
Predictors for malignant potential and deep submucosal invasion in colorectal laterally spreading tumors
2022-07-16 05:51:58XiaoWenHaoPengLiYongJunWangMingJiShuTianZhangHaiYunShi
INTRODUCTION
Colorectal laterally spreading tumors (LSTs) are lesions 10 mm or greater in diameter characterized by lateral and circumferential extension with a low vertical axis along the colorectal wall[1]. LSTs are easily missed during colonoscopy and constitute an important contributor to post-colonoscopy colorectal cancer[2,3]. LSTs are morphologically categorized into the granular type (LST-G), which has a nodular surface, and non-granular type (LST-NG), which has a smooth surface[1,3]. The LST-G type can be divided into a granular nodular mixed subtype (G-NM) and homogeneous subtype (G-H), according to the existence of irregular and large nodules. The LST-NG type can be further subclassified into the nongranular pseudodepressed (NG-PD), presenting a gently sloping central depression, and the flat elevated subtype (NG-FE), characterized by a flat and smooth surface[1,3]. Although some studies have reported that the four subtypes of LSTs have varying clinicopathological features, previous analyses have not been adjusted for confounding factors, and the risk of deep submucosal invasion (SMI) and endoscopic resectability have not been evaluated[4-7].
Endoscopic resection is widely used to treat colorectal neoplasms with a negligible risk of lymph node metastasis.
resection is indicated for early colorectal cancer[8]. In Eastern countries, early colorectal cancer includes carcinoma
, tumors with a SMI depth less than 1000 μm (superficial SMI or T1a), and tumors with a SMI depth greater than 1000 μm (deep SMI or T1b)[9]. Given their high risk of lymph node metastasis, lesions with deep SMI are endoscopically unresectable and require surgery[10]. Endoscopic methods for achieving
resection includes endoscopic mucosal resection (EMR)(for lesions < 2 cm) and endoscopic submucosal dissection (ESD) (for larger lesions)[9,11]. ESD is also indicated when the likelihood of superficial SMI is high[8].
LSTs are good candidates for endoscopic resection owing to their low overall rate of SMI[3].However, each morphologic subtype of LSTs is associated with a distinct risk of SMI. Tumor size is known to have various additional effects on SMI among the four subtypes[1,3]. Therefore, morphologic subtype is the initial consideration when selecting treatments for LSTs. Risk stratification of carcinogenesis and invasiveness according to morphologic subtype in combination with other factors remains to be fully elucidated. The aim of our study was to determine the predictors for carcinoma, invasion depth and endoscopically unresectable lesions for colorectal LSTs and to perform risk assessments for each morphologic subtype.
MATERIALS AND METHODS
The endoscopic and histological results of consecutive patients who underwent ESD for colorectal LSTs at Beijing Friendship Hospital between June 2013 and March 2019 were retrospectively reviewed. In our centre, ESD is the standard treatment for LSTs. Patients with familial adenomatous polyposis or inflammatory bowel disease were excluded. This study was approved by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University.
Because of the retrospective nature of this study, decisions regarding study inclusion were made by two endoscopists after reviewing all colonoscopy findings. LSTs were defined as lesions ≥ 1 cm in diameter that extended laterally and circumferentially along the colorectal wall rather than perpendicular to it. All lesions were reviewed and classified by two endoscopists (Shi HY and Hao XW) using Kudo’s classification. All lesions were subclassified as follows:(1) G-NM subtype, which had a granular surface with giant nodules; (2) G-H subtype, which had an even granular surface; (3) NG-PD subtype,characterized by a mixture of elevated and depressed flat regions in each lesion; or (4) NG-FE subtype,exhibited an elevated flat and smooth surface[1].
Accurate preoperative assessment based on various risk factors to identify carcinoma and invasion depth is essential for selecting an appropriate therapeutic strategy.
This store is just blocks from Humboldt State University, and this late afternoon it was overrun by students dressed in creative costumes, carrying copious1 quantities of candy, chips, and beer in anticipation2 of Halloween parties they would soon be attending
Statistical analysis
Categorical variables were analysed using the
χ
test or Fisher’s exact test where appropriate.Continuous data were analysed using Student’s
test if they were normally distributed or the Mann-Whitney
test if they followed a skewed distribution. Variables found to be significant in univariate analysis were entered into multivariate logistic regression to determine the independent factors for carcinoma, SMI, deep SMI and endoscopically unresectable lesions. Two-sided
values < 0.05 were considered significant. Statistical analyses were performed with IBM SPSS Statistics 20.0.
RESULTS
Characteristics of the patients and lesions
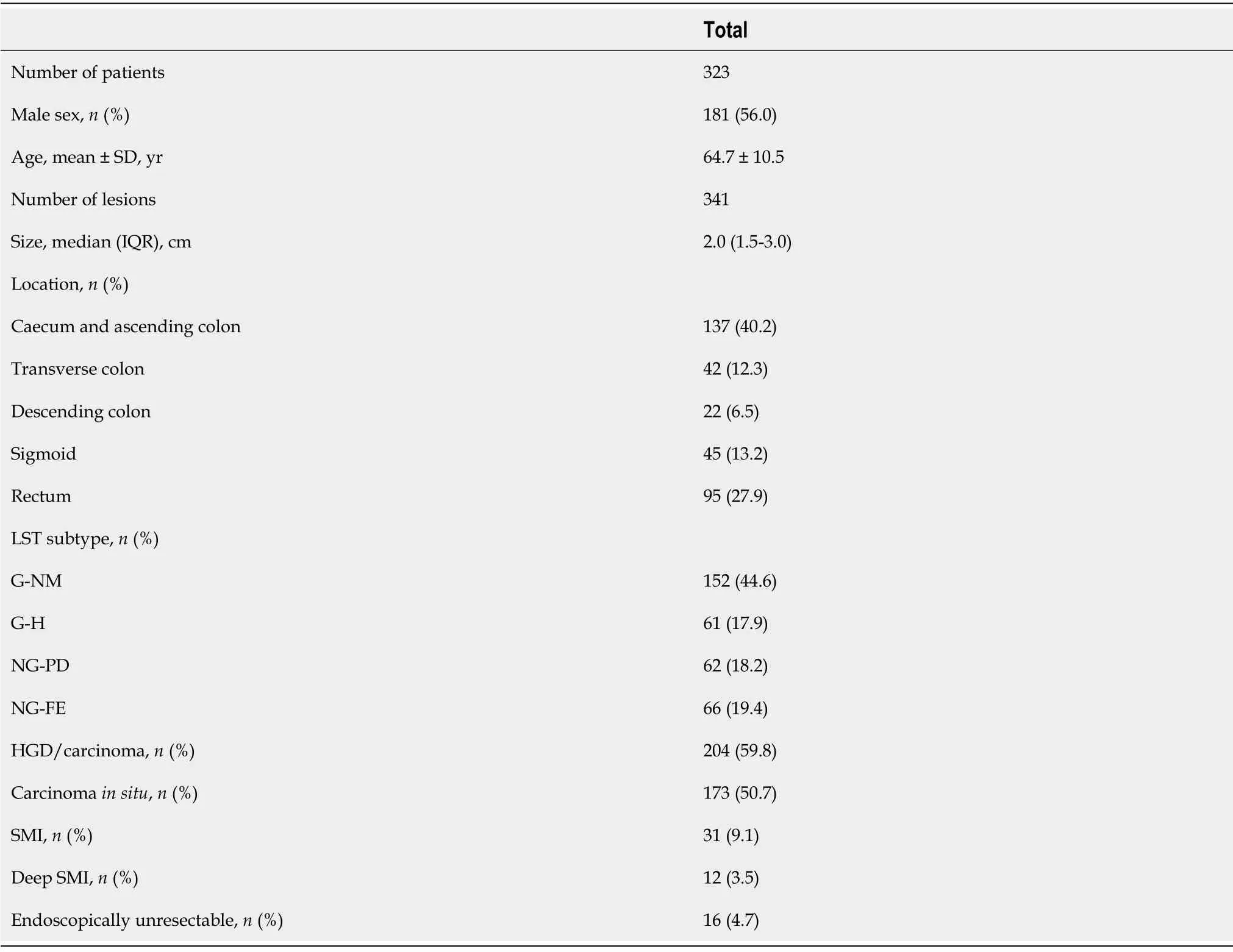
A total of 323 patients with 341 LSTs were included. The mean age was 64.7 years (range 26-88 years),and 56.0% were men. The median size of the lesions was 20 (range 10-100) mm. Most (52.5%) LSTs were located in the right colon, and 41.1% of the lesions were located in the rectosigmoid region. G-NM was the predominant subtype (44.6%). Up to 59.8% of the LSTs were carcinoma, among which 84.4%(173/204) were carcinoma
. The proportions of SMI, deep SMI and endoscopic unresectable lesions were 9.1%, 3.5% and 4.7%, respectively (Table 1).
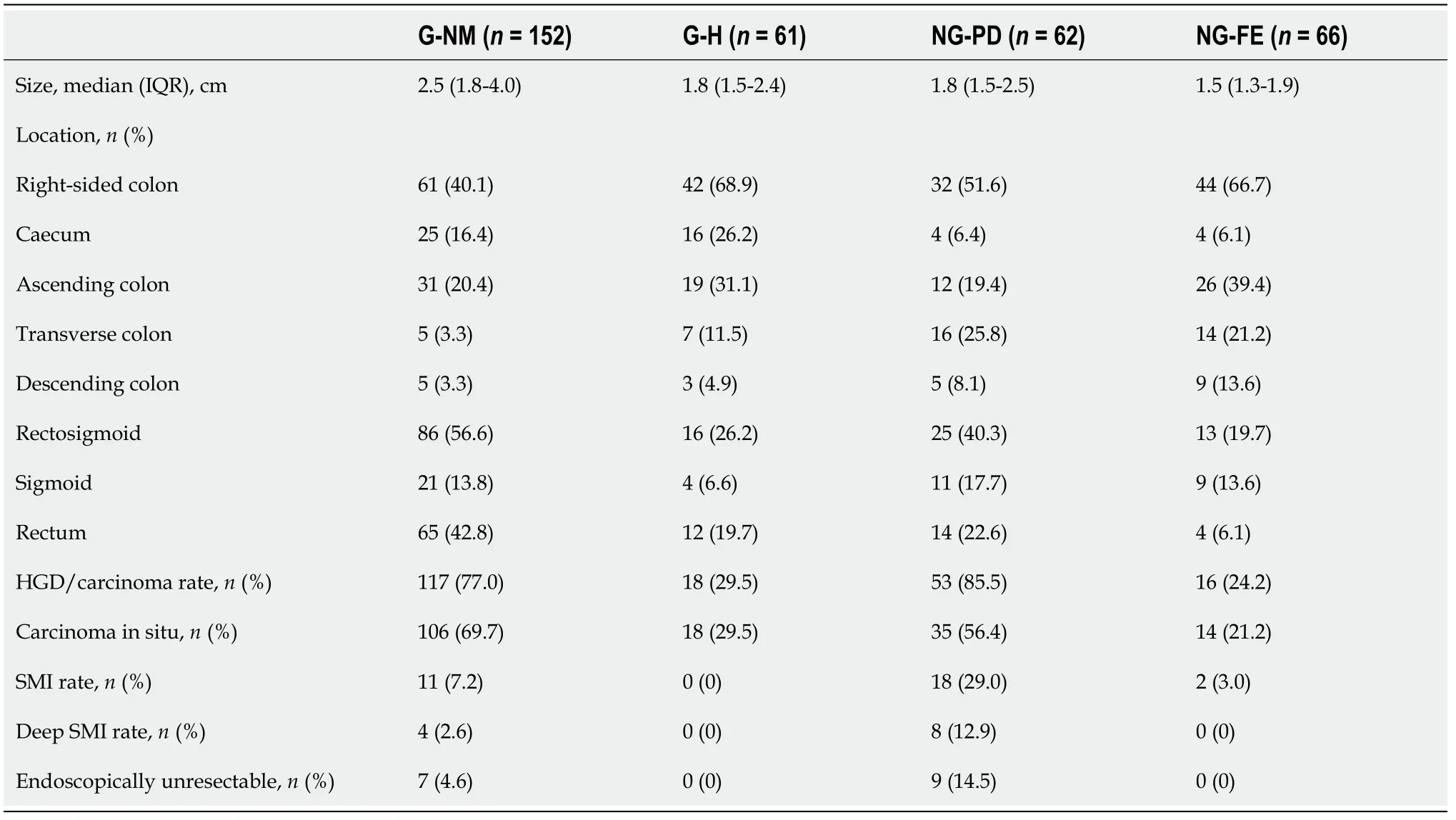
Comparisons among LST subtypes
Table 2 shows that the four LST subtypes had distinct clinicopathological features. G-NM [median 25 mm, interquartile range (IQR) 18-40 mm] was the largest subtype (
any of the other three subtypes,
< 0.001), and NG-FE (median 15 mm, IQR 13-19 mm) was the smallest subtype (
NG-PD subtype,
=0.009;
G-H subtype,
= 0.002). A higher percentage of the G-H (68.9%), NG-PD (51.6%) and NG-FE(66.7%) subtypes were located in the right colon, whereas the majority (56.6%) of the G-NM LSTs were located in the rectosigmoid region. The carcinoma rates of the G-NM and NG-PD LSTs were 77.0% and 85.5%, respectively, and both were significantly higher than those of the G-H (
29.5%,
< 0.001) and NG-FE (
24.2%,
< 0.001) LSTs. Of the tumors that were carcinoma, carcinoma
accounted for 90.6% (106/117), 100% (18/18), 66.0% (35/53) and 87.5% (14/16) of G-NM, G-H, NG-PD and NG-FE lesions, respectively. Among the four subtypes, the NG-PD subtype had the highest risk for having SMI(
any of the other three subtypes,
< 0.001), having deep SMI (12.9%
2.6% of the G-NM subtype,
= 0.004; 12.9%
0% of the G-H/NG-FE subtype,
= 0.002), and being endoscopically unresectable(14.5%
4.6% of the G-NM subtype,
= 0.016; 14.5%
0% of the G-H/NG-FE subtype,
= 0.001).
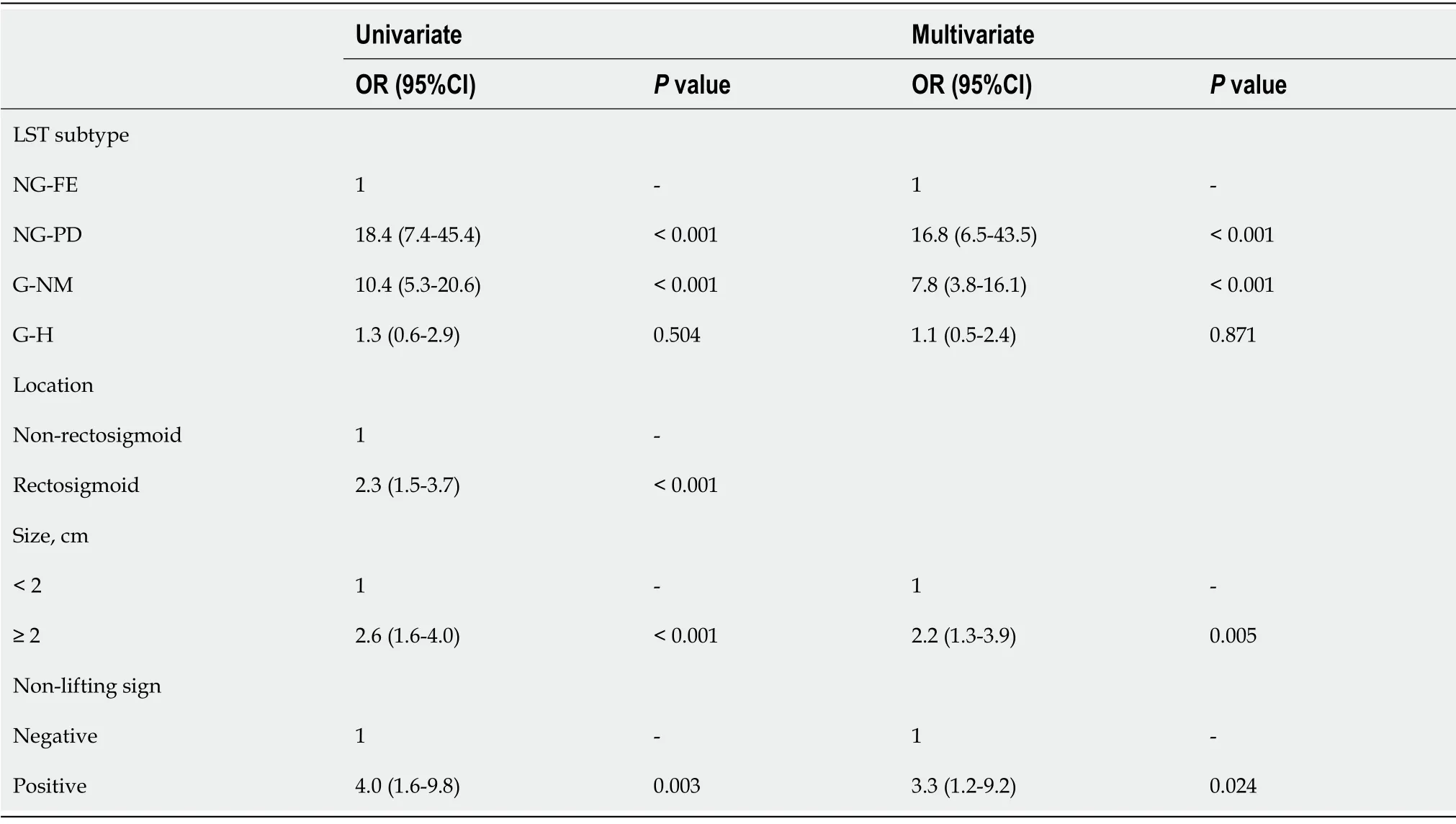
Predictors for carcinoma
As shown in Table 3, in univariate analysis, the G-NM subtype, NG-PD subtype, rectosigmoid location,size ≥ 2 cm, and positive non-lifting sign were associated with a higher risk for carcinoma. In the adjusted multivariate analysis, the G-NM subtype [odds ratio (OR) = 7.8, 95% confidence interval (CI):3.8-16.1,
< 0.001)], NG-PD subtype (OR = 16.8, 95%CI:6.5-43.5,
< 0.001), size ≥ 2 cm (OR = 2.2,95%CI:1.3-3.9,
= 0.005), and positive non-lifting sign (OR = 3.3, 95%CI:1.2-9.2,
= 0.024) remained independent predictors. We further performed subgroup analysis according to LST subtype. For the GNM subtype, a larger size was associated with a higher risk of carcinoma (85.1% of lesions ≥ 3 cm
70.6% of those < 3 cm,
= 0.035). Almost all (96.0%) of the NG-PD lesions located in the rectosigmoid region were carcinoma.
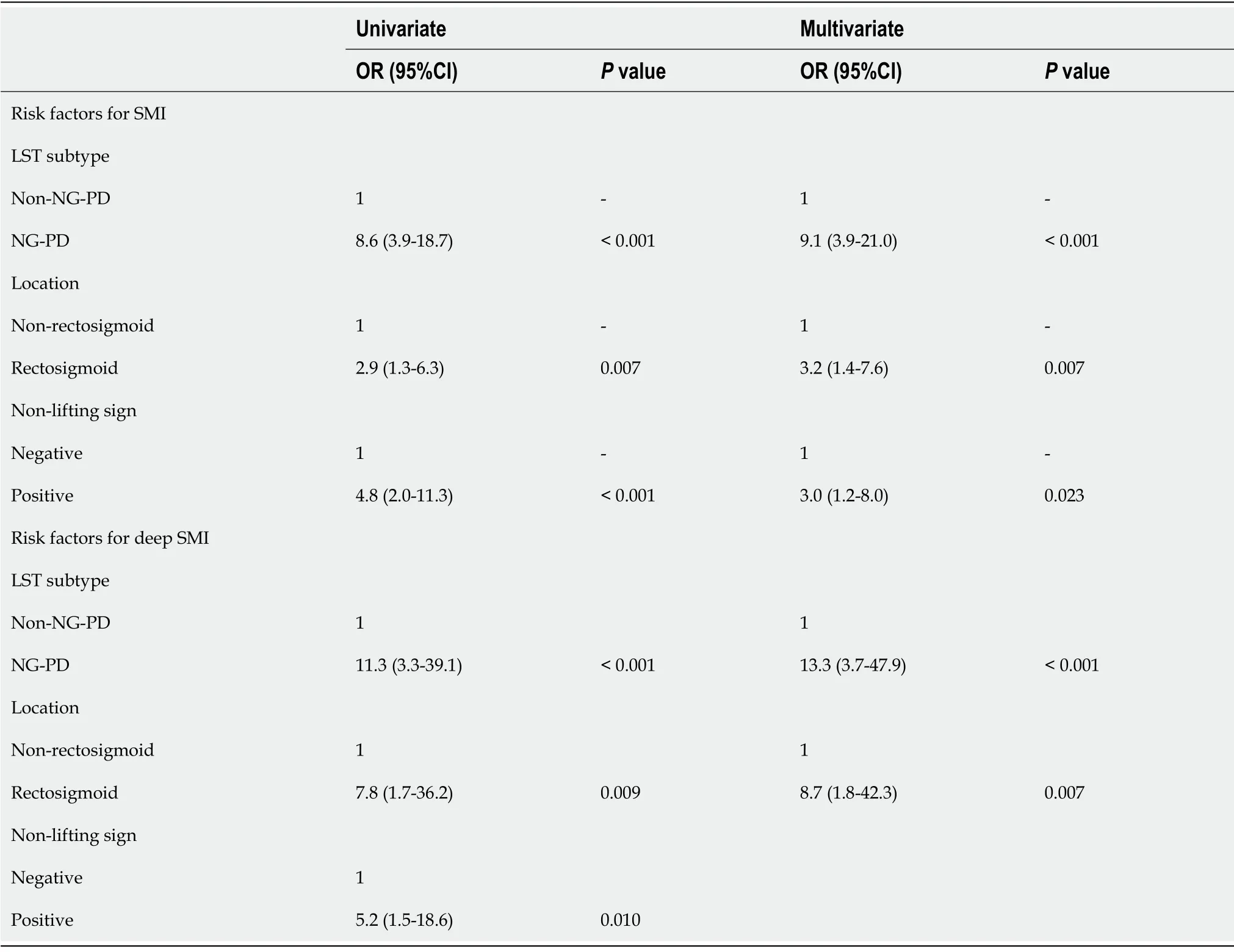
Predictors for SMI and deep SMI
The NG-PD subtype (OR = 9.1, 95%CI:3.9-21.0,
< 0.001), rectosigmoid location (OR = 3.2, 95%CI:1.4-7.6,
= 0.007), and positive non-lifting sign (OR = 3.0, 95%CI:1.2-8.0,
= 0.023) were independent predictive factors for SMI in the adjusted multivariate analysis (Table 4). The NG-PD subtype,rectosigmoid location and positive non-lifting sign were associated with an increased risk for deep SMI.In the adjusted multivariate analysis, the NG-PD subtype (OR = 13.3, 95%CI:3.7-47.9,
< 0.001) and rectosigmoid location (OR = 8.7, 95%CI:1.8-42.3,
= 0.007) were independent predictors for deep SMI(Table 4).
In the subgroup analysis by LST subtype, for the G-NM subtype, lesions located in the rectum were more likely to have SMI than those located in the colon (13.8%
2.3%,
= 0.009). None of the G-H lesions in our study invaded the submucosal layer. For the NG-PD subtype, 61.5% of LSTs with a positive non-lifting sign (
22.7% of those without a positive non-lifting sign,
= 0.015) had SMI. Deep SMI occurred in 44.4% of NG-PD lesions with a positive non-lifting sign (
9.3% of lesions without a non-lifting sign,
= 0.023) and 30.4% of those located in the rectosigmoid region (
3.0% of lesions located proximal to the sigmoid colon,
= 0.006). Kudo’s pit pattern type V (60.0%
0% of those with type I-IV pit patterns,
= 0.027) and JNET type 2B/3 (75.0%
0% of those with JNET type 1/2A,
=0.033) were associated with a significantly higher risk for deep SMI. For NG-FE lesions, a rectosigmoid location was associated with a higher risk of SMI (15.4%
0%,
= 0.036). None of the NG-FE LSTs in our study invaded the deep submucosal layer.
Then she brought out the young man, who explained how he was seeking for his palace, and that no man had been able to tell him where it was, so he had come to the wind
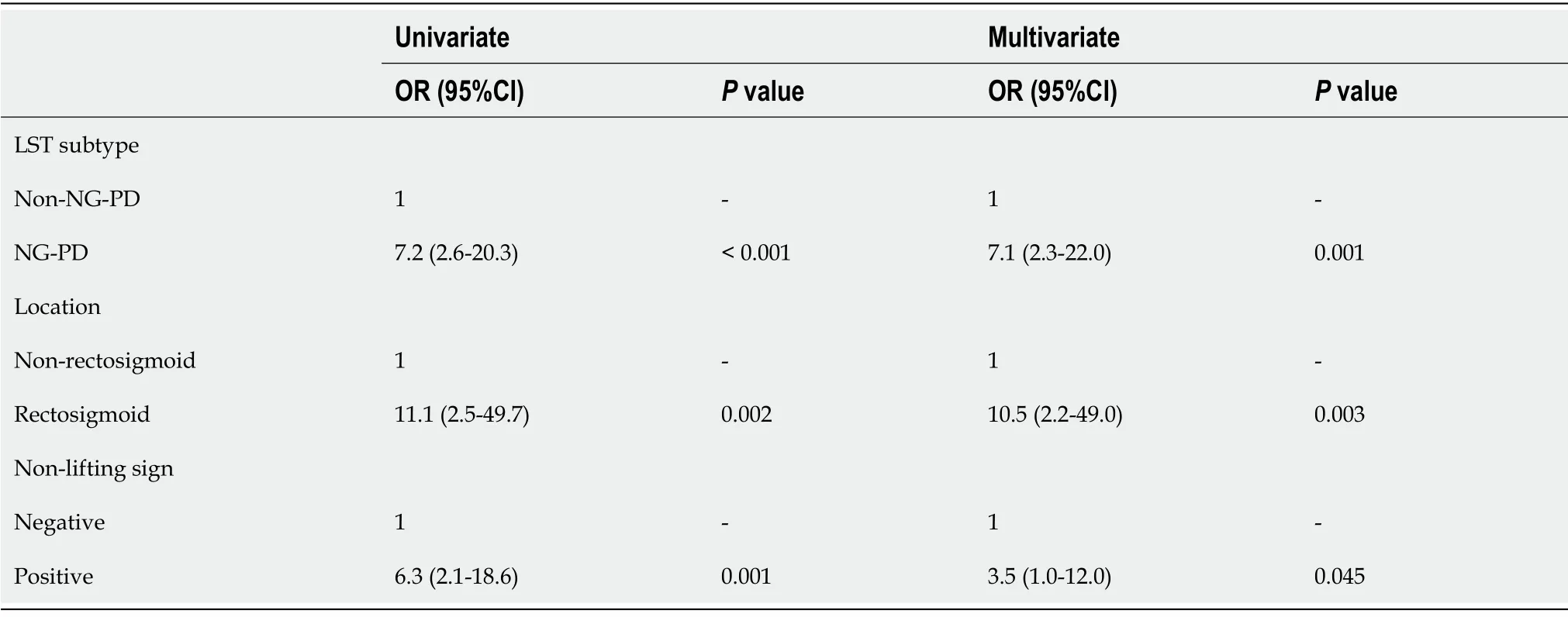
Predictors for endoscopically unresectable lesions
The NG-PD subtype (OR = 7.1, 95%CI:2.3-22.0,
= 0.001), rectosigmoid location (OR = 10.5, 95%CI:2.2-49.0,
= 0.003), and positive non-lifting sign (OR = 3.5, 95%CI:1.0-12.0,
= 0.045) were independent predictors for endoscopically unresectable lesions (Table 5). For the NG-PD subtype, 33.3% of the lesions in the rectosigmoid region (
3.0% of those located proximal to the sigmoid colon,
= 0.003)and 50.0% of the lesions with positive non-lifting signs (
9.3% of those without non-lifting signs,
=0.008) were endoscopically unresectable. The risk for being endoscopically unresectable was low in GNM LSTs. All of the G-H or NG-FE LSTs in our study were endoscopically resectable.
DISCUSSION
Our study revealed that the G-NM subtype, NG-PD subtype, size ≥ 2 cm and positive non-lifting sign were independent predictors for carcinoma. The NG-PD subtype, rectosigmoid location and positive non-lifting sign were independently associated with SMI and endoscopically unresectable lesions. We comprehensively compared the clinicopathological characteristics among the four subtypes of LSTs. GNM lesions had the largest tumor size among the four subtypes and most commonly occurred in the rectosigmoid region. Although a substantial proportion of carcinomas (77%) were found among G-NM LSTs, over 90% of the carcinomas were carcinomas
. Approximately 30% of the G-H LSTs were carcinomas, and all were carcinoma
. The NG-PD subtype was associated with the highest risks for being malignant (86%), having SMI (29%), having deep invasion (12.9%) and being endoscopically unresectable (16%) among the four subtypes. NG-FE LSTs had the smallest tumor size and a malignancy rate of approximately 25%. None of the malignant lesions considered the NG-FE subtype invaded the deep submucosal layer.
He looked at her reproachfully, and said: How can you ask me, cruel one? Are you not leaving me to my death perhaps? Ah! don t be so sorrowful, cried Beauty; I am only going to assure my father that I am safe and happy
An accurate preoperative diagnosis to identify carcinoma and determine the depth of invasion is essential for selecting an appropriate therapeutic strategy. We investigated independent factors for carcinoma, SMI, deep SMI and endoscopically unresectable lesions. The G-NM subtype, NG-PD subtype, large lesion size and positive non-lifting sign were predictors for carcinoma in our study,which was in line with previous studies[5-8,26]. For SMI, we found that the NG-PD subtype, positive non-lifting sign and rectosigmoid location were predictive factors. Although the NG-PD subtype and positive non-lifting sign are well acknowledged markers for SMI[5-8,21,26], the rectosigmoid location is a newly identified predictor for SMI. A large prospective multicentre study from Australia reported that rectosigmoid location was an independent factor for SMI, and the significance of this parameter remained among lesions without obvious high-risk features for SMI (type V Kudo pit pattern and Paris 0-IIc components)[27]. Rectal lesions accounted for a greater proportion of lesions with SMI in a few previous studies[4,28]. This may suggest different pathways of carcinogenesis between distal and proximal LSTs. Endoscopic resection of lesions located in the distal colorectum, particularly in the rectum, is technically easier and is associated with a lower risk of complications than that of lesions located in the proximal colon[29]. Endoscopically assessing the depth of SMI is extremely important in deciding whether to perform ESD or refer the patient to surgery. However, research investigating predictors for deep SMI is limited. Yamada
[30] reported that a depressed component was strongly associated with deep SMI both in LST-G and LST-NG. In our study, the NG-PD subtype and rectosigmoid location were also independent factors for deep SMI. We also confirmed that NG-PD,rectosigmoid location and positive non-lifting sign were independent factors for endoscopic unresectability. In addition to deep SMI, factors including lymphovascular invasion also determine endoscopic resectability. There were 4 cases of lymphovascular invasion on pathological examination without deep SMI in our study. The other risk factors for being endoscopically unresectable are very large lesion size(size > 40 mm), special location (lesions involving the ileocaecal valve, appendix, diverticulum), prior failed attempt at resection or recurrence at site of previous resection, and non-lifting sign after submucosal injection[31].
Several limitations of our study should be acknowledged. First, as this was a single-centre retrospective study based on clinical records, regional or institutional bias may exist. Second, because ESD was the commonly used treatment for LSTs in our centre and to allow for accurate histopathological assessment, only lesions that were resected
by ESD were included in this study; thus,there were no data on LSTs resected by EMR and surgery. However, the number of these lesions was relatively small. Third, it has previously been reported that magnifying observation (pit pattern diagnosis) and image-enhancement technology (
narrow band imaging) are reliable and effective methods for predicting the depth of tumor invasion; however, due to the inherent limitations of retrospective studies, some lesion records on JNET and Kudo pit pattern type were missing.
To the best of our knowledge, the present work is one of the largest studies comprehensively comparing the clinicopathological features, including risk of carcinoma, depth of invasion and endoscopic resectability, among the four subtypes of LSTs. With a relatively large number of cases involved, we were able to perform multivariate analyses and determine the independent predictors for carcinoma, SMI, deep SMI and endoscopic unresectability. Subgroup analyses were also conducted to identify distinct risks for the four subtypes of LSTs. We also proposed a treatment strategy for each subtype of LST, according to the risks of carcinoma and deep SMI based on our findings. Additionally,ESD is the standard therapy for LSTs in our centre and enables accurate pathological evaluation with detailed information on the depth of invasion and other risk factors for lymph node metastasis.
Now in the front row of the spectators sat the respected and popular Mayor of the village, who was much put out by what he considered nothing but a foolish trick
The risk of carcinoma, invasion depth and endoscopic unrespectability in each LST subtypes was further assessed. G-H LSTs are good candidates for EMR due to their relatively small tumor size and very low risk for SMI. For G-NM lesions, the overall rate of carcinoma was high, and this rate increased with as lesion size increased. A rectal location was associated with a high risk for SMI. Therefore,
resection is desirable for the G-NM subtype, whereas ESD is preferred for large lesions and those located in the rectum. NG-FE LSTs had a small tumor size and low overall risk for SMI. However, the risk for SMI increased significantly if the lesions were located in the rectosigmoid region, suggestingESD in such cases. A consensus has been reached that the NG-PD subtype is an indicator for ESD[8,11,32]. The high rate of SMI in our study supported this consensus. However, the NG-PD subtype is also associated with a high risk of being endoscopically unresectable. The decision between performing ESD and referring the patient to surgical treatment should be cautiously considered in this scenario. Our results showed that a rectosigmoid location, positive non-lifting sign and type V Kudo pit pattern were associated with a significantly higher risk for having deep SMI and being endoscopically unresectable.Before treating lesions with these risk features, the endoscopists’ experience and patients’ preferences should be cautiously considered. Despite improvements in endoscopic diagnosis, the sensitivity of endoscopic techniques for identifying SMI remains unsatisfactory[27]. In recent years,
ESD prior to surgery as a total excisional biopsy for early colorectal carcinoma has been introduced in clinical practice[33]. A recent multicentre study on the influence of preoperative ESD on the prognosis of patients with early colorectal carcinomas (T1) found that
ESD did not adversely affect the longterm clinical outcomes[34]. As a more cost-effective method than surgery, ESD is a reasonable first option for early colorectal carcinomas without obvious features of deep invasion.
CONCLUSION
In conclusion, the clinicopathological characteristics of LSTs varied according to subtypes in terms of size, distribution, malignant potential, depth of invasion and endoscopic resectability. Because of their increased risk for malignancy, it is highly recommended that NG-PD and G-NM LSTs are removed
through ESD. Given their substantial risk for deep SMI, surgery needs to be considered in NG-PD subtype LSTs located in the rectosigmoid, especially those with a positive non-lifting sign.
ARTICLE HIGHLIGHTS
Research background
Research motivation
In pathological evaluations, high-grade dysplasia was regarded as carcinoma
, according to the Japanese classification[9]. Carcinomas included carcinoma
and tumors with SMI. Lesions with a SMI depth ≥ 1000 μm were defined as having deep SMI. If the pathologic diagnosis was adenocarcinoma, in addition to invasion depth, the degree of carcinoma differentiation and tumor budding, as well as the presence of lymphovascular invasion, were evaluated. Endoscopically resectable lesions were defined as those without any of the following features:Poorly differentiated, deep SMI invasion,lymphovascular invasion, and high-grade tumor budding. Demographic and clinicopathologic data,including sex, age, LST subtype (G-NM, G-H, NG-PD, NG-FE), location, size, and pathological features,were recorded.
Research objectives
This study aimed to identify the predictors of carcinoma, invasion depth and endoscopically unresectable lesions for colorectal LSTs and to facilitate appropriate preoperative selection.
Research methods
This retrospective study analysed the endoscopic and histological results of consecutive patients who underwent ESD for colorectal LSTs in our hospital during a six-year period. The characteristics of the LSTs were compared by subtypes. Risk factors for high-grade dysplasia (HGD)/carcinoma and deep submucosal invasion (SMI) (invasion depth ≥ 1000 μm) were determined for each morphologic subtype.
Research results
Among the four subtypes, non-granular pseudodepressed (NG-PD) LSTs had the highest rate of HGD/carcinoma and deep SMI (invasion depth ≥ 1000 μm). NG-PD subtype and rectosigmoid location were the independent risk factors for deep SMI in adjusted multivariate analysis.
Research conclusions
We demonstrated that it is highly recommend that NG-PD and granular nodular mixed (G-NM) LSTs are removed through ESD; given their substantial risk for deep SMI, surgery needs to be considered in NG-PD LSTs located in the rectosigmoid, especially those with positive non-lifting signs.
Research perspectives
A risk score chart, which can determine the risk for carcinoma, invasion depth and endoscopically unresectable lesions for colorectal LSTs should be developed. It can help endoscopists in selective use of different types of endo-resection or to proceed to surgery instead of endoscopy.
The incidence of laterally spreading tumors (LSTs) is continually increasing; however, the optimal strategy for resecting large colorectal LSTs is still under debate. Endoscopic submucosal dissection(ESD) is associated with a high en bloc resection rate, low risk of recurrence and perfect pathological analysis. However, the possibility of a positive postoperative pathological resection margin exists,which would require additional surgical procedures. Surgery has a high complication rate, high mortality and prolonged hospital stays.
Large non-pedunculated colorectal lesions are traditionally managed by surgical resection[12]. Over the past decade, with the evolution of endoscopic techniques, endoscopic resection has become the firstline therapy for colorectal tumors without deep invasion[13,14]. Compared to surgery, endoscopic resection is associated with significantly lower rates of complications and a much quicker recovery[15-17]. Long-term outcomes including recurrence and survival rates are comparable between endoscopic and surgical treatment[8,18]. Furthermore, endoscopic resection has been shown to be more costeffective than surgery for the management of superficial colorectal neoplasms[19,20].
resection is indicated for carcinomatous lesions because of its superiority over piecemeal resection in reducing recurrence rates[8,9,21-23]. If superficial SMI is suspected, ESD is recommended to provide complete resection for accurate histological staging and reduced recurrence[8]. LSTs are good candidates forendoscopic resection due to their low risk for deep invasion[24,25]. In our study, approximately 60% of the LSTs were carcinomas, and the majority (approximately 85%) were carcinoma
.
Shi HY designed the research study and performed the data collection; Hao XW analyzed the data and wrote the first draft of the manuscript; Li P, Wang YJ, Ji M and Zhang ST performed the endoscopic therapies; Shi HY reviewed and edited the manuscript; and all authors read and approved the final manuscript.
A British man and his Spanish former sweetheart have finally married 16 years after they drifted apart, reunited by a love letter lost behind a fireplace1 for over a decade, reports said on Monday.
Beijing Nova Program, No. Z201100006820147; and Beijing Municipal Administration of Hospitals’Youth Program, No. QML20180102.
This study was approved by the Ethics Committee of Beijing Friendship Hospital (2020-P2-047-01) and was performed in accordance with the ethical guidelines of the 1975 Declaration of Helsinki.
It would be nice of you to make a poor fellow happy; therefore you may tell your father that it was I who slew9 the dragon, and if you refuse to, I will throw you into the river, and no one will be any the wiser, for they will think the dragon has devoured10 you
All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
All the authors report no relevant conflicts of interest for this article.
No additional data are available.
17.We will sit down and eat: Dummling passes the test that his brothers fail. Tater notes that a test of compassion posed early on in the tale determines whether the hero is eligible28 to carry out impossible tasks (284).Dummling s first reward is better food than what his mother gave him.Return to place in story.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
Mr. Alfred again spoke of Italy, and of the glorious colors inItalian scenery; the purple hills, the deep blue of the Mediterranean,the azure11 of southern skies, whose brightness and glory could onlybe surpassed in the north by the deep-blue eyes of a maiden12; and hesaid this with a peculiar13 intonation14; but she who should haveunderstood his meaning looked quite unconscious of it, which alsowas charming.
China
So she did what she was bid, and then her husband took the nyamatsane s liver from his pouch and said to her, There, I have brought you what you wanted, and now you know that I love you truly
Xiao-Wen Hao 0000-0003-1955-9325; Peng Li 0000-0003-2927-2758; Yong-Jun Wang 0000-0002-9584-7196; Ming Ji 0000-0002-2666-7423; Shu-Tian Zhang 0000-0003-2356-4397; Hai-Yun Shi 0000-0002-2084-8370.
Wang JJ
But that evening when they got home Curdken went to the old King, and said: I refuse to herd17 geese any longer with that girl. For what reason? asked the old King. Because she does nothing but annoy me all day long, replied Curdken; and he proceeded to relate all her iniquities27, and said: Every morning as we drive the flock through the dark gate she says to a horse s head that hangs on the wall:
The dolphins sported in the waves, and the great whales spouted29 water from their nostrils30 till it seemed as if a hundred fountains were playing in every direction
A
Wang JJ
1 Kudo Se, Lambert R, Allen JI, Fujii H, Fujii T, Kashida H, Matsuda T, Mori M, Saito H, Shimoda T, Tanaka S, Watanabe H, Sung JJ, Feld AD, Inadomi JM, O'Brien MJ, Lieberman DA, Ransohoff DF, Soetikno RM, Triadafilopoulos G, Zauber A, Teixeira CR, Rey JF, Jaramillo E, Rubio CA, Van Gossum A, Jung M, Vieth M, Jass JR, Hurlstone PD. Nonpolypoid neoplastic lesions of the colorectal mucosa.
2008; 68:S3-47 [PMID:18805238 DOI:10.1016/j.gie.2008.07.052]
2 Sanduleanu S, Masclee AM, Meijer GA. Interval cancers after colonoscopy-insights and recommendations.
2012; 9:550-554 [PMID:22907162 DOI:10.1038/nrgastro.2012.136]
3 Kudo SE, Takemura O, Ohtsuka K. Flat and depressed types of early colorectal cancers:from East to West.
2008; 18:581-593, xi [PMID:18674705 DOI:10.1016/j.giec.2008.05.013]
4 Kim BC, Chang HJ, Han KS, Sohn DK, Hong CW, Park JW, Park SC, Choi HS, Oh JH. Clinicopathological differences of laterally spreading tumors of the colorectum according to gross appearance.
2011; 43:100-107 [PMID:21165823 DOI:10.1055/s-0030-1256027]
5 Zhao X, Zhan Q, Xiang L, Wang Y, Wang X, Li A, Liu S. Clinicopathological characteristics of laterally spreading colorectal tumor.
2014; 9:e94552 [PMID:24751926 DOI:10.1371/journal.pone.0094552]
6 Cong ZJ, Hu LH, Ji JT, Xing JJ, Shan YQ, Li ZS, Yu ED. A long-term follow-up study on the prognosis of endoscopic submucosal dissection for colorectal laterally spreading tumors.
2016; 83:800-807 [PMID:26341853 DOI:10.1016/j.gie.2015.08.043]
7 Myung DS, Kweon SS, Lee J, Shin IS, Kim SW, Seo GS, Kim HS, Joo YE. Clinicopathological features of laterally spreading colorectal tumors and their association with advanced histology and invasiveness:An experience from Honam province of South Korea:A Honam Association for the Study of Intestinal Diseases (HASID).
2017; 12:e0184205 [PMID:28977010 DOI:10.1371/journal.pone.0184205]
8 Tanaka S, Kashida H, Saito Y, Yahagi N, Yamano H, Saito S, Hisabe T, Yao T, Watanabe M, Yoshida M, Saitoh Y,Tsuruta O, Sugihara KI, Igarashi M, Toyonaga T, Ajioka Y, Kusunoki M, Koike K, Fujimoto K, Tajiri H. Japan Gastroenterological Endoscopy Society guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection.
2020; 32:219-239 [PMID:31566804 DOI:10.1111/den.13545]
9 Nishimura M, Saito Y, Nakanishi Y, Shia J, Lauwers GY, Wallace MB. Pathology definitions and resection strategies for early colorectal neoplasia:Eastern
Western approaches in the post-Vienna era.
2020; 91:983-988 [PMID:31874160 DOI:10.1016/j.gie.2019.12.021]
10 Bosch SL, Teerenstra S, de Wilt JH, Cunningham C, Nagtegaal ID. Predicting lymph node metastasis in pT1 colorectal cancer:a systematic review of risk factors providing rationale for therapy decisions.
2013; 45:827-834 [PMID:23884793 DOI:10.1055/s-0033-1344238]
11 Draganov PV, Wang AY, Othman MO, Fukami N. AGA Institute Clinical Practice Update:Endoscopic Submucosal Dissection in the United States.
2019; 17:16-25.e1 [PMID:30077787 DOI:10.1016/j.cgh.2018.07.041]
12 Bronzwaer MES, Koens L, Bemelman WA, Dekker E, Fockens P; COPOS study group. Volume of surgery for benign colorectal polyps in the last 11 years.
2018; 87:552-561.e1 [PMID:29108978 DOI:10.1016/j.gie.2017.10.032]
13 Hassan C, Repici A, Sharma P, Correale L, Zullo A, Bretthauer M, Senore C, Spada C, Bellisario C, Bhandari P, Rex DK.Efficacy and safety of endoscopic resection of large colorectal polyps:a systematic review and meta-analysis.
2016;65:806-820 [PMID:25681402 DOI:10.1136/gutjnl-2014-308481]
14 Fukami N. Surgery Versus Endoscopic Mucosal Resection Versus Endoscopic Submucosal Dissection for Large Polyps:Making Sense of When to Use Which Approach.
2019; 29:675-685 [PMID:31445690 DOI:10.1016/j.giec.2019.06.007]
15 Kiriyama S, Saito Y, Yamamoto S, Soetikno R, Matsuda T, Nakajima T, Kuwano H. Comparison of endoscopic submucosal dissection with laparoscopic-assisted colorectal surgery for early-stage colorectal cancer:a retrospective analysis.
2012; 44:1024-1030 [PMID:23012216 DOI:10.1055/s-0032-1310259]
16 Ahlenstiel G, Hourigan LF, Brown G, Zanati S, Williams SJ, Singh R, Moss A, Sonson R, Bourke MJ; Australian Colonic Endoscopic Mucosal Resection (ACE) Study Group. Actual endoscopic
predicted surgical mortality for treatment of advanced mucosal neoplasia of the colon.
2014; 80:668-676 [PMID:24916925 DOI:10.1016/j.gie.2014.04.015]
17 Dang H, de Vos Tot Nederveen Cappel WH, van der Zwaan SMS, van den Akker-van Marle ME, van Westreenen HL,Backes Y, Moons LMG, Holman FA, Peeters KCMJ, van der Kraan J, Langers AMJ, Lijfering WM, Hardwick JCH,Boonstra JJ. Quality of life and fear of cancer recurrence in T1 colorectal cancer patients treated with endoscopic or surgical tumor resection.
2019; 89:533-544 [PMID:30273589 DOI:10.1016/j.gie.2018.09.026]
18 Heo J, Jeon SW, Jung MK, Kim SK, Kim J, Kim S. Endoscopic resection as the first-line treatment for early colorectal cancer:comparison with surgery.
2014; 28:3435-3442 [PMID:24962854 DOI:10.1007/s00464-014-3618-3]
19 Jayanna M, Burgess NG, Singh R, Hourigan LF, Brown GJ, Zanati SA, Moss A, Lim J, Sonson R, Williams SJ, Bourke MJ. Cost Analysis of Endoscopic Mucosal Resection
Surgery for Large Laterally Spreading Colorectal Lesions.
2016; 14:271-8.e1 [PMID:26364679 DOI:10.1016/j.cgh.2015.08.037]
20 Law R, Das A, Gregory D, Komanduri S, Muthusamy R, Rastogi A, Vargo J, Wallace MB, Raju GS, Mounzer R, Klapman J, Shah J, Watson R, Wilson R, Edmundowicz SA, Wani S. Endoscopic resection is cost-effective compared with laparoscopic resection in the management of complex colon polyps:an economic analysis.
2016; 83:1248-1257 [PMID:26608129 DOI:10.1016/j.gie.2015.11.014]
21 Chen T, Qin WZ, Yao LQ, Zhong YS, Zhang YQ, Chen WF, Hu JW, Ooi M, Chen LL, Hou YY, Xu MD, Zhou PH. Longterm outcomes of endoscopic submucosal dissection for high-grade dysplasia and early-stage carcinoma in the colorectum.
2018; 38:3 [PMID:29764504 DOI:10.1186/s40880-018-0273-4]
22 Belderbos TD, Leenders M, Moons LM, Siersema PD. Local recurrence after endoscopic mucosal resection of nonpedunculated colorectal lesions:systematic review and meta-analysis.
2014; 46:388-402 [PMID:24671869 DOI:10.1055/s-0034-1364970]
23 Saunders BP, Tsiamoulos ZP. Endoscopic mucosal resection and endoscopic submucosal dissection of large colonic polyps.
2016; 13:486-496 [PMID:27353401 DOI:10.1038/nrgastro.2016.96]
24 Bogie RMM, Veldman MHJ, Snijders LARS, Winkens B, Kaltenbach T, Masclee AAM, Matsuda T, Rondagh EJA,Soetikno R, Tanaka S, Chiu HM, Sanduleanu-Dascalescu S. Endoscopic subtypes of colorectal laterally spreading tumors(LSTs) and the risk of submucosal invasion:a meta-analysis.
2018; 50:263-282 [PMID:29179230 DOI:10.1055/s-0043-121144]
25 Bae JH, Yang DH, Lee JY, Soh JS, Lee S, Lee HS, Lee HJ, Park SH, Kim KJ, Ye BD, Myung SJ, Yang SK, Kim JH,Byeon JS. Clinical outcomes of endoscopic submucosal dissection for large colorectal neoplasms:a comparison of protruding and laterally spreading tumors.
2016; 30:1619-1628 [PMID:26169642 DOI:10.1007/s00464-015-4392-6]
26 Kim KO, Jang BI, Jang WJ, Lee SH. Laterally spreading tumors of the colorectum:clinicopathologic features and malignant potential by macroscopic morphology.
2013; 28:1661-1666 [PMID:23934010 DOI:10.1007/s00384-013-1741-6]
27 Burgess NG, Hourigan LF, Zanati SA, Brown GJ, Singh R, Williams SJ, Raftopoulos SC, Ormonde D, Moss A, Byth K,Mahajan H, McLeod D, Bourke MJ. Risk Stratification for Covert Invasive Cancer Among Patients Referred for Colonic Endoscopic Mucosal Resection:A Large Multicenter Cohort.
2017; 153:732-742.e1 [PMID:28583826 DOI:10.1053/j.gastro.2017.05.047]
28 Miyamoto H, Ikematsu H, Fujii S, Osera S, Odagaki T, Oono Y, Yano T, Ochiai A, Sasaki Y, Kaneko K.Clinicopathological differences of laterally spreading tumors arising in the colon and rectum.
2014; 29:1069-1075 [PMID:24986136 DOI:10.1007/s00384-014-1931-x]
29 Ma MX, Bourke MJ. Complications of endoscopic polypectomy, endoscopic mucosal resection and endoscopic submucosal dissection in the colon.
2016; 30:749-767 [PMID:27931634 DOI:10.1016/j.bpg.2016.09.009]
30 Yamada M, Saito Y, Sakamoto T, Nakajima T, Kushima R, Parra-Blanco A, Matsuda T. Endoscopic predictors of deep submucosal invasion in colorectal laterally spreading tumors.
2016; 48:456-464 [PMID:26919264 DOI:10.1055/s-0042-100453]
31 Rutter MD, Chattree A, Barbour JA, Thomas-Gibson S, Bhandari P, Saunders BP, Veitch AM, Anderson J, Rembacken BJ, Loughrey MB, Pullan R, Garrett WV, Lewis G, Dolwani S. British Society of Gastroenterology/Association of Coloproctologists of Great Britain and Ireland guidelines for the management of large non-pedunculated colorectal polyps.
2015; 64:1847-1873 [PMID:26104751 DOI:10.1136/gutjnl-2015-309576]
32 Pimentel-Nunes P, Dinis-Ribeiro M, Ponchon T, Repici A, Vieth M, De Ceglie A, Amato A, Berr F, Bhandari P, Bialek A,Conio M, Haringsma J, Langner C, Meisner S, Messmann H, Morino M, Neuhaus H, Piessevaux H, Rugge M, Saunders BP, Robaszkiewicz M, Seewald S, Kashin S, Dumonceau JM, Hassan C, Deprez PH. Endoscopic submucosal dissection:European Society of Gastrointestinal Endoscopy (ESGE) Guideline.
2015; 47:829-854 [PMID:26317585 DOI:10.1055/s-0034-1392882]
33 Asayama N, Oka S, Tanaka S, Hayashi N, Arihiro K, Chayama K. Endoscopic submucosal dissection as total excisional biopsy for clinical T1 colorectal carcinoma.
2015; 91:64-69 [PMID:25632920 DOI:10.1159/000368866]
34 Yamashita K, Oka S, Tanaka S, Nagata S, Hiraga Y, Kuwai T, Furudoi A, Tamura T, Kunihiro M, Okanobu H, Nakadoi K, Kanao H, Higashiyama M, Kuraoka K, Shimamoto F, Chayama K. Preceding endoscopic submucosal dissection for T1 colorectal carcinoma does not affect the prognosis of patients who underwent additional surgery:a large multicenter propensity score-matched analysis.
2019; 54:897-906 [PMID:31104172 DOI:10.1007/s00535-019-01590-w]
 World Journal of Gastrointestinal Oncology2022年7期
World Journal of Gastrointestinal Oncology2022年7期
- World Journal of Gastrointestinal Oncology的其它文章
- Da Vinci robot-assisted pancreato-duodenectomy in a patient with situs inversus totalis:A case report and review of literature
- Correction to “Novel long non-coding RNA LINC02532 promotes gastric cancer cell proliferation, migration, and invasion in vitro”
- Primary signet-ring cell carcinoma of the extrahepatic bile duct:A case report
- Pediatric case of colonic perivascular epithelioid cell tumor complicated with intussusception and anal incarceration:A case report
- Effect of obesity on post-operative outcomes following colorectal cancer surgery
- Neutrophile-to-lymphocyte, lymphocyte-to-monocyte, and platelet-tolymphocyte ratios as prognostic and response biomarkers for resectable locally advanced gastric cancer