
Listen the next time when someone asks you something and you aGREe, because when you could simply say yes, instead you will say absolutely or without doubt or Oh, yeah, unquestionably - absolutely without doubt
When they were both alone, he said, On the way to church thou didst name Maid Maleen, who was my betrothed bride; if I could believe it possible, I should think she was standing21 before me thou art like her in every respect
UTILITY OF CARDIAC CT IN INFECTIVE ENDOCARDITIS
In the 2009 paper by Feuchter
[24]using surgical/pathological diagnosis as the reference standard,CCT had sensitivity of 96% and specificity of 97% for the diagnosis of vegetations.5 vegetations were missed by CCT(11%)either due to artefact or small size(≤ 4mm)[24].The performance of TEE was similar to CCT with sensitivity of 96% and specificity of 100%[24].CCT was found to be inferior to TEE for detecting leaflet perforations[24].The study by Gahide
[25]on aortic valve IE showed CCT had a sensitivity of 71% and a specificity of 100% for detecting vegetations,though the sensitivity was increased to 100% for large vegetations(> 10 mm).The 2012 paper by Fagman
[23]found that CCT detected vegetations in 7 out of 13 cases(54%),with a lower detection rate being potentially explained by artefact from the prosthetic valves obscuring the CCT images.The 2013 study by Habets
[35]found additional benefit with CCT in addition to usual work-up with TEE in PVE,with a final diagnosis being either determined clinically or at the time of surgery.They reported that usual work-up had sensitivity of 63% for detecting vegetations,which was increased to 100% with the use of CCT[35].The 2018 study by Koo
[27]reported sensitivity for CCT to detect vegetations of 91%,compared to 100% by TEE.Missed vegetations were smaller,and the authors also listed motion artefact and beam hardening from mechanical valves as reasons for the failure of CCT to detect the vegetations[27].Sims
[36]reported the sensitivity for detecting vegetations to be 70% for CCT(34 patients)and 96% for TEE(251 patients).The study by Oucho
[37]reported sensitivity of 92% for detecting vegetations for CCT,correctly identifying 12 of 13 cases who had vegetations confirmed at the time of surgery.The retrospective review on 122 patients by Koneru
[31]showed TEE to have a statistically significantly higher sensitivity for detecting vegetations compared to CCT at 85%
16%,though CCT did have a higher specificity at 96% compared to 69% for TEE.The lower sensitivity in detecting vegetations by CCT in this study may be related to only reviewing single-phase images,and the fact that the slice thickness used was 3 mm which was thicker than the other studies referenced above[31].In the 2019 paper by Hryniewiecki
[26]the sensitivity and specificity for detecting vegetations by CT were 89% and 71%,respectively,compared to TEE at 97% and 42%,respectively.The 2020 study by Sifaoui
[38]showed that TEE had a higher area under the curve(AUC)than CCT for detecting vegetations,with AUC for TEE of 0.86
AUC for CT of 0.69.
When he came to the outskirts26 of the wood he said to his followers27: You wait here, I ll manage the giants by myself ; and he went on into the wood, casting his sharp little eyes right and left about him
PERIVALVULAR COMPLICATIONS
Pseudoaneurysms and abscesses
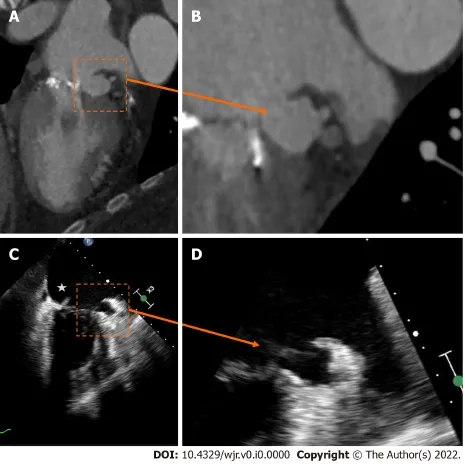
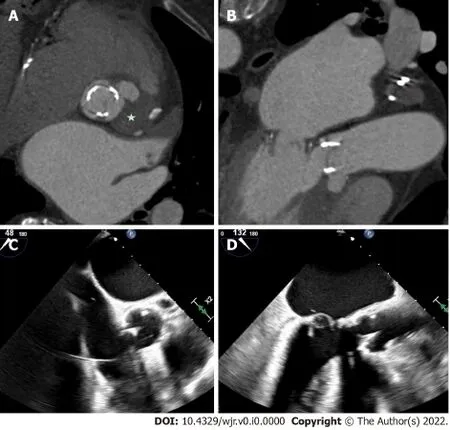
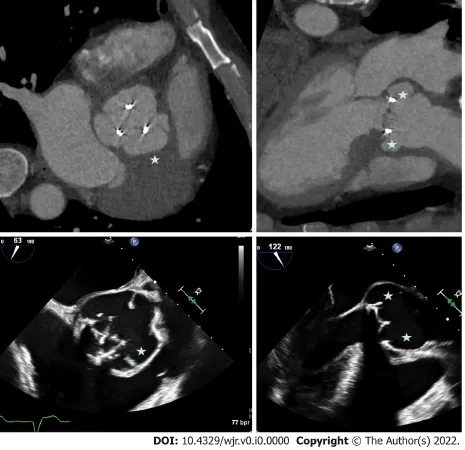
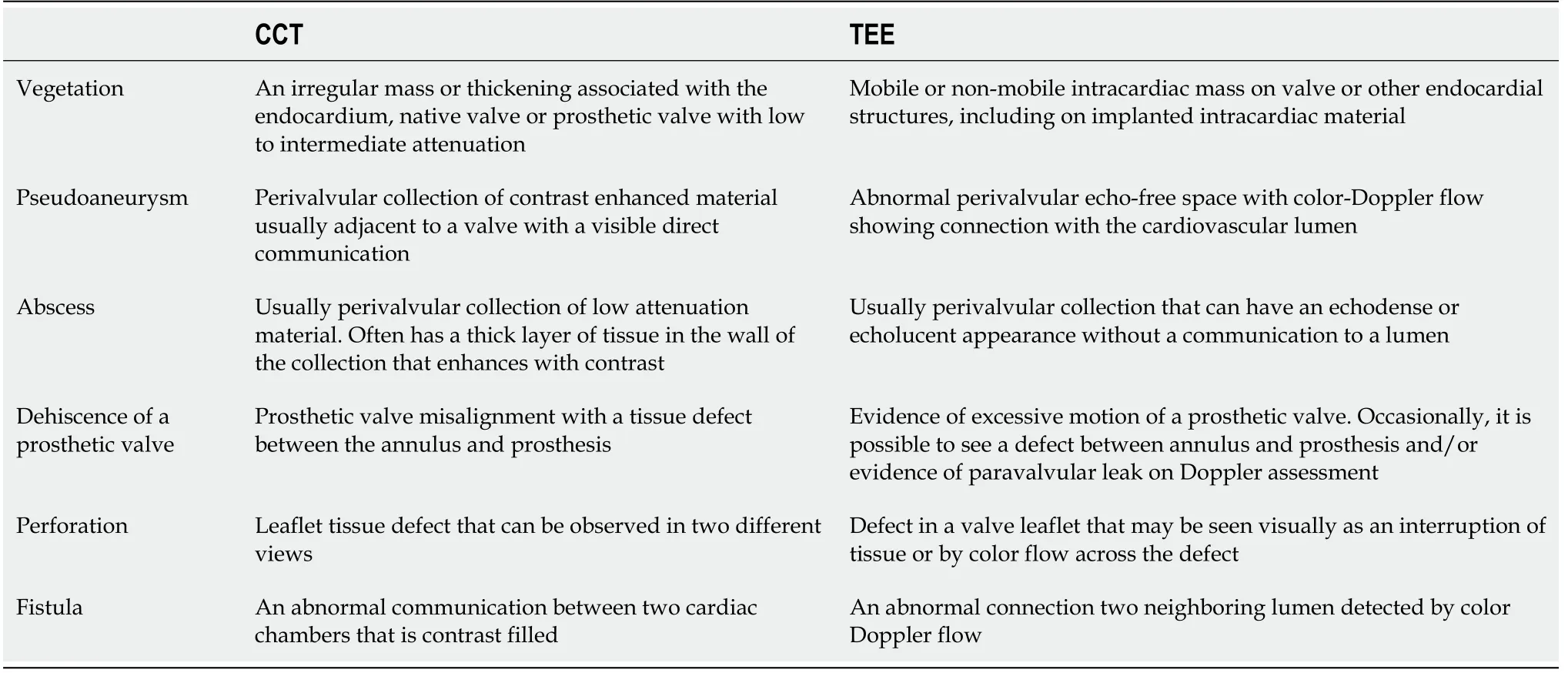
Perivalvular extension of IE,which includes pseudoaneurysms,abscesses and fistulae are associated with a higher rate of operative management and mortality[32-34].A pseudoaneurysm is a perivalvular cavity that is in communication with the cardiovascular lumen which results from an abscess rupturing into a cavity[17].On echocardiography,this appears as a pulsatile echo-free space with detectable Doppler color flow,while on CCT,it appears as an abnormal cavity close to the valve with direct communication with the heart chambers or major blood vessel[30].An abscess is a closed cavity with necrosis and purulent material not in communication with a cardiovascular cavity[17].On echocardiography,this appears as a thickened perivalvular area with a homogenous echo-dense or echo-lucent appearance.On CCT,abscesses appear as perivalvular collections of fluid encased in a thick layer of inflammatory tissue enhanced by the injection of contrast medium.See Figures 1-4 for examples ofcomparisons of TEE and CCT images in patients with perivalvular complications of IE(Table 2).


A 2009 study by Feuchter
[24]to investigate the value of CCT for the assessment of valvular abnormalities included 37 consecutive patients(29 of whom went on to have surgery)with clinically suspected IE who underwent both CCT and TEE.CCT identified all pseudoaneurysms and abscesses in this study with sensitivity and specificity of 100%,which was superior to TEE(sensitivity of 89% and a specificity of 100%)[24].CCT was also shown to be superior to TEE for perivalvular extension of the IE,identifying myocardial and pericardial extension more often than TEE[24].In a 2009 prospective study,19 patients with aortic valve endocarditis requiring surgical intervention underwent CCT preoperatively[25].The majority of patients(approx.90%)had native valve IE.This study showed that CCT had sensitivity and specificity for diagnosing pseudoaneurysms of 100% and 92%,respectively,and CCT correctly identified all cases where there was extension of IE into the intervalvular fibrosa[25].This paper did not report the TEE findings for their participants[25].
A vegetation is a mass-like lesion of infected material composed of fibrin,platelets and microorganisms attached to an endocardial structure or on an implanted cardiac device(CIED)[40,41].On echocardiography,this appears as an oscillating or non-oscillating intracardiac echodensity,which can be attached to a valve,other endocardial surface or cardiac device[15].A vegetation tends to move with the cardiac cycle,and is more frequently found on the atrial side of the atrioventricular valves and the ventricular side of the semi-lunar valves[15].On CT,vegetations appear as hypodense homogeneous irregular masses,which can be attached to a valve or other cardiac structures[30].
Two studies from 2018(Ouchi
[31]and Koneru
[37])retrospectively investigated the utility of CCT in IE with intra-operative findings as the reference standard.CCT performed better than TEE in detecting abscess/pseudoaneurysm in prosthetic valves with sensitivity of 81%(versus 64% for TEE)in the study by Koneru
[31].CCT had sensitivity of 100% sensitivity for detecting perivalvular complications,such as pseudoaneurysms in the paper by Ouchi
[37].A 2019 study by Hryniewiecki
[26]investigated 53 consecutive patients who had perivalvular complications from IE,who also underwent CCT and TEE pre-operatively.They showed the sensitivity and specificity for detecting abscesses/pseudoaneurysms for CCT were 81% and 90%,respectively,compared to 63% and 90%,respectively for TEE[26].A 2020 study of 68 patients reported by Sifaoui
with definite left-sided IE who underwent CCT and TEE reported the comparison of CCT and TEE to detect perivalvular complications[38].They showed again that CT had a higher sensitivity for detecting pseudoaneurysms at 100%,compared to TEE at 67%[38].
Overall,the current evidence base suggests that the diagnostic performance of CCT is likely superior to that of TEE for the detection of pseudoaneurysms and abscesses in appropriately selected cases.A recent meta-analysis reported pooled sensitivity and specificity for CCT for the detection of peri-annular complications of 88% and 93%,respectively,compared to TEE at 70% and 96%,respectively[39].
The identification of perivalvular complications is important for prognostic and management considerations.These sequelae of invasive IE,which are more common with aortic valve endocarditis and PVE,have been associated with increased rates of surgical management,and may confer an increased risk of mortality[32,33].Therefore,a multimodality imaging strategy for IE that includes CCT would have the ability to identify more of these complications,compared to using TEE alone,and therefore impact on decision making for patients.
Vegetations
A paper by Fagman
[23]reported in 2012 on 27 consecutive patients who had TEE findings of aortic valve PVE and investigated the strength of agreement between the TEE and CT results.They found a strength of agreement compared to TEE was 0.68 for abscesses and 0.75 for dehiscence[23].However,using surgery as the reference standard(16 patients went on to have surgery),CCT had sensitivity of 91% to detect pseudoaneurysms /abscesses compared to 82% for TEE[23].A 2013 study investigated the additional value of CCT beyond the usual evaluation with TEE in PVE in 28 patients,with a final diagnosis being either determined clinically or at the time of surgery as reported by Habets
[35].They reported that usual evaluation had sensitivity of 68% for detecting periannular complications(mycotic aneurysms and abscesses),which was increased to 100% with the use of CCT[35].Koo
[27]also compared CCT
TEE using intra-operative findings as the reference standard in 2018.They enrolled 49 patients,12 of whom had PVE[27].The overall detection of IE by CCT was 94%,compared to 96% by TEE[27].CCT performed better than TEE at detecting abscess/pseudoaneurysms,with sensitivities of 60% for CCT and 40% for TEE,respectively[27].A retrospective study from 2018 by Sims
[36]investigated the performance of CCT in the pre-operative evaluation of IE.In total,they had 251 patients undergoing TEE with 34 of these patients also having a CCT[36].The sensitivity of CCT for detecting abscesses/pseudoaneurysms was 91%,which was superior to TEE at 78%[36].CCT was reported to have a lower sensitivity for detecting fistulae at 50%
79% for TEE,and dehiscence at 57%
70% for TEE[36].
CCT has the ability to assess for valvular lesions,perivalvular extension,metastatic spread/embolization,as well as aortic anatomy.CCT may also be used in appropriate cases for the assessment of coronary artery disease[30].This is particularly relevant in patients with aortic valve IE and vegetations,whereby invasive coronary angiography may be relatively contraindicated,due to the potential risk of causing the vegetations to embolize during the procedure.CCT can detect valvular lesions,such as vegetations,prosthetic valve dehiscence in addition to perivalvular lesions such as abscesses,fistulae and pseudoaneurysms[26,31].Table 1 compares the various definitions for IE detected on CCT
TEE.
He lay down where he was and fell asleep, and did not awake before it was bright daylight, and he heard steps outside, and the noise of the key being put into the lock
INCREMENTAL VALUE OF CCT IN INFECTIVE ENODCARDITIS
Pre-operative assessment
In addition to the advantages related to the management of IE as outlined above,CCT can also assist in the pre-operative planning of IE surgery.In patients with prior cardiothoracic surgery,CCT can delineate the relationship of cardiovascular structures to the sternum and the location of the coronary artery bypass grafts(CABG).See Figure 8 for CCT images of a patient with a prior CABG.For all patients,CCT can identify calcification of the ascending aorta(‘porcelain aorta’),which may preclude surgery as well as give precise anatomic location and extent of the degree of calcification of the subclavian,axillary and femoral arteries.The advantage of having a pre-operative CCT was described by Merlo
[43]with reported lower rates of stroke and mortality in patients undergoing pre-operative CCT followed by primary cardiac surgery,
those without pre-operative CCT imaging.Figure 9 shows a CCT in a patient with vascular calcification.
Because images are acquired throughout the entire cardiac cycle,this results in a significantly higher radiation dose penalty compared to prospectively gated CT as used typically in CT angiography of the coronary arteries.Radiation dose may be lowered utilizing methods such as iterative reconstruction and ECG-triggered radiation dose modulation.However,ECG-triggered dose modulation may result in suboptimal evaluation during the phase of reduced tube current,typically the systolic phase[29].There are specific protocols used for visualizing the various cardiac and extra manifestations of IE and for preoperative planning.Herein,we group all of these into an umbrella term of CCT,referring to ECG-gated CT of the chest with contrast.There are some situations,such as during investigation for septic emboli to the visceral organs,when abdominal imaging may also be needed.


Pre-operative assessment
In addition to the advantages related to the management of IE as outlined above,CCT can also assist in the pre-operative planning of IE surgery[44-50].In patients with prior cardiothoracic surgery,CCT can delineate the relationship of cardiovascular structures to the sternum and the location of the coronary artery bypass grafts(CABG).See Figure 8 for CCT images of a patient with a prior CABG[50-60].For all patients,CCT can identify calcification of the ascending aorta(‘porcelain aorta’),which may preclude surgery as well as give precise anatomic location and extent of the degree of calcification of the subclavian,axillary and femoral arteries[61,62].The advantage of having a pre-operative CCT was described by Merlo
[43]with reported lower rates of stroke and mortality in patients undergoing pre-operative CCT followed by primary cardiac surgery,
those without pre-operative CCT imaging.Figures 9 and 10 shows a CCT in a patient with vascular calcification.

CONCLUSION
With tears and groans20 the peasant told him the whole dreadful story, and the hare, filled with anger and compassion21, comforted him as best he could, and promised to help him in his revenge
FOOTNOTES
Hughes D,Lingchangco R,Reyaldeen R and Xu B were involved in the conceptualization,writing,revision and final approval of the manuscript.
Overall,the current evidence base suggests that TEE is overall superior to CCT for the detection of vegetations,particular small vegetations,with pooled sensitivity for TEE from a recent meta-analysis of 94%[42].CCT demonstrated a lower pooled sensitivity,at 64% for the detection of vegetations[42].There was a wide range of results reported likely related to small sample sizes,differing patient populations and different protocols used for imaging.While CCT should not replace echocardiography as the first line imaging tool in the majority of patients primarily to detect vegetations,in a small subset of patients who could not undergo clinical indicated TEE(
esophageal pathology),CCT may add diagnostic value.CCT has also been shown to improve the diagnostic accuracy overall,when used in combination with TEE[35].For example Figure 5 shows a hypoattenuating lesion on a mechanical aortic valve that was more clearly defined on CCT.Figures 6 and 7 shows an examples of an aortic graft and aortic stent infections that can be difficult to image with TEE.
No conflicts of interest to declare for all authors for this article.
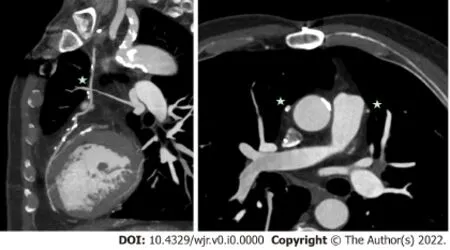
With improvements in the temporal and spatial resolution of CCT technology,including the use of dedicated 4D CCT,there has been an expanding role of CCT imaging in IE.CCT has been shown to be superior to TEE for the identification of pseudoaneurysms and abscesses in appropriately selected cases,while the combination of both modalities results in the greatest sensitivity for detection.TEE is superior to CCT for small vegetations;however this advantage is less marked for larger vegetations.In addition,CCT has a number of adjunctive uses in IE beyond evaluation of valvular pathology.CCT can aid in the diagnosis of embolic events,such as pulmonary complications in RSIE.It can also be used to diagnose significant CAD in low to intermediate risk patients preoperatively,or when there is a contraindication to ICA,such as when there is a large aortic valve vegetation.CCT can also be helpful for pre-operative planning to assess the relationship of the cardiovascular structures in relation to the sternum,which is particularly helpful in re-do sternotomy cases.The addition of hybrid techniques such as positron emission computed tomography or SPECT/CT,has been shown to improve the diagnostic accuracy in challenging cases of PVE.Greater awareness of the strengths,weaknesses and appropriate applications of CCT in IE will assist in its optimal use for improved diagnosis and management of this challenging condition.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
When I married, I told my wife Susan about the significant part the lowly pickle jar had played in my life as a boy. In my mind, it defined, more than anything else, how much my dad had loved me. No matter how rough things got at home, Dad continued to doggedly15 drop his coins into the jar. Even the summer when Dad got laid off from the mill, and Mama had to serve dried beans several times a week, not a single dime10 was taken from the jar. To the contrary, as Dad looked across the table at me, pouring catsup over my beans to make them more palatable16, he became more determined17 than ever to make a way out for me. When you finish college, son, he told me, his eyes glistening18, you ll never have to eat beans again unless you want to.
Then he asked if the hermit could shelter him and his beasts for the night, and the hermit said Yes ; so, very soon the king had watered and tethered his horse, and, after a supper of bread and parched22 peas, lay down in the cave, with the hound at his feet, and tried to go to sleep
United States
Diarmaid Hughes 0000-0003-3110-6759;Richard Linchangco 0000-0002-9265-9851;Reza Reyaldeen 0000-0001-7501-2354;Bo Xu 0000-0002-2985-7468.
Wang LL
We volleyed back and forth4 a few favorite lines. I love you more than peanut butter. Well, I love you more than television. I even love you more than bubble gum. It was my turn again, and I made the move that usually brings victory. Too bad chickadee. I love you bigger than the universe! On this day, however, Amanda was not going to give up. I could see she was thinking. Mom, she said in a quiet voice, I love you more than myself.
A
Wang LL
1 Sy RW,Kritharides L.Health care exposure and age in infective endocarditis:results of a contemporary population-based profile of 1536 patients in Australia.
2010;31:1890-1897[PMID:20453066 DOI:10.1093/eurheartj/ehq110]
2 Mansur AJ,Grinberg M,da Luz PL,Bellotti G.The complications of infective endocarditis.A reappraisal in the 1980s.
1992;152:2428-2432[PMID:1456853]
3 Pant S,Patel NJ,Deshmukh A,Golwala H,Patel N,Badheka A,Hirsch GA,Mehta JL.Trends in infective endocarditis incidence,microbiology,and valve replacement in the United States from 2000 to 2011.
2015;65:2070-2076[PMID:25975469 DOI:10.1016/j.jacc.2015.03.518]
4 Toyoda N,Chikwe J,Itagaki S,Gelijns AC,Adams DH,Egorova NN.Trends in Infective Endocarditis in California and New York State,1998-2013.
2017;317:1652-1660[PMID:28444279 DOI:10.1001/jama.2017.4287]
5 Murdoch DR,Corey GR,Hoen B,Miró JM,Fowler VG Jr,Bayer AS,Karchmer AW,Olaison L,Pappas PA,Moreillon P,Chambers ST,Chu VH,Falcó V,Holland DJ,Jones P,Klein JL,Raymond NJ,Read KM,Tripodi MF,Utili R,Wang A,Woods CW,Cabell CH;International Collaboration on Endocarditis-Prospective Cohort Study(ICE-PCS)Investigators.Clinical presentation,etiology,and outcome of infective endocarditis in the 21st century:the International Collaboration on Endocarditis-Prospective Cohort Study.
2009;169:463-473[PMID:19273776 DOI:10.1001/archinternmed.2008.603]
6 Strom BL,Abrutyn E,Berlin JA,Kinman JL,Feldman RS,Stolley PD,Levison ME,Korzeniowski OM,Kaye D.Risk factors for infective endocarditis:oral hygiene and nondental exposures.
2000;102:2842-2848[PMID:11104742 DOI:10.1161/01.cir.102.23.2842]
7 Baddour LM,Wilson WR,Bayer AS,Fowler VG Jr,Tleyjeh IM,Rybak MJ,Barsic B,Lockhart PB,Gewitz MH,Levison ME,Bolger AF,Steckelberg JM,Baltimore RS,Fink AM,O'Gara P,Taubert KA;American Heart Association Committee on Rheumatic Fever,Endocarditis,and Kawasaki Disease of the Council on Cardiovascular Disease in the Young,Council on Clinical Cardiology,Council on Cardiovascular Surgery and Anesthesia,and Stroke Council.Infective Endocarditis in Adults:Diagnosis,Antimicrobial Therapy,and Management of Complications:A Scientific Statement for Healthcare Professionals From the American Heart Association.
2015;132:1435-1486[PMID:26373316 DOI:10.1161/CIR.0000000000000296]
8 Bayer AS.Infective endocarditis.
1993;17:313-20;quiz 321[PMID:8218670 DOI:10.1093/clinids/17.3.313]
9 Durack DT,Lukes AS,Bright DK.New criteria for diagnosis of infective endocarditis:utilization of specific echocardiographic findings.Duke Endocarditis Service.
1994;96:200-209[PMID:8154507 DOI:10.1016/0002-9343(94)90143-0]
10 Sekeres MA,Abrutyn E,Berlin JA,Kaye D,Kinman JL,Korzeniowski OM,Levison ME,Feldman RS,Strom BL.An assessment of the usefulness of the Duke criteria for diagnosing active infective endocarditis.
1997;24:1185-1190[PMID:9195080 DOI:10.1086/513657]
11 Hoen B,Béguinot I,Rabaud C,Jaussaud R,Selton-Suty C,May T,Canton P.The Duke criteria for diagnosing infective endocarditis are specific:analysis of 100 patients with acute fever or fever of unknown origin.
1996;23:298-302[PMID:8842267 DOI:10.1093/clinids/23.2.298]
12 Li JS,Sexton DJ,Mick N,Nettles R,Fowler VG Jr,Ryan T,Bashore T,Corey GR.Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis.
2000;30:633-638[PMID:10770721 DOI:10.1086/313753]
13 Fukuchi T,Iwata K,Ohji G.Failure of early diagnosis of infective endocarditis in Japan--a retrospective descriptive analysis.
2014;93:e237[PMID:25501088 DOI:10.1097/MD.0000000000000237]
14 Naderi HR,Sheybani F,Erfani SS.Errors in diagnosis of infective endocarditis.
2018;146:394-400[PMID:29310727 DOI:10.1017/S0950268817002977]
15 Habib G,Lancellotti P,Antunes MJ,Bongiorni MG,Casalta JP,Del Zotti F,Dulgheru R,El Khoury G,Erba PA,Iung B,Miro JM,Mulder BJ,Plonska-Gosciniak E,Price S,Roos-Hesselink J,Snygg-Martin U,Thuny F,Tornos Mas P,Vilacosta I,Zamorano JL;ESC Scientific Document Group.2015 ESC Guidelines for the management of infective endocarditis:The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology(ESC).Endorsed by:European Association for Cardio-Thoracic Surgery(EACTS),the European Association of Nuclear Medicine(EANM).
2015;36:3075-3128[PMID:26320109 DOI:10.1093/eurheartj/ehv319]
16 Otto CM,Nishimura RA,Bonow RO,Carabello BA,Erwin JP 3rd,Gentile F,Jneid H,Krieger EV,Mack M,McLeod C,O'Gara PT,Rigolin VH,Sundt TM 3rd,Thompson A,Toly C.2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease:Executive Summary:A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.
2021;143:e35-e71[PMID:33332149 DOI:10.1161/CIR.0000000000000932]
17 Habib G,Badano L,Tribouilloy C,Vilacosta I,Zamorano JL,Galderisi M,Voigt JU,Sicari R,Cosyns B,Fox K,Aakhus S;European Association of Echocardiography.Recommendations for the practice of echocardiography in infective endocarditis.
2010;11:202-219[PMID:20223755 DOI:10.1093/ejechocard/jeq004]
18 Haq IU,Haq I,Griffin B,Xu B.Imaging to evaluate suspected infective endocarditis.
2021;88:163-172[PMID:33648969 DOI:10.3949/ccjm.88a.19142]
19 Daniel WG,Mügge A,Martin RP,Lindert O,Hausmann D,Nonnast-Daniel B,Laas J,Lichtlen PR.Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography.
1991;324:795-800[PMID:1997851 DOI:10.1056/NEJM199103213241203]
20 Zmaili MA,Alzubi JM,Kocyigit D,Bansal A,Samra GS,Grimm R,Griffin BP,Xu B.A Contemporary 20-Year Cleveland Clinic Experience of Nonbacterial Thrombotic Endocarditis:Etiology,Echocardiographic Imaging,Management,and Outcomes.
2021;134:361-369[PMID:32827467 DOI:10.1016/j.amjmed.2020.06.047]
21 Lo Presti S,Elajami TK,Zmaili M,Reyaldeen R,Xu B.Multimodality imaging in the diagnosis and management of prosthetic valve endocarditis:A contemporary narrative review.
2021;13:254-270[PMID:34589164 DOI:10.4330/wjc.v13.i8.254]
22 Altiok E,Koos R,Schr?der J,Brehmer K,Hamada S,Becker M,Mahnken AH,Almalla M,Dohmen G,Autschbach R,Marx N,Hoffmann R.Comparison of two-dimensional and three-dimensional imaging techniques for measurement of aortic annulus diameters before transcatheter aortic valve implantation.
2011;97:1578-1584[PMID:21700756 DOI:10.1136/hrt.2011.223974]
23 Fagman E,Perrotta S,Bech-Hanssen O,Flinck A,Lamm C,Olaison L,Svensson G.ECG-gated computed tomography:a new role for patients with suspected aortic prosthetic valve endocarditis.
2012;22:2407-2414[PMID:22622348 DOI:10.1007/s00330-012-2491-5]
24 Feuchtner GM,Stolzmann P,Dichtl W,Schertler T,Bonatti J,Scheffel H,Mueller S,Plass A,Mueller L,Bartel T,Wolf F,Alkadhi H.Multislice computed tomography in infective endocarditis:comparison with transesophageal echocardiography and intraoperative findings.
2009;53:436-444[PMID:19179202 DOI:10.1016/j.jacc.2008.01.077]
25 Gahide G,Bommart S,Demaria R,Sportouch C,Dambia H,Albat B,Vernhet-Kovacsik H.Preoperative evaluation in aortic endocarditis:findings on cardiac CT.
2010;194:574-578[PMID:20173130 DOI:10.2214/AJR.08.2120]
26 Hryniewiecki T,Zatorska K,Abramczuk E,Zakrzewski D,Szymański P,Ku?mierczyk M,Micha?owska I.The usefulness of cardiac CT in the diagnosis of perivalvular complications in patients with infective endocarditis.
2019;29:4368-4376[PMID:30643945 DOI:10.1007/s00330-018-5965-2]
27 Koo HJ,Yang DH,Kang JW,Lee JY,Kim DH,Song JM,Kang DH,Song JK,Kim JB,Jung SH,Choo SJ,Chung CH,Lee JW,Lim TH.Demonstration of infective endocarditis by cardiac CT and transoesophageal echocardiography:comparison with intra-operative findings.
2018;19:199-207[PMID:28329276 DOI:10.1093/ehjci/jex010]
28 Vrachliotis TG,Bis KG,Haidary A,Kosuri R,Balasubramaniam M,Gallagher M,Raff G,Ross M,O'neil B,O'neill W.Atypical chest pain:coronary,aortic,and pulmonary vasculature enhancement at biphasic single-injection 64-section CT angiography.
2007;243:368-376[PMID:17400761 DOI:10.1148/radiol.2432060447]
29 Jakobs TF,Becker CR,Ohnesorge B,Flohr T,Suess C,Schoepf UJ,Reiser MF.Multislice helical CT of the heart with retrospective ECG gating:reduction of radiation exposure by ECG-controlled tube current modulation.
2002;12:1081-1086[PMID:11976849 DOI:10.1007/s00330-001-1278-x]
30 Grob A,Thuny F,Villacampa C,Flavian A,Gaubert JY,Raoult D,Casalta JP,Habib G,Moulin G,Jacquier A.Cardiac multidetector computed tomography in infective endocarditis:a pictorial essay.
2014;5:559-570[PMID:25225108 DOI:10.1007/s13244-014-0353-1]
31 Koneru S,Huang SS,Oldan J,Betancor J,Popovic ZB,Rodriguez LL,Shrestha NK,Gordon S,Pettersson G,Bolen MA.Role of preoperative cardiac CT in the evaluation of infective endocarditis:comparison with transesophageal echocardiography and surgical findings.
2018;8:439-449[PMID:30214859 DOI:10.21037/cdt.2018.07.07]
32 Baumgartner FJ,Omari BO,Robertson JM,Nelson RJ,Pandya A,Milliken JC.Annular abscesses in surgical endocarditis:anatomic,clinical,and operative features.
2000;70:442-447[PMID:10969660 DOI:10.1016/s0003-4975(00)01363-1]
33 Graupner C,Vilacosta I,SanRomán J,Ronderos R,Sarriá C,Fernández C,Mújica R,Sanz O,Sanmartín JV,Pinto AG.Periannular extension of infective endocarditis.
2002;39:1204-1211[PMID:11923047 DOI:10.1016/s0735-1097(02)01747-3]
34 Harris WM,Sinha S,Caputo M,Angelini GD,Ahmed EM,Rajakaruna C,Benedetto U,Vohra HA.Surgical outcomes and optimal approach to treatment of aortic valve endocarditis with aortic root abscess.
2022;37:1917-1925[PMID:35384049 DOI:10.1111/jocs.16464]
35 Habets J,Tanis W,van Herwerden LA,van den Brink RB,Mali WP,de Mol BA,Chamuleau SA,Budde RP.Cardiac computed tomography angiography results in diagnostic and therapeutic change in prosthetic heart valve endocarditis.
2014;30:377-387[PMID:24293045 DOI:10.1007/s10554-013-0335-2]
36 Sims JR,Anavekar NS,Chandrasekaran K,Steckelberg JM,Wilson WR,Gersh BJ,Baddour LM,DeSimone DC.Utility of cardiac computed tomography scanning in the diagnosis and pre-operative evaluation of patients with infective endocarditis.
2018;34:1155-1163[PMID:29450741 DOI:10.1007/s10554-018-1318-0]
37 Ouchi K,Sakuma T,Ojiri H.Cardiac computed tomography as a viable alternative to echocardiography to detect vegetations and perivalvular complications in patients with infective endocarditis.
2018;36:421-428[PMID:29713878 DOI:10.1007/s11604-018-0740-5]
38 Sifaoui I,Oliver L,Tacher V,Fiore A,Lepeule R,Moussafeur A,Huguet R,Teiger E,Audureau E,Derbel H,Luciani A,Kobeiter H,Lim P,Ternacle J,Deux JF.Diagnostic Performance of Transesophageal Echocardiography and Cardiac Computed Tomography in Infective Endocarditis.
2020;33:1442-1453[PMID:32981789 DOI:10.1016/j.echo.2020.07.017]
39 Jain V,Wang TKM,Bansal A,Farwati M,Gad M,Montane B,Kaur S,Bolen MA,Grimm R,Griffin B,Xu B.Diagnostic performance of cardiac computed tomography
transesophageal echocardiography in infective endocarditis:A contemporary comparative meta-analysis.
2021;15:313-321[PMID:33281097 DOI:10.1016/j.jcct.2020.11.008]
40 Habib G,Hoen B,Tornos P,Thuny F,Prendergast B,Vilacosta I,Moreillon P,de Jesus Antunes M,Thilen U,Lekakis J,Lengyel M,Müller L,Naber CK,Nihoyannopoulos P,Moritz A,Zamorano JL;ESC Committee for Practice Guidelines.Guidelines on the prevention,diagnosis,and treatment of infective endocarditis(new version 2009):the Task Force on the Prevention,Diagnosis,and Treatment of Infective Endocarditis of the European Society of Cardiology(ESC).Endorsed by the European Society of Clinical Microbiology and Infectious Diseases(ESCMID)and the International Society of Chemotherapy(ISC)for Infection and Cancer.
2009;30:2369-2413[PMID:19713420 DOI:10.1093/eurheartj/ehp285]
41 Fava AM,Xu B.Tricuspid valve endocarditis:Cardiovascular imaging evaluation and management.
2021;9:8974-8984[PMID:34786381 DOI:10.12998/wjcc.v9.i30.8974]
42 Oliveira M,Guittet L,Hamon M.Comparative Value of Cardiac CT and Transesophageal Echocardiography in Infective Endocarditis:A Systematic Review and Meta-Analysis.
2020;2:e190189[PMID:33778583 DOI:10.1148/ryct.2020190189]
43 Merlo A,Chen K,Deo S,Markowitz A.Does routine preoperative computed tomography imaging provide clinical utility in patients undergoing primary cardiac surgery?
2017;25:659-662[PMID:28962500 DOI:10.1093/icvts/ivx098]
44 Gulati M,Levy PD,Mukherjee D,Amsterdam E,Bhatt DL,Birtcher KK,Blankstein R,Boyd J,Bullock-Palmer RP,Conejo T,Diercks DB,Gentile F,Greenwood JP,Hess EP,Hollenberg SM,Jaber WA,Jneid H,Joglar JA,Morrow DA,O'Connor RE,Ross MA,Shaw LJ.2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain:Executive Summary:A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines.
2021;144:e368-e454[PMID:34709928 DOI:10.1161/CIR.0000000000001030]
45 SCOT-HEART investigators..CT coronary angiography in patients with suspected angina due to coronary heart disease(SCOT-HEART):an open-label,parallel-group,multicentre trial.
2015;385:2383-2391[PMID:25788230 DOI:10.1016/S0140-6736(15)60291-4]
46 SCOT-HEART Investigators.,Newby DE,Adamson PD,Berry C,Boon NA,Dweck MR,Flather M,Forbes J,Hunter A,Lewis S,MacLean S,Mills NL,Norrie J,Roditi G,Shah ASV,Timmis AD,van Beek EJR,Williams MC.Coronary CT Angiography and 5-Year Risk of Myocardial Infarction.
2018;379:924-933[PMID:30145934 DOI:10.1056/NEJMoa1805971]
47 Knuuti J,Ballo H,Juarez-Orozco LE,Saraste A,Kolh P,Rutjes AWS,Jüni P,Windecker S,Bax JJ,Wijns W.The performance of non-invasive tests to rule-in and rule-out significant coronary artery stenosis in patients with stable angina:a meta-analysis focused on post-test disease probability.
2018;39:3322-3330[PMID:29850808 DOI:10.1093/eurheartj/ehy267]
48 Opolski MP,Staruch AD,Jakubczyk M,Min JK,Gransar H,Staruch M,Witkowski A,Kepka C,Kim WK,Hamm CW,M?llmann H,Achenbach S.CT Angiography for the Detection of Coronary Artery Stenoses in Patients Referred for Cardiac Valve Surgery:Systematic Review and Meta-Analysis.
2016;9:1059-1070[PMID:27344418 DOI:10.1016/j.jcmg.2015.09.028]
49 Vahanian A,Beyersdorf F,Praz F,Milojevic M,Baldus S,Bauersachs J,Capodanno D,Conradi L,De Bonis M,De Paulis R,Delgado V,Freemantle N,Gilard M,Haugaa KH,Jeppsson A,Jüni P,Pierard L,Prendergast BD,Sádaba JR,Tribouilloy C,Wojakowski W;ESC/EACTS Scientific Document Group.2021 ESC/EACTS Guidelines for the management of valvular heart disease.
2022;43:561-632[PMID:34453165 DOI:10.1093/eurheartj/ehab395]50Hekimian G,Kim M,Passefort S,Duval X,Wolff M,Leport C,Leplat C,Steg G,Iung B,Vahanian A,Messika-Zeitoun D.Preoperative use and safety of coronary angiography for acute aortic valve infective endocarditis.
2010;96:696-700[PMID:20424151 DOI:10.1136/hrt.2009.183772]
51 Saby L,Laas O,Habib G,Cammilleri S,Mancini J,Tessonnier L,Casalta JP,Gouriet F,Riberi A,Avierinos JF,Collart F,Mundler O,Raoult D,Thuny F.Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis:increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion.
2013;61:2374-2382[PMID:23583251 DOI:10.1016/j.jacc.2013.01.092]
52 Wang TKM,Sánchez-Nadales A,Igbinomwanhia E,Cremer P,Griffin B,Xu B.Diagnosis of Infective Endocarditis by Subtype Using
F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography:A Contemporary Meta-Analysis.
2020;13:e010600[PMID:32507019 DOI:10.1161/CIRCIMAGING.120.010600]
53 Mahmood M,Kendi AT,Ajmal S,Farid S,O'Horo JC,Chareonthaitawee P,Baddour LM,Sohail MR.Meta-analysis of 18F-FDG PET/CT in the diagnosis of infective endocarditis.
2019;26:922-935[PMID:29086386 DOI:10.1007/s12350-017-1092-8]
54 Swart LE,Gomes A,Scholtens AM,Sinha B,Tanis W,Lam MGEH,van der Vlugt MJ,Streukens SAF,Aarntzen EHJG,Bucerius J,van Assen S,Bleeker-Rovers CP,van Geel PP,Krestin GP,van Melle JP,Roos-Hesselink JW,Slart RHJA,Glaudemans AWJM,Budde RPJ.Improving the Diagnostic Performance of
F-Fluorodeoxyglucose Positron-Emission Tomography/Computed Tomography in Prosthetic Heart Valve Endocarditis.
2018;138:1412-1427[PMID:30018167 DOI:10.1161/CIRCULATIONAHA.118.035032]
55 Erba PA,Conti U,Lazzeri E,Sollini M,Doria R,De Tommasi SM,Bandera F,Tascini C,Menichetti F,Dierckx RA,Signore A,Mariani G.Added value of 99mTc-HMPAO-labeled leukocyte SPECT/CT in the characterization and management of patients with infectious endocarditis.
2012;53:1235-1243[PMID:22787109 DOI:10.2967/jnumed.111.099424]
56 Rouzet F,Chequer R,Benali K,Lepage L,Ghodbane W,Duval X,Iung B,Vahanian A,Le Guludec D,Hyafil F.Respective performance of 18F-FDG PET and radiolabeled leukocyte scintigraphy for the diagnosis of prosthetic valve endocarditis.
2014;55:1980-1985[PMID:25453046 DOI:10.2967/jnumed.114.141895]
57 Di Salvo G,Habib G,Pergola V,Avierinos JF,Philip E,Casalta JP,Vailloud JM,Derumeaux G,Gouvernet J,Ambrosi P,Lambert M,Ferracci A,Raoult D,Luccioni R.Echocardiography predicts embolic events in infective endocarditis.
2001;37:1069-1076[PMID:11263610 DOI:10.1016/s0735-1097(00)01206-7]
58 Rossi SE,Goodman PC,Franquet T.Nonthrombotic pulmonary emboli.
2000;174:1499-1508[PMID:10845470 DOI:10.2214/ajr.174.6.1741499]
59 Huang JS,Ho AS,Ahmed A,Bhalla S,Menias CO.Borne identity:CT imaging of vascular infections.
2011;18:335-343[PMID:21424803 DOI:10.1007/s10140-011-0946-7]
60 Thuny F,Avierinos JF,Tribouilloy C,Giorgi R,Casalta JP,Milandre L,Brahim A,Nadji G,Riberi A,Collart F,Renard S,Raoult D,Habib G.Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis:a prospective multicentre study.
2007;28:1155-1161[PMID:17363448 DOI:10.1093/eurheartj/ehm005]
61 García-Cabrera E,Fernández-Hidalgo N,Almirante B,Ivanova-Georgieva R,Noureddine M,Plata A,Lomas JM,Gálvez-Acebal J,Hidalgo-Tenorio C,Ruíz-Morales J,Martínez-Marcos FJ,Reguera JM,de la Torre-Lima J,de Alarcón González A;Group for the Study of Cardiovascular Infections of the Andalusian Society of Infectious Diseases; Spanish Network for Research in Infectious Diseases.Neurological complications of infective endocarditis:risk factors,outcome,and impact of cardiac surgery:a multicenter observational study.
2013;127:2272-2284[PMID:23648777 DOI:10.1161/CIRCULATIONAHA.112.000813]
62 Heiro M,Nikoskelainen J,Engblom E,Kotilainen E,Marttila R,Kotilainen P.Neurologic manifestations of infective endocarditis:a 17-year experience in a teaching hospital in Finland.
2000;160:2781-2787[PMID:11025788 DOI:10.1001/archinte.160.18.2781]
 World Journal of Radiology2022年7期
World Journal of Radiology2022年7期
- World Journal of Radiology的其它文章
- Catheter-based renal sympathetic nerve denervation on hypertension management outcomes
- Type 2 dynamic curves:A diagnostic dilemma
- Radiological review of rhinocerebral mucormycosis cases during the COVID-19 Pandemic:A single-center experience
- Impact of X-radiation in the management of COVID-19 disease
- Molecular imaging as a tool for evaluation of COVID-19 sequelae–A review of literature