
Tuberculosis conundrum - current and future scenarios: A proposed comprehensive approach combining laboratory, imaging, and computing advances
2022-07-02 08:44:58SulemanAdamMerchantMohdJavedSaifullahShaikhPrakashNadkarni
World Journal of Radiology 2022年6期
lNTRODUCTlON
Nearly 1.5 centuries after Robert Koch discovered
(MTB) in 1882, tuberculosis (TB) remains a global threat and a deadly human pathogen, ubiquitous enough to comprise an occupational hazard for medical personnel in many locales. Its high prevalence in both immunocompetent and immunocompromised individuals historically made TB a top-10 cause of death worldwide and the leading cause of death from a single infectious agent, though it fell to 13
after being overtaken by COVID-19 in 2021[1]. 95% of cases and deaths occur in developing countries. About one-quarter of the world's population has a TB infection, though most are not (yet) symptomatic and contagious[2]. Because people with active TB can infect 5-15 other people through close contact over a single year, the consequence of delayed/missed diagnosis cascade[2]. However, TB is curable and preventable[2].
The incessant rise of Multidrug-resistant TB (MDR-TB) and extensively drug-resistant (XDR) TB, either primary or acquired, pose an additional challenge[3,4]. Incidence of either varies in different studies: More concerning, only 1/3
of such individuals accessed treatment in 2020[2].
The next fall, after watching a football game on television, Tom asked, Dad, remember that football you have in the garage? Can I use it to play with the guys now? Eyes rolling up in my head, I replied, Tom, you don t understand
The three countries with the largest share of the global burden in 2019 were India (27%, 2.8 million cases annually, 150,000 MDR-TB cases every year), China (14%), and the Russian Federation (8%)[5,6]. In 2020, an estimated 10 million people fell ill with TB worldwide. The largest number of new TB cases occurred in the WHO South-East Asian Region (43%), African Region (25%), and Western Pacific (18%)[2]. In descending case-count order, eight countries account for two thirds of the total: India, China, Indonesia, the Philippines, Pakistan, Nigeria, Bangladesh, and South Africa[2].
Ending the TB epidemic by 2030 is among the health targets of the United Nations Sustainable Development Goals[2]. The End TB Strategy defines five-yearly milestones/targets for reducing TB cases and deaths. The targets for 2030 are a 90% reduction in TB deaths and an 80% reduction in new cases per year, compared with levels in 2015, with a reduction in new cases to < 1 per million population annually by 2050[7,8].
DlAGNOSlS OF TB
MDR-TB: Advances in laboratory diagnosis
MDR-TB is defined as an infection with MTB strains non-responsive to isoniazid (INH) and rifampicin (RIF), the 2 most effective first-line anti-TB drugs. Mutations in the INH and RIF resistance gene confers high competitive fitness, favoring their spread: >90% of RIF-resistant strains are also INH-resistant[9-11]. Most people develop MDR-TB because of delayed or incomplete treatment, increasing subsequent healthcare costs dramatically[12]. MDR-TB is curable with second-line drugs: In 2018, the treatment success rate of MDR-TB patients was 59% worldwide. The earlier treatment regimens for up to 2 years have been superseded by WHO’s updated (2021) recommendation for shorter (9-11 mo) and fully oral regimens, which increase compliance greatly[2,13,14]. Previously laboratory confirmation of TB by culture required 6-8 wk: Diagnosing MDR-TB, which used to be exclusively clinical, involved delays of up to 4 mo to identify therapeutic response failure; coupled with persistently positive sputum smears after 4 mo of regular treatment with a first-line DOTS (Directly Observed Treatment, Short-course Regimen)[15-17]. Such therapeutic setbacks especially impacted impoverished or illiterate patients psychologically: after expecting a treatment duration of 7-9 mo only, to be informed halfway through that a new regimen was necessary, they often stopped treatment and were lost to follow-up, eventually spreading MDR-TB to others, exponentially. The spread of MDR-TB was also worsened by policies of using the much cheaper ‘regular TB’ drug regimen empirically: Treating MDR-TB is 5-200 times more expensive than treating nondrug resistant TB[18].
However, PCR based technologies such as cartridge based nucleic acid amplification techniques [CBNAAT] (GeneXpert
, Cepheid United States, introduced in 2010), can now rapidly detect both MTB genetic material from sputum samples and RIF resistance within 2 h using the current generation of technology, without requiring special technicians/rooms and barely occupying the space of a computer printer, at a cost of $5/test[19,12]. This has been called the most exciting innovation in TB diagnostics in over a century[12]. It is recommended by WHO, which developed policies/guidelines and monitoring frameworks for its use to support developing countries’ Ministries of Health (MOHs) in their implementation[12,20]. The latest GeneXpert technology (MTB/RIF Ultra) has a ten-fold improvement in the lower limit of TB detection, and improves differentiation of certain silent mutations, RIF resistance detection in mixed infections (in 3-7 d), increased specificity in detecting RIF resistance in paucibacillary specimens, and better sensitivity in both pulmonary samples and extrapulmonary samples such as pleural/ascitic fluid and biopsied material such as lymph nodes[12,19,21-23]. Our group were amongst the first to successfully use it for lymph nodes and also to recommend the same being used to detect MDR TB upfront.
TB-QUICK is a recent ultrasensitive MTB detection platform which combines loop-mediated isothermal amplification and clustered regularly interspaced short palindromic repeats (CRISPR)-Cas12b reaction for M TB detection. It is highly sensitive (with a near single-copy sensitivity), requires less sample input and offers even a shorter turnaround time than Gene-Xpert for RIF resistance[24].
We discuss these advances under two broad categories, software (
, Artificial Intelligence, Augmented and Virtual Reality) as well as Hardware Innovations.
Overall, TB, either incident or prevalent, is found in 4.1% of the MDR-TB contacts, which is higher than the corresponding prevalence rates of 1.9% and 1.7% reported among household contacts of drugsusceptible TB in the same locality[26,27]. In a study it was shown that RFLP analysis confirmed the transmission of MDR-TB among household contacts while regression analysis showed XDR-TB had an even higher risk of household transmission among all MDR-TB cases[28]. We have successfully used CBNAAT to diagnose extrapulmonary TB, and feel this has tremendous potential to revolutionize TB, especially MDR-TB early diagnosis, treatment, and further management. Piatek
[12] and Mechal
[23] have independently reported the same.
National TB control programs are working to eliminate TB mainly by intensifying efforts to find and cure patients with active disease. Mathematical models developed by Dye and Williams[29] suggest that, while most TB patients can be cured with present drug regimens, the 2050 target is far more likely to be achieved with a synergistic combination of diagnostics, drugs, and vaccines to detect and treat both latent infection and active disease.
lMAGlNG METHODS lN TUBERCULOSlS
Note: While interventional radiology plays a major role in TB treatment, we deliberately limit this review’s scope to diagnostic/prognostic imaging.
TB has a known propensity for dissemination from its primary site and can affect virtually any organ system in the body. It therefore demonstrates a variety of clinical and radiologic findings and can mimic numerous other diseases[30]. Hence, the role of imaging in TB has grown exponentially. The possibility of TB is often first suggested on an imaging study, particularly in relatively inaccessible sites.
In a known case of TB, imaging is often requested to assess the extent of disease, evaluate response to therapy, or detect residual infection after completion of anti-TB therapy. Imaging is also vital in guiding aspiration biopsies, therapeutic drainage of collections of pathological fluid
[31]. Hence, Radiologists will continue to play a vital role in eliminating TB.
Imaging findings in TB depend upon the extent of the disease process. Familiarity with various imaging features permits early diagnosis and prompt management, thereby reducing patient morbidity[30].
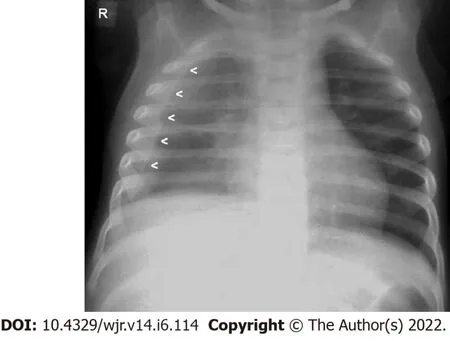
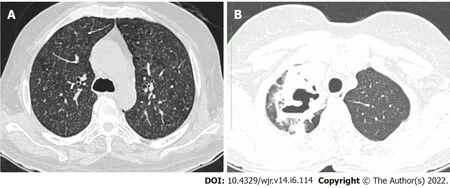
The TB Primary Complex (Ghon’s focus, draining lymphatics and hilar node/s) is very common in developing countries. However, inexperienced radiologists find it challenging to identify it in children on CXR, partly because the relatively prominent pulmonary arteries obscure the hila. However, cooccurrence of pleural effusion simplifies identification, because “classical” pleural effusions, especially of the lamellar type (tracking along the pleura, mimicking pleural thickening) (Figure 1) are relatively uncommon in children due to non-TB causes. A Childhood TB diagnosis algorithm using this information would gain in specificity. Similar considerations apply to Adult TB. Patients with “Open Kochs” (lung cavities or smear positive) (Figure 7B) are far more contagious and require isolation: including these factors in analysis/algorithms enables more effective screening/control/management[27].
Conventional Chest radiography
His mother then said, You know, what we have here is a failed experiment in how to effectively carry a big milk bottle with two tiny hands. Let s go out in the back yard and fill the bottle with water and see if you can discover a way to carry it without dropping it. The little boy learned7 that if he grasped the bottle at the top near the lip with both hands, he could carry it without dropping it. What a wonderful lesson!
After that he went a step further and began to have long talks with the Princess--still, however, keeping himself invisible, until she begged him so earnestly to appear to her that he could no longer resist, and after making her promise that, no matter what he was like, she would still love him, he drew the ring from his finger, and the Princess saw with delight that he was as handsome as he was agreeable
Ultrasonography
Ultrasonography (US) is one of the commonest recommended examinations for TB, including in the evaluation of suspected/affected lymph nodes and for guiding biopsies for the same. Basic details are well known and beyond the scope of this manuscript. It is a very useful non-invasive examination method in children including those with cervical lymphadenitis (across age groups). The US signs of hilar absence, short to long axis (S/L) ratio ≥ 0.5, an unclear edge, necrosis, an echogenic thin layer, strong echoes and capsular or peripheral vascularity; may aid in the diagnosis of cervical tuberculous lymphadenitis[35]. Endobronchial US-guided fine-needle aspiration biopsy for intrathoracic TB lymphadenopathy is valuable when bronchoalveolar lavage and sputum culture are ambiguous[36].
But the Queen, believing that she had eaten Snow-white s heart, could not but think that she was again the first and most beautiful of all; and she went to her looking-glass and said --
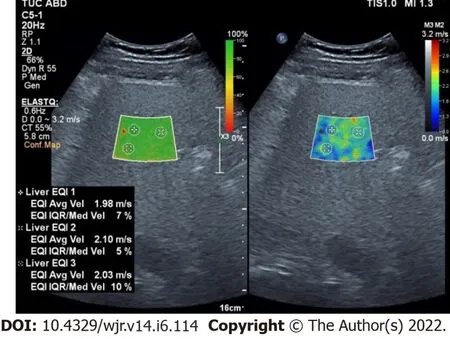
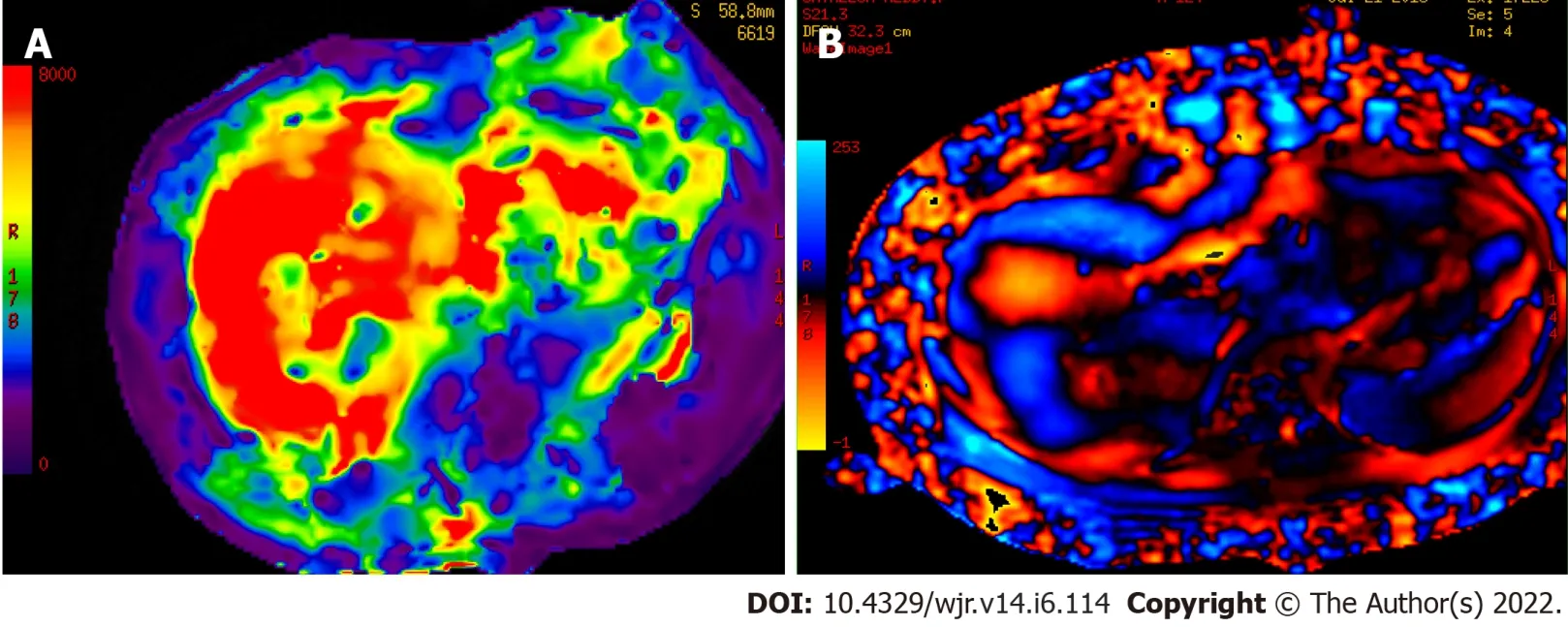
[Strain/shear wave] is useful for further evaluation of lymph nodes and the detection of complications such as fibrosis[37,38]. US elastography (USE) techniques are classified by the type of excitation applied: (1) Strain elastography; and (2) Shear wave elastography. Strain elastography includes constant force-induced displacement (static/quasi-static imaging) or acoustic energy-induced physiologic motion. Shear wave elastography is sub-classified as: Transient elastography, point shear wave elastography (pSWE), two-dimensional SWE (2D-SWE), and three-dimensional SWE. Shear wave USE has clear advantages over strain USE by virtue of being quantitative and user independent. However, shear wave measurements are effective only till 3 cm depth from the skin surface, as the shear wave signal tends to attenuate rapidly beyond this depth. This though is an ideal depth for evaluating most cervical TB lymph nodes. On the color elastogram, red represents the softest and blue represents the hardest areas, while intermediate stiffness is indicated by green. These colors represent the relative hardness of tissues on the elastogram (Figure 2A-C). The units of measurement are kilopascal (kPA) or Velocity (V) in meters/sec (m/s) - [1 KPa = 3 × V
(m/s)][39].
Cervical, axillary, and inguinal lymph nodes are easily evaluated by standard USE; and USE has the potential to non-invasively differentiate tuberculous from metastatic lymph nodes because of the latter’s greater stiffness[40,41]. On strain USE a cut-off value of 3.0 (strain ratio) has been suggested for determining if a mass/tissue is benign or malignant[42-44]. Shehata
[43] stated that the best shear wave elasticity ratio cut-off value that allows significant differentiation between benign and malignant mass groups was > 4.9. USE also has great potential for marking biopsy sites in a lymph node for collecting samples for confirmation of the disease, as well as for drug sensitivity purposes, especially in drug resistant TB (Figure 2D). The samples collected should also be run through CBNAAT techniques such as GenXpert. This will enable MDR TB to be detected upfront (refer ’diagnosis of TB section).

These non-invasive techniques will be useful both for initial diagnosis and follow-up, including treatment - response assessment and monitoring of sequelae;
, post TB medication Liver fibrosis (Figure 3); where avoiding a liver biopsy would be a great boon[38]. Shear wave Elastography features while assessing liver tissue stiffness are as follows: (1) Normal: 1.37 m/s, Metavir F0-F1; (2) Mild Fibrosis: 1.37 - 1.55 m/s, Metavir F2; (3) Advanced Fibrosis: 1.55 - 1.8 m/s, Metavir F3; and (4) Cirrhosis: > 1.8 m/sec, F4[39]. Metavir is an acronym for "meta-analysis of histological data in viral hepatitis".
EUS elastography has proven to be useful for the evaluation of mediastinal and abdominal lymph nodes and can provide additional information about the structure and pathology of mediastinal and abdominal lymph nodes. It is an excellent method for targeting different areas of the lymph node to avoid unnecessary needle passes in EUS guided biopsies[40].
Multimodal ultrasound imaging combines several US modalities simultaneously: Color Doppler US, US elastography, and contrast-enhanced ultrasound (discussed shortly). It differentiates tuberculous from non-tuberculosis superficial tuberculous lymphadenitis with 100.00% sensitivity and a 94.12% positive predictive value[45].
“Theragnostics” combines disease diagnosis with therapy[46,47]. Micrometer-sized gas bubbles “micro-bubbles (MB)” allow for intravenous contrastenhanced US: MBs oscillate resonantly when subjected to high-frequency US, which they reflect intensely[48].
The utility of the same in diagnostic radiology, especially for the urinary tract, is well established[49]. They can readily be utilized for US assessment of vesico-ureteric reflux in patulous golf-hole ureterovesical junctions seen in TB, circumventing the use of ionizing radiation. Kiessling
[50] discuss conjugation of antibodies to the MB surface and incorporation of various molecules inside or onto the MB shell.
The Princess was the King and Queen s only child and it should come as no surprise that the little blacksmith loved her very much for she was both kind and beautiful. She was even smaller than he, and had dancing eyes and long silken hair which she wore in a coiled braid. But, alas3, the little blacksmith could admire the Princess only from afar because she was, after all, a princess and he but a lowly blacksmith--not even that tall. One day a terrible dragon came to the kingdom. Breathing fire on anyone who crossed its path, it trampled4 houses and burned fields. Many knights battled the dragon but their swords could not cut its thick scales. Each night it flew home to its cave in the mountains surrounded by a deep ravine.
MBs have potential for targeted therapies. High-intensity US (HIUS) temporarily disrupts the bloodbrain barrier, allowing medications contained in MBs, which HIUS also disrupts, to treat CNS cancers and intracranial TB[50]. Additionally, MBs can deliver medications to TB lymph nodes, as well as gene therapy to tissues exhibiting congenital disease phenotypes[51].
‘Oh, do not speak to me of marrying,’ sobbed6 the king; ‘rather let me die with you !’ But the queen only smiled faintly, and turned over on her pillow and died.

Dark Field Radiography
X-ray dark-field radiography relies on ultra-small-angle scattering (diffraction) of X-rays at the material interfaces within the tissue under investigation[53]. “Dark field”, when applied to visible light, refers to the bright appearance of scattering objects on a dark background. Healthy lung tissue, with numerous air/parenchyma interfaces in the alveoli, produces a relatively high signal[54,55]. Introduced experimentally in 2008, Dark field radiography may increase sensitivity for early detection of varied lung pathologies involving the alveoli, including tuberculosis.
Computed Tomography
Computed tomography (CT) enables non-invasive diagnosis of TB in patients with negative sputum examination or no sputum production (as occurs in the follow-up of patients on anti-tuberculosis therapy (ATT) or at presentation) non-invasively: it permits empirical ATT initiation until culture results are obtained[56]. Contrast-enhanced CT is the investigation of choice for evaluating mediastinal LNs and identifying pleural enhancement in empyema (Figure 5). High-resolution CT (HRCT) reconstructions are especially useful to detect miliary and centrilobular nodules, ground-glass opacities, and air-trapping (Figure 6).
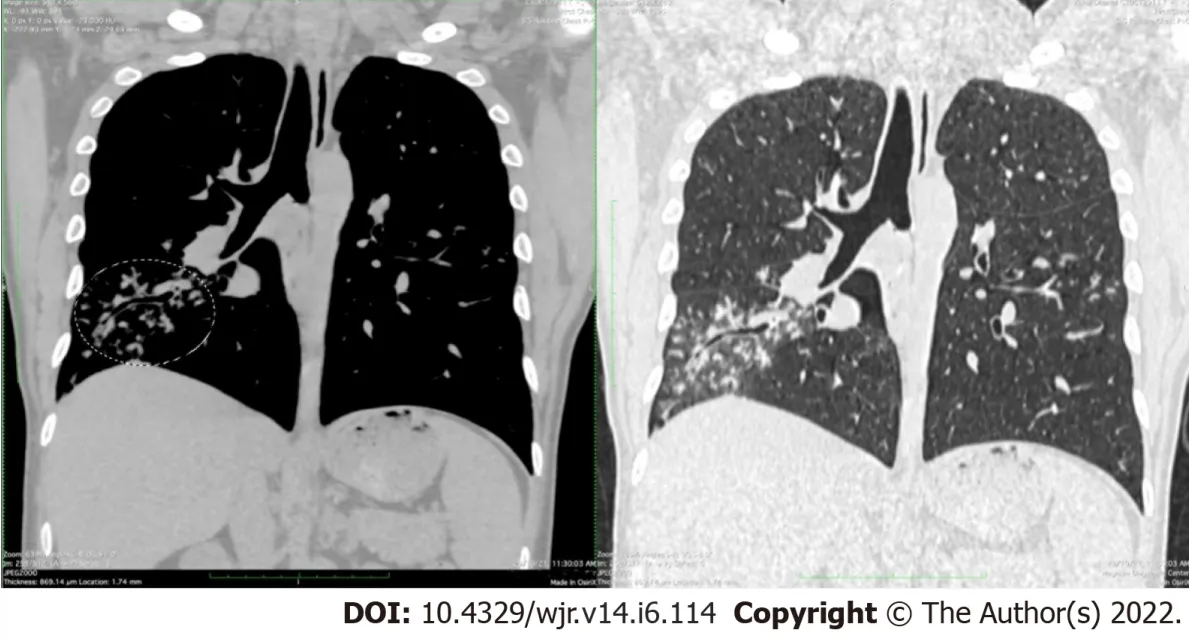
Multi-detector CT and its volumetric capability enables earlier and more accurate diagnosis of pulmonary lesions: detection of radiographically occult disease; assessment of disease activity, parenchymal lesions (including miliary TB), mediastinal lymph nodes (LNs), and visualized bones. It also helps evaluate complications like bronchiectasis, cavitation, associated fungal balls, LN necrosis, and pleural/airway/diaphragmatic pathology (Figure 7).
Spectral imaging on CT (dual-/tri-/quad-energy), when it becomes widely available, should further enhance radiologists’ diagnostic armamentarium[38]. Khan
[57] concluded that dual energy CT is superior to high-resolution CT for assessing pulmonary TB. Recent CT iterative reconstructions allow significant X-ray dose reduction and improved image quality over conventional filtered back-projection reconstruction methods[58]. These advantages would enable greater use of CT in Molecular Imaging.
While radiology training has moved away from conventional radiology, most of the developing world’s population cannot access tomographic (cross sectional) imaging readily for logistic or financial reasons. Therefore, the time-tested signs/patterns of TB in conventional chest X-ray (CXR) cannot be forgotten. There is no excuse for missing a Ghon’s focus/complex or lamellar effusion of childhood TB in a CXR taken for a different purpose (Figure 1). CXR has high sensitivity but limited specificity for detecting pulmonary TB. As recommended by WHO’s guidelines, it is very suitable for TB screening and triaging, to stratify for risk, assess asymptomatic active disease, and for follow-up[33]. Stability of radiographic findings for 6 mo distinguishes inactive from active disease. Where CT is unavailable, lordotic view and penetrated (high kV) views improve depiction of the lung apices and mediastinal/carinal nodes, respectively[34]. Dual-energy radiography with bone subtraction, has also been used to improve depiction of the lung apices[34].
Magnetic Resonance Imaging
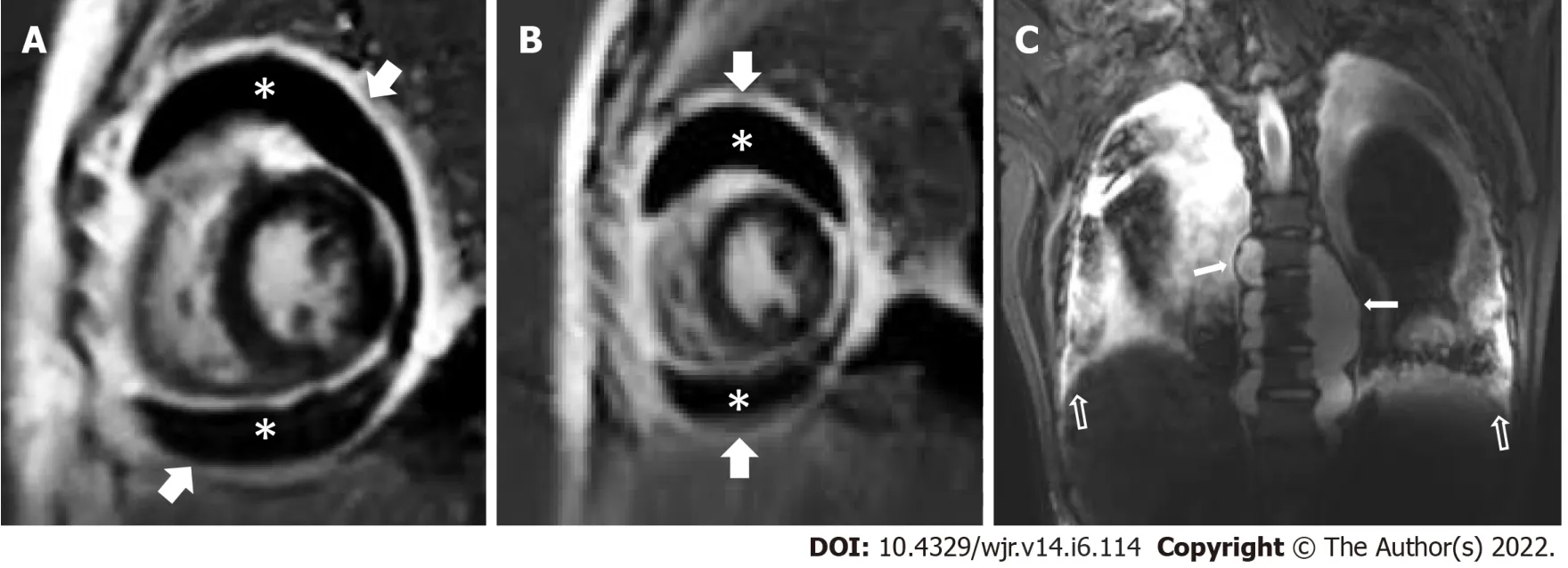
Magnetic resonance imaging (MRI) yields high soft tissue contrast and resolution with high sensitivity for detection of tissue necrosis, as occurs in TB[59]. While MRI lacks the ionizing-radiation hazard, it usually requires longer acquisition times. However, more recently, short-sequence lung MRI (such as HASTE T2, BLADE T2, TRUFI T2 and VIBE T1) have been used for pulmonary imaging in TB patients[60]. Cardiac MRI has made rapid progress too and is the ideal modality for diagnosing Cardiac TB.
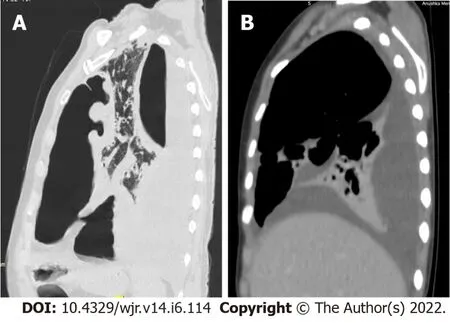
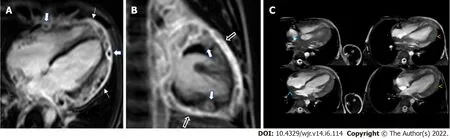
Cardiac TB can take the form of Pericarditis, Peri-Myocarditis or a Pancarditis. Pericardial TB is the commonest manifestation of Cardiac TB (Figure 8A and B). In its early form it is seen as pericardial thickening. In advanced cases, pericardial effusion and septations are seen. Accompanying para-spinal abscesses and pleural effusions can easily be seen (Figure 8C). This may resolve on therapy or can undergo calcification. Myocardial TB is rare and in the presence of a myocardial mass lesion, can frequently be misdiagnosed as a neoplasm. The presence of associated diffuse or non-contiguous pericarditis in the presence of myocardial masses is a good pointer to TB etiology of the cardiac masses: The ‘Myocarditis - Pericarditis Complex’ sign[61] (Figure 9). In a case series of 11 Cardiac TB cases imaged on a 3 Tesla MRI scanner, myocardial lesions were seen in 6 cases (55%) and all of them had concomitant (either diffuse or non-contiguous) pericardial involvement[61]. This is in keeping with the etiopathogenesis of myopericarditis in Cardiac TB. Greater awareness about the “Myopericarditis-Pericarditis Complex” sign/when added to Cardiac AI diagnostic protocols/algorithms, can save the patient from unnecessary invasive tests / cardiac biopsies.
Additionally, novel modalities, such as MR spectroscopy (MRS), chemical exchange saturation transfer (CEST) contrast, Amide Proton transfer imaging and dynamic contrast-enhanced imaging can detect physiological or metabolic changes without the need of exogenous agents. In animal models, these novel MRI capabilities differentiated bacterial infections from sterile inflammation or oncological processes[62,63].
Though currently still under development, low-field-strength (and lower-cost) MRI (0.5 T
1.5 or 3 T for typical scanners), coupled with state-of-the-art hardware, is being evaluated for highquality imaging lungs and heart[64].
MR spectroscopy (MRS) allows imaging of biochemical processes using endogenous metabolites (
, choline, creatine, lactate) or substances labelled with exogenous nuclei such as 19F and 13C. MRS can be performed with most clinical MRI scanners, but multi-voxel MRS scanners are preferred for their greater coverage and resolution. Morales
[65] reported that a singlet peak at ~3.8 parts-per-million (ppm) is present in most tuberculomas and absent in most malignant tumors, allowing differentiation between these lesions.
Ultrasound biomicroscopy (UBM) is a superb tool to assess superficial TB lesions such as skin TB (lupus vulgaris), both in their diagnosis, as well as during follow up (Figure 4). This is safe and easily repeatable and avoids the use of repeated biopsies. Ma
[48] have designed a small-aperture (0.6 mm × 3 mm) IVUS probe optimized for highfrequency contrast imaging. Their design utilizes a dual-frequency (6.5 MHz/30 MHz) transducer for exciting microbubbles at low frequencies (near their resonance) and detecting their broadband harmonics at high frequencies. Fei
[52] have developed broadband lithium niobate single element ultrasonic transducers in the range of 100-300 MHz for high resolution imaging. They claim a performance comparable to optical resolution and state that availability of ultrahigh frequency transducers will make Ultrasound Biomicroscopy (UBM) a promising tool to study fine biological structures. Future applications of CEUS and UBM could be expected in TB too.
CEST contrast MRI uses compounds containing exchangeable protons or molecules in concentrations too low to be visualized using standard MR imaging, with gadolinium substituted by alternative metals, such as manganese, lanthanides, or iron-based agents[66,67]. CEST agents can be diamagnetic or paramagnetic[68].
agents create relatively small chemical shift differences (within 5 ppm of the water signal) that limit the observed effect per injected agent dose.
(PARACEST) ions induce much larger shifts, up to a few hundred ppm, thus allowing much shorter proton lifetimes. PARACEST can be single metal-containing chelates (
, lanthanides), dendrimers, supramolecules, and liposomes.
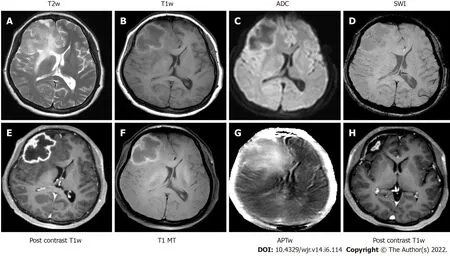
Building on the principles of CEST and Magnetization Transfer (MT), amide proton transfer (APT) imaging generates tissue contrast as a function of the mobile amide protons in the tissue’s native peptides and intracellular proteins (Figure 10). Tuberculomas demonstrate lower MT ratios (MTR
) compared to High Grade Gliomas, reflective of a relative paucity of mobile amide protons in the ambient microenvironment. Elevated MTR
values in the perilesional parenchyma of tuberculomas are a unique observation that may be a clue to the inflammatory milieu[69].
Later that evening, Mother and I revisited the attic in search of the lost letters. Perhaps they are in my oldcollege trunk, my mother said as she quickly located the keys. She unlocked the large sixty-year-old trunk. Lying on top were old tattered15 clothes from years gone by. We started digging, and toward the bottom, we discovered an unmarked gold cardboard box. Mother said she had no clue what was inside. We both held our breath as I slowly lifted off the top. Yes! Here were the long-lost letters! They were all separated by month, tightly bundled in aged16 cotton twine17.
Rapid progress has been noted in the utilisation of MR elastography (MRE), which includes the evaluation of alternatives to the expensive and invasive ‘liver biopsy option’ for assessing liver fibrosis in patients. Hepatic fibrosis is a known complication of TB medications (ATT) (Figure 11)[70]. Imajo
[71] reported that MRE and US shear wave elastography (2D-SWE) demonstrated excellent diagnostic accuracy in detecting liver fibrosis in patients. They reported that MRE demonstrated the highest diagnostic accuracy for stage 4 fibrosis detection and intra - and interobserver reproducibility[71]. MRE has the potential to be applied to detection of TB fibrosis in other organs too,
kidney: Including for treatment-response assessment and monitoring of sequelae, as fibrosis is a common manifestation in TB, including during healing[38]. This could be extremely vital in TB ureteric strictures which need to be stented, as they will heal by fibrosis (with treatment); and could result in serious damage/function loss of the affected kidney, if left unstented.
The development of sequences, arrays of coils, k-space strategies, stochastic imaging, and machine learning (ML)-based image analysis procedures will provide numerous opportunities to improve image contrast in MRI[72,73]. MRI sequences and post-processing techniques may replace or decrease the use of contrast agents (for example 4D MRI instead of MRA and CEST imaging); hybrid technologies such as positron emission tomography (PET)/MR may rely on radiotracers in lieu of MR contrast agents[74].
Nuclear imaging, fusion imaging and miscellaneous
Nuclear imaging detects gamma-radiation produced by radioactive molecules administered noninvasively in micromolar quantities. If such molecules also have biological functions, one visualizes biological processes
through functional images (at the cost of poorer anatomical resolution compared to CT/MRI/High-res US). Well-established for cancer management, molecular imaging may soon have potential for infectious disease[75].
PET uses radionuclides that decay
positron emission relatively quickly (
, 18-Fluorine and 11-Carbon have half-lives of 110 and 20 min) and require an on-site cyclotron to make the radionuclides on demand before they decay. Single-photon emission computed tomography (SPECT) uses longer-lived radionuclides (99-metastable-Technetium and 123-Iodine have half-lives of 6 and 13.2 h). In either case, gamma radiation is converted by semiconductor detectors into electrical signals which are then reconstructed as 3D tomographic images.
Pathogen-specific PET imaging agents currently in development, could provide more accurate data on bacterial burden and other longitudinal information on infection dynamics and treatment responses[76,77].
PET CT (Figure 12A and B) and PET MR (Figure 12C) combines functional imaging (PET, SPECT) for pharmacokinetic/ metabolic information with anatomic imaging (CT, MRI) for structural detail. This permits repeated studies in the same subject over time, a fundamental advantage over traditional techniques. Data thus obtained can be supplied to mathematical models of disease progression, which represents a major advance for the field that has primarily relied on snapshots to understand TB[75]. A small study in adults with MDR-TB, 18F-Fluoro-deoxyglucose (18-FDG) PET plus CT showed quantitative changes in computed abnormal volumes at 2 mo into the treatment that predicted long-term treatment success more sensitively than conventional sputum microbiology, suggesting the potential of imaging scans as possible surrogate endpoints in clinical trials of new TB drug regimens[78]. TB reactivation risk in animal models and human subjects has been accurately identified through 18F-FDG PET/CT[79-81].

: This device’s increased sensitivity (× 40) allows PET scans at extremely low radiation doses while improving the scan speed (potentially in less than a minute) and can track radiopharmaceuticals for longer periods after injection[82]. Although MDR-TB poses mortality risks comparable to those of many common cancers, radiopharmaceutical imaging, while accepted for cancer workup, is oddly avoided for infectious diseases[83]. Explorer total-body PET could allow increased PET use in both pediatric and adult patients with infectious diseases and would be very useful for assessing the extent of TB, especially when involving multiple sites, including the response to treatment[84-86].
A rotating gamma camera captures energies from labelled molecules, which decay
the emission of single gamma rays. Most cameras produce 2D images, although some can perform tomographic 3D reconstructions. Foss
[87] have designed a monoclonal antibody mAb 3d29 that can be used to detect and localize areas of infection with M. tuberculosis non-invasively, on SPECT, 24 h after radiotracer injection.
Optical Imaging provides high-resolution (
, single-cell resolution) live imaging in small animal models and has provided very valuable insights into various biological processes (
, TB granuloma formation)[32,88]. It is performed with highly sensitive fluorescent or bioluminescent agents. However, the use of low-energy photons means that the depth of penetration is limited to only a few centimetres. These could be used for superficial pathologies
cervical lymph nodes, including their complications (TB lymphadenitis, including collar-stud abscess
.).
Advances in ex vivo molecular imaging and microscopy
Including autoradiography, fluorescence microscopy, fluorescence life-time imaging microscopy (FLIM), matrix assisted laser desorption/ ionization mass spectroscopy imaging (MALDI/MSI): Visualization of molecules based on mass detection. MALDI/MSI can simultaneously detect multiple compounds and provides high spatial resolution. Quantum Microscopy (improving the speed and sensitivity of Raman Scatter Microscopy (SRS); visualizing structures that would otherwise be impossible to see.
The molecular imaging techniques discussed below offer potential for cutting-edge research into the cellular mechanisms of TB. While autoradiography and Fluorescence Microscopy are long-established molecular imaging methods, the newer techniques use different modalities and/or extended study in living tissue.
Performed
with highly sensitive fluorescent or bioluminescent agents provides highresolution (
, single-cell resolution) in small animal models, allowing visualization of various biological processes (
, TB granuloma formation)[32,88,89]. However, the use of low-energy photons limits the depth of penetration to a few centimeters. These could be used for superficial pathologies
, cervical lymph nodes, including their complications (TB lymphadenitis, including collar-stud abscess,
).
Multiphoton intravital microscopy (MP-IVM) is based on the simultaneous absorption of two or more (near-) infrared photons. It allows visualization at single-cell resolution within a depth of a few millimeters. Murooka
[90] used MP-IVM to monitor lymphocyte motility in lymph nodes of mice.
This visualizes molecules based on mass detection. MALDI/MSI can simultaneously detect multiple compounds with high spatial resolution. It has been used to localize mycobacterial biomarkers and TB drugs in infected tissue[89]. MALDI-MSI can localize multiple molecules (
, drugs, metabolites, lipids, proteins) simultaneously, overlaying them onto histologically stained sections to reveal the spatial distribution of each molecule with subcellular resolution[89,90]. MALDI-MSI can also be applied to archived tissue blocks dating back decades[91]. This would be a great boon for research, including retrospective studies.
The transition from anatomical imaging to functional/molecular imaging now allows integration of imaging data with various levels of “omics” data (genomics, metabolomics, proteomics, and pharmacogenomics). This may open new avenues for predictive, preventive, and personalized medicines[58].
Yes, the boy said harshly, a single blanket s enough for an old man when he s sent away. We ll save the other half, Dad. It ll come in handy later.
Quantum Microscopy has been utilized for improving the speed and sensitivity of SRS microscopy; visualizing structures that would otherwise be impossible to see. Casacio applied squeezed states of light in SRS, developing a quantum-enhanced-microscope[92]. This enhancement allowed for resolution of the cell membrane which could not be seen on a conventional microscope and sub-micron spatial resolution and the improved image contrast and reduced imaging time surpassed the current state-of-the-art Raman microscopes, while avoiding photodamage in the sample.
MOLECULAR MECHANlSMS lN TB
Role of vitamin D
Another addition worth considering is the humble Vitamin D, which was used to treat TB in the preantibiotic era[93]. Serum levels of 25-hydroxy-cholecalciferol (25-OH-D3) in TB patients have been shown to be lower than in healthy controls[94]. The vitamin D-cathelicidin pathway regulates the autophagy machinery, protective immune defenses, and inflammation; and contributes to immune cooperation between innate and adaptive immunity[95]. Vitamin D activates macrophages and restricts MTB’s intracellular growth[96]. In monocytes and macrophages, MTB lipoprotein binds to the TLR2/TLR1 heterodimer (TLR = Toll-like receptor): this increases vitamin D receptor expression and processing of the pro-vitamin D precursor, which in turn increases production of a mycobactericidal peptide[94]. Vitamin D supplementation during TB treatment accelerates sputum smear conversion and hastens resolution of inflammatory responses[97].
How could I ever forget those beautiful brown eyes and your country accent? she asked, hoping he would guess that she watched for him every time a truck pulled in.
A systematic review (Sutaria
[98]) evaluated 21 randomized, controlled trials and concluded that: (1) TB patients had lower vitamin D status (lower serum levels of 25-OH-D3than healthy, age-matched, and sex-matched controls) [99]; (2) People with certain Vitamin D receptor polymorphisms (BsmI and FokI) had increased susceptibility to TB; and (3) TB patients receiving vitamin D supplementation had improved outcomes in most studies, including shortening treatment duration[98,100]. Vitamin D deficiency may adversely influence TB re-activation/ re-infection: lowered 25-OH-D3 Level leads to a fall in cell-mediated immune defenses, which can activate latent tuberculosis[101]. Hence, it would be worth checking and restoring 25-OH-D3 Levels in malnourished TB patients[102].
Epigenetics perspective
Epigenetics refers to heritable changes in DNA function caused by environmental factors, without altering the DNA sequence, through mechanisms such as DNA (de)methylation (methylation typically deactivates genes) and histone modification (DNA is inactive when tightly bound to histone proteins.) MTB is known to cause histone changes in immune cells that inactivate the defensive IL-2V gene (IL=interleukin), improving MTB’s survival chances[103]. Gauba
[104] review various MTB-induced epigenetic mechanisms. In their review, they have unravelled the numerous ways by which MTB reshapes the host epigenetic landscape as a strategy to overpower the host immune system, for its survival and persistence.
The degree of methylation of key genes in the vitamin D metabolic pathway influence risk and prognosis of tuberculosis[105]. Here’s where Vit D supplementation can play a vital role in protecting against TB and in complimenting Anti TB therapies. Understanding the inter-talk between MTB and epigenetic mechanisms will also play a vital role in controlling/ eliminating the scourge of TB[106]. Analysing epigenetic changes offers great potential in the diagnosis, prevention, and treatment strategies for a wide range of diseases, including TB. CRISPR interference (CRISPRi) has been utilized in mycobacteria to identify novel drug targets by the demonstration of gene essentiality. Faulkner
[107] used CRISPRi to study genes involved in mycobacterial antibiotic resistance, restoring Rifampicin sensitivity in M. smegmatis with CRISPR. This offers hope for the future - for the creation of epigenetically modified Anti -TB drugs to treat MDR and XDR TB.
ADVANCES lN COMPUTlNG
In South Africa, national screening of high-risk groups [
, human immunodeficiency virus (HIV)-infected individuals), deployment of Gene-Xpert machines, treating latent TB, and using quality MTB drugs with shorter regimens led to a decline in TB[25]. We suggest that an identical approach be deployed elsewhere to control the spread of this dreaded scourge.
Artificial intelligence applications in TB
Increasing Internet bandwidth, coupled with transparent data security, has advanced telemedicine, so that remote diagnosis is now routine. Diagnosis can be assisted by Artificial Intelligence (AI). An important AI sub-field, ML, uses statistical techniques, rather than explicitly encoded insight from human experts, to detect patterns in (often considerable) volumes of data. ML allows classification (
, diagnosis) or making predictions. A rapidly progressing branch of ML, called multilayer neural networks or “Deep Learning” (DL), can increase speed and accuracy of onsite and remote diagnosis. DL algorithms have already been used to detect features consistent with pulmonary TB in CXR and CT scans[108].
However, “Artificial Intelligence needs Real Intelligence to guide it!” To maximize AI applications’ accuracy and utility in medical diagnosis and treatment modalities, AI must incorporate experiential wisdom accumulated over decades of clinical and radiological experience time, namely time-tested key medical ‘teaching’ and/or key ‘clinical’ parameters, including prognostic indicators.
Yes, replied the woman, He sends joy and sorrow, and He has aright to send them. To-morrow our little son would have been fiveyears old if we had been permitted to keep him.
TB is no exception. Take childhood (< 15 years) pulmonary TB, which represents 12% of new cases, but 16% of the estimated 1.4 million deaths[109]. This higher mortality highlights the urgent need to improve case detection, and to identify children without TB disease eligible for preventive treatment. One strategy is systematic screening for tuberculosis in high-risk groups[109]. Early diagnosis and prompt treatment will prevent spread to other children at school or in community settings, especially in resource-limited settings[109]. Imaging algorithms can thus play an important role in screening strategies.
In this section, we will also refer to various techniques that fall into the category of “Molecular Imaging Technology” (MIT). MIT visualizes molecules of relevance to a disease at both microscopic levels and in living subjects. For the latter, it provides 3D spatial characterization (often using existing imaging modalities) and non-invasive, temporal monitoring within the same subject[32]. MIT may augment TB research by advancing fundamental knowledge and accelerating the development of novel diagnostics, biomarkers, and therapeutics[32].
The technique of
g (FL), originally pioneered by Google as an application of their well-known MapReduce algorithm allows iteratively training an ML model across geographically separated hardware: the ML algorithm is distributed, while data remains local[111,112]. It can be employed for both statistical and deep learning.
Augmented reality and Virtual reality
Virtual reality creates entirely synthesized 3-D environments, while augmented reality (which is technically simpler to create and often more practical) superimposes synthesized content on existing environments, typically under user control. Both are potentially valuable for teaching/simulation and in clinical practice/patient education, by providing novel visualizations. Clinicians/radiologists could walk the patient through their own body to explain the disease, intended intervention, and anticipated post-intervention changes. Such immersive experiences could likely ensure greater compliance with the treatment regimen.
I wished I could have said that to my husband earlier, but I d been angry. The washing machine had leaked on my brand-new linoleum2. If he d just taken the time to fix it the night before when I asked him instead of playing checkers with Jonathan. What are his priorities anyway? I wondered. I was still mopping up the mess when Jonathan walked into the kitchen. What s for breakfast, Mom? I opened the empty refrigerator. Not cereal, I said, watching the sides of his mouth drop. How about toast and jelly? I smeared3 the toast with jelly and set it in front of him. Why was I so angry? I tossed my husband s dishes into the sudsy() water.
Distributed computing
We introduce distributed computing (DC) because many AI problems, such as would address TB, require computing power that single computing units cannot provide; including data housed in computers at diverse geographical locations. In DC, a computational problem is tackled by multiple, communicating, computing units. It has the following characteristics: (1) The units may lie within a single organization (connected by a local area network) or be distributed geographically (connected by the Internet); (2) Typically, a subset of units (often, just one “central” unit) may operate as either “coordinators” that control/direct other “peripheral” units, or provide resources (
, data, computing services) to them; (3) The central units typically have far more CPU power and storage capacity than the peripheral units. In the extreme case, the peripherals may be devices like smartphones, or even singlepurpose sensors (
, for continuous glucose or EKG monitoring); (4) The central units’ upkeep requires skilled/expensive personnel. In Cloud Computing, the units’ housing/maintenance are outsourced to a “cloud vendor” (Amazon, Microsoft, Google,
). The available services can be scaled up or down in each billing cycle based on the customer’s requirements. The term “cloud” indicates that the central unit is “out there”, its physical location transparent to customers: location may even change; and (5) A single central unit can pose a bottleneck if thousands of small devices connect to it, especially over a sluggish Internet. Edge Computing enhances cloud computing by interposing intermediary units between the peripherals and central units[110]. The Edge units are physically close to the peripherals at a given geographic location (
, at the “Edge” of a network diagram). They prevent overwhelming of the central unit, reduce overall network traffic by aggregating inputs from the peripherals and also provide some computing resources.
ML in general, and DL specifically, need lots of data (as well as diverse data from multiple geographic locales) to achieve the desired accuracy. “Big-data” solutions naturally suggest themselves. However, the obvious solution, physical pooling of data, faces the following barriers: (1) Data privacy - which is less of an issue with all forms of digital imaging, where DICOM metadata containing identifiable information can be removed; and (2) Mistrust - a formidable hurdle when academic or commercial consortia bring rivals together.
While DL excels at recognizing individual patterns (most artificial-vision applications use it), higherlevel knowledge of key imaging and clinical signs allows integrating the individual patterns into a diagnosis. Such “Holistic” algorithms that integrate all the available information-not just on a single patient, but also molecular and epidemiologic knowledge-can significantly improve not only early detection of TB, including MDR-TB, but more effective management and significant improvement in healthcare outcomes.
Typically, a central server coordinates computations across multiple distributed clients. At start-up, the server sends the clients initialization information. The clients commence computation. When each client is done, it sends only aggregate results back to the server, not detailed or identifiable data elements. The server collates all clients’ results and sends updates to each client, which then computes again. The process continues until the ML training completes convergence.
Ng
[113] provide a detailed technology overview. Sheller
[114] use FL to replicate prior analysis of a 10-institution brain-tumor-image-dataset derived from The Cancer Genome Atlas (TCGA). Navia-Vasquez
[115] describe an approach for Federated Logistic Regression.
Most important, many AI algorithms can run in FL mode, making them more accurate because they are based on more voluminous and diverse data. This increases the scope for Multi- Institutional/Multicity collaborations. Dashboards augmented with these algorithms’ can aid key organizational decisionmakers to identify trends (including epidemiological), communicate vital information and monitor performance against strategic goals. Better information through technology-assisted developments would aid WHO, UNICEF and other such organizations counter/eliminate the scourge of TB worldwide. While FL works around institutional barriers, one pays a cost in computational speed, which is limited by Internet bandwidth. In almost all cases, this tradeoff is worthwhile.
In prison, holidays are the worst. Birthdays, anniversaries, Thanksgiving, Christmas, even Valentine s Day can be a bummer. It s difficult and painful to be away from those we love-to be left out of the celebrations and the memory making. Many times, we feel a little forgotten or overlooked.
Quantum technology
“Quantum” technology refers to a highly diverse set of technologies that leverage “quantum mechanics”, the physics of sub-atomic particles. Some of these are established, such as scanning tunneling microscopy and photoionization, while others are still largely theoretical, or in the prototype stage[116]. Quantum Computers and Quantum microscopes, new quantum repeaters enabling a scalable super secure Quantum Internet (distance will no longer be a hindrance, not just IOT but ‘Intelligent Edge’ devices commonplace); will give a quantum boost to Medical Imaging/other healthcare Algorithms/strategies, including in other related fields, improving healthcare in ways beyond the realm of dreams[117].
Hardly had he sat down under the bridge and heaved a sigh, than Puddocky came out; and, sitting down opposite him, asked, What s wrong with you now, dear Prince? The Prince, who this time never doubted the little toad s power to help him, told her his difficulty at once
Quantum entanglement (QE) occurs when a group of particles are generated and interact with each other so that each particle’s sub-atomic (
, quantum) state cannot be described independently of the others’ state. Originally postulated in 1935 by Einstein, Podolsky, and Rosen, it led to seemingly bizarre predictions if true. For example, if one particle encountered an object (
, a bacterium), the other particles would reflect this interaction instantaneously - even if the particles were at opposite ends of the universe, violating General Relativity’s prediction that faster-than-light interactions are impossible. Such predictions led Einstein to believe that Quantum Theory was erroneous: However, QE was demonstrated experimentally almost eight decades later.
With QE using confocal “differential interference contrast,” standard microscopy wavelengths,
, visible light or ultraviolet (UV), provides much higher resolution than without QE, demonstrated by Ono
[118]. QE achieves such detail using much less light (useful for light-sensitive micro-organisms or living tissues when UV is employed). A quantum optical counterpart has been developed to the classical Fourier-transform infrared spectrometer[119]. "Quantum ghost imaging" produced the world's first 2D image captured and reconstructed using asynchronous detection. Ghost imaging is well suited to biological and medical applications, in which light-sensitive cell samples can be observed over a long period because the new processes use less light[120]. QE microscopy may thus impact TB research and diagnosis.
Quantum computing (QC) relies on the possibility of keeping a collection of “qubits” (quantum bits) stable long enough to perform computations with. While a bit (the smallest unit of information in a traditional computer, 1 Byte = 8 bits) can be either 1 or 0, a qubit can be both 1 and 0 simultaneously: thus, 32 qubits can represent 2
approximately equal to 4 billion possibilities. Conceived by Nobelist Richard Feynman, QC’s theoretical foundations were strengthened after Peter Shor’s work (“Shor’s[121] Algorithm) showed that QC could achieve exponential speedup for extremely compute-intensive problems like factorizing the product of two large prime numbers, the basis of RSA (= Rivest, Shamir, Adelman ) encryption. Building a practical Quantum Computer, however, is challenging. Qubits are most stable at very low temperatures (
, 0.025 Kelvin), and most Qubits in a computer perform error correction rather than computation. However, QC is showing remarkable progress - entangling qubits that could improve error correction in quantum computing, creation of a third state to qubits, to create ‘qutrits’ that allow more information to be encoded in a single element and decrease readout errors significantly, development of a high-performance source of "squeezed light" used to transmit information in optical quantum computing; all signify a quantum leap in the technology; with the last being a paradigm shift[122-124]. Optical Quantum computers can now be expected to run at room temperature, without the expensive cooling equipment needed for other quantum computers that use superconductors.
A recent simulated quantum algorithm by Case Western Reserve University and Microsoft scientists (it would have required a quantum computer with 1 million computing qubits) addressed Magnetic Resonance Fingerprinting (MRF)[125]. MRF goes beyond MRI in identifying signatures from individual tissues simultaneously.
If QC’s hardware challenges are solved (there is no clear-cut timeline for this) the impact on general computing, including AI-deep learning, under the hood, performing mathematical optimization-could be extraordinary. Almost all aspects of healthcare would benefit: TB diagnosis and disease modeling would definitely be a part of it. As quantum computers are also ideally suited for solving complex optimization tasks and performing fast searches of unsorted data, this could be relevant for many applications in healthcare related to TB; medical imaging, epidemiological simulations, dashboard creation, holistic algorithm creation, targeted policy making, to a host of other applications; including the realm of Quantum Artificial Intelligence, which offers unlimited possibilities, including many presently undreamable/unthinkable ones. Researchers have now suggested that neuromorphic or brain like computers built using memristors (these resemble neuronal synapsis) would perform well at running neural networks[126]. Scientists in Austria and Italy have already developed a quantum version of the memristor that they suggest could lead to ‘quantum neuromorphic computers’, which in turn could lead to an exponential growth in performance, in an ML approach known as ‘reservoir computing ‘that excels at learning quickly; and may have a quantum advantage over classical reservoir computing, due to the fact that the memristor, unlike any other quantum component has memory[127].
Thus, the Future looks great for QC (including QC based AI) contributing phenomenally to Medical Imaging and overall Healthcare as well. We can merely speculate at the potential applications of this yet ‘Work in Progress’ technology. The spectacular jump in overall computing power will enable hitherto unimaginable tasks to be done in a ‘jiffy’ and thus enable more complex tasks to be thought of. Quantum Artificial Intelligence Algorithms and the like will be something to look forward to. As and when QC evolves the Metaverse will give a more immersive experience both for teaching/simulation and during actual interactions; by giving visualizations/viewpoints that would otherwise not have been possible; with Augmented Reality/Virtual reality (especially for teaching/simulations
.) offering tremendous potential for Medical Imaging in TB, community involvement, amongst other applications; to enable better compliance of TB guidelines and norms (refer the Augmented Reality &/Virtual Reality sectionabove).
CONCLUSlON
While we have discussed numerous technologies, which operate at scales ranging from the subatomic to human populations, the primary challenge for employing these to eliminate the scourge of TB is integrating them into a holistic approach. For example, AI cannot operate in a vacuum; it needs large volumes of data at the patient and population level: incorporating data also from novel imaging modalities, or from translational applications of bench-science research (
, detection of resistance mutations through PCR, augmented optionally by CRISPR), will make it much more useful. The integration must be guided by policies developed by the coordinated actions of international consortia (including bodies like WHO, Big Pharma, national health ministries, philanthropists,
) that make use of diverse expertise around the globe, including those available through leading-edge technologies.
Below, we provide an outline for the implementation of such policies.
Prevention: In addition to current standard practices (besides the usual methods, nutrition, social norms
Screening of vulnerable contacts/populations.
Screening for, and correction of nutritional deficiencies, including vitamin D.
Early diagnosis utilizing newer techniques/technological developments:
, Gene-Xpert, TB QUICK
, for both ‘regular TB’ and MDR/XDR TB, including extrapulmonary samples.
Effective treatment, especially for MDR/XDR TB [including addition of recent drugs, shorter duration regimen (for better compliance)] + vitamin D for better healing as well as complimenting the action of various anti-TB drugs.
Effective monitoring including long term follow up coupled with development of large epidemiological data banks and dashboards that summarize the data therein to facilitate timely decisionmaking.
Enhanced Computing Infrastructure to facilitate all the above, from optimized data gathering, to more sophisticated algorithms, to more powerful hardware architectures.
The following is a useful acronym for the strategies we believe are vital to help us achieve the various targets set by the international health community for elimination of TB.
TB – REVISITED: Regular Screening / Remote patient monitoring; Early Diagnosis; Vitamin D levels/ supplementation; Imaging and Investigations; Set up a Holistic Approach (Clinical/Imaging/Bacteriological); Intelligent comprehensive Holistic AI algorithms (+ wisdom
knowledge); Technology – CBNAAT (GenXpert
)/National - Global Dashboards; Ensure a Global approach/Edge Computing; Do not delay the diagnosis of MDR-TB.
We believe that effective strategy implementation can help alleviate the suffering of millions of underprivileged citizens of the world.
ACKNOWLEDGEMENTS
We wish to thank Merchant N, MD, Diagnostic Radiologist, The Joint Department of Medical Imaging - Lecturer, Faculty of Medicine, University of Toronto, for assistance in preparing this manuscript.
FOOTNOTES
Merchant SA conceptualized the article; all authors wrote, read and approved the final manuscript.
All authors declare no conflict of interests for this article.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
India
Suleman Adam Merchant 0000-0001-6513-450X; Mohd Javed Saifullah Shaikh 0000-0002-5615-4813; Prakash Nadkarni 0000-0002-9628-4700.
Wang LL
A
Wang LL
1 WHO. Global tuberculosis report 2020. [cited 20 January 2022]. Available from: https://www.who.int/publications/i/item/9789240013131
2 WHO. Global Tuberculosis Report 2021. [cited 20 January 2022]. Available from: https://www.who.int/publications/i/item/9789240037021
3 Centers for Disease C and Prevention. Emergence of Mycobacterium tuberculosis with extensive resistance to secondline drugs-worldwide, 2000-2004.
2006; 55: 301-305 [PMID: 16557213]
4 Salazar-Austin N, Ordonez AA, Hsu AJ. Extensively drug-resistant tuberculosis in a young child after travel to India.
2015; 15: 1485-1491 [PMID: 26607130 DOI: 10.1016/S1473-3099(15)00356-4]
5 Kanabus A. TB Statistics - 2020 - deaths, case notifications. [cited 20 January 2022]. Available from: https://tbfacts.org/tb-statistics/(2021)
6 United States AID. [cited 20 January 2022]. Available from: https://blog.usaid.gov/2017/
7 WHO. Global strategy and targets for tuberculosis prevention, care and control after 2015. Sixty seventh World health Assembly: WORLD HEALTH ORGANISATION. [cited 20 January 2022]. Available from: https://apps.who.int/gb/ebwha/pdf_files/WHA67/A67_R1-en.pdf
8 Dye C, Glaziou P, Floyd K. Prospects for tuberculosis elimination.
2013; 34: 271-286 [PMID: 23244049 DOI: 10.1146/annurev-publhealth-031912-114431]
9 Lee JH, Ammerman NC, Nolan S. Prospects for tuberculosis elimination.
2012; 3: 753-753 [PMID: 22434196 DOI: 10.1038/ncomms1724]
10 Comas I, Borrell S, Roetzer A. Whole-genome sequencing of rifampicin-resistant Mycobacterium tuberculosis strains identifies compensatory mutations in RNA polymerase genes.
2011; 44: 106-110 [PMID: 22179134 DOI: 10.1038/ng.1038]
11 Jaleta KN, Gizachew M, Gelaw B. Rifampicin-resistant Mycobacterium tuberculosis among tuberculosis-presumptive cases at University of Gondar Hospital, northwest Ethiopia.
2017; 10: 185-192 [PMID: 28652786 DOI: 10.2147/IDR.S135935]
12 Piatek AS, Van Cleeff M, Alexander H. GeneXpert for TB diagnosis: planned and purposeful implementation.
2013; 1: 18-23 [PMID: 25276513 DOI: 10.9745/GHSP-D-12-00004]
13 WHO. The shorter mdr-tb regimen. [cited 20 January 2022]. Available from: https://apps.who.int/iris/bitstream/handle/10665/250125/9789241549639-eng.pdf
14 Mirzayev F, Viney K, Linh NN, Gonzalez-Angulo L, Gegia M, Jaramillo E, Zignol M, Kasaeva T. World Health Organization recommendations on the treatment of drug-resistant tuberculosis, 2020 update.
2021; 57 [PMID: 33243847 DOI: 10.1183/13993003.03300-2020]
15 Ogwang S, Mubiri P, Bark CM, Joloba ML, Boom WH, Johnson JL. Incubation time of Mycobacterium tuberculosis complex sputum cultures in BACTEC MGIT 960: 4weeks of negative culture is enough for physicians to consider alternative diagnoses.
2015; 83: 162-164 [PMID: 26239846 DOI: 10.1016/j.diagmicrobio.2015.07.002]
16 Chavez Pachas AM, Blank R, Smith Fawzi MC, Bayona J, Becerra MC, Mitnick CD. Identifying early treatment failure on category I therapy for pulmonary tuberculosis in Lima Ciudad, Peru.
2004; 8: 52-58 [PMID: 14974746]
17 Satti H, McLaughlin MM, Seung KJ, Becerra MC, Keshavjee S. High risk of drug-resistant tuberculosis when first-line therapy fails in a high HIV prevalence setting.
2013; 17: 100-106 [PMID: 23232009 DOI: 10.5588/ijtld.12.0344]
18 WHO. Multidrug and extensively drug-resistant TB (M/XDR-TB). 2010. [cited 20 January 2022]. Available from: http://apps.who.int/iris/bitstream/handle/10665/44286/9789241599191_eng.pdf?sequence=1
19 Osei Sekyere J, Maphalala N, Malinga LA, Mbelle NM, Maningi NE. A Comparative Evaluation of the New Genexpert MTB/RIF Ultra and other Rapid Diagnostic Assays for Detecting Tuberculosis in Pulmonary and Extra Pulmonary Specimens.
2019; 9: 16587 [PMID: 31719625 DOI: 10.1038/s41598-019-53086-5]
20 Helb D, Jones M, Story E, Boehme C, Wallace E, Ho K, Kop J, Owens MR, Rodgers R, Banada P, Safi H, Blakemore R, Lan NT, Jones-López EC, Levi M, Burday M, Ayakaka I, Mugerwa RD, McMillan B, Winn-Deen E, Christel L, Dailey P, Perkins MD, Persing DH, Alland D. Rapid detection of Mycobacterium tuberculosis and rifampin resistance by use of ondemand, near-patient technology.
2010; 48: 229-237 [PMID: 19864480 DOI: 10.1128/JCM.01463-09]
21 Perez-Risco D, Rodriguez-Temporal D, Valledor-Sanchez I, Alcaide F. Evaluation of the Xpert MTB/RIF Ultra Assay for Direct Detection of Mycobacterium tuberculosis Complex in Smear-Negative Extrapulmonary Samples.
2018; 56 [PMID: 29950333 DOI: 10.1128/JCM.00659-18]
22 Dorman SE, Schumacher SG, Alland D, Nabeta P, Armstrong DT, King B, Hall SL, Chakravorty S, Cirillo DM, Tukvadze N, Bablishvili N, Stevens W, Scott L, Rodrigues C, Kazi MI, Joloba M, Nakiyingi L, Nicol MP, Ghebrekristos Y, Anyango I, Murithi W, Dietze R, Lyrio Peres R, Skrahina A, Auchynka V, Chopra KK, Hanif M, Liu X, Yuan X, Boehme CC, Ellner JJ, Denkinger CM; study team. Xpert MTB/RIF Ultra for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospective multicentre diagnostic accuracy study.
2018; 18: 76-84 [PMID: 29198911 DOI: 10.1016/S1473-3099(17)30691-6]
23 Mechal Y, Benaissa E, El Mrimar N, Benlahlou Y, Bssaibis F, Zegmout A, Chadli M, Malik YS, Touil N, Abid A, Maleb A, Elouennass M. Evaluation of GeneXpert MTB/RIF system performances in the diagnosis of extrapulmonary tuberculosis.
2019; 19: 1069 [PMID: 31856744 DOI: 10.1186/s12879-019-4687-7]
24 Sam IK, Chen YY, Ma J, Li SY, Ying RY, Li LX, Ji P, Wang SJ, Xu J, Bao YJ, Zhao GP, Zheng HJ, Wang J, Sha W, Wang Y. TB-QUICK: CRISPR-Cas12b-assisted rapid and sensitive detection of Mycobacterium tuberculosis.
2021; 83: 54-60 [PMID: 33951419 DOI: 10.1016/j.jinf.2021.04.032]
25 Churchyard GJ, Mametja LD, Mvusi L, Ndjeka N, Hesseling AC, Reid A, Babatunde S, Pillay Y. Tuberculosis control in South Africa: successes, challenges and recommendations.
2014; 104: 244-248 [PMID: 24893501 DOI: 10.7196/samj.7689]
26 Noertjojo K, Tam CM, Chan SL, Tan J, Chan-Yeung M. Contact examination for tuberculosis in Hong Kong is useful.
2002; 6: 19-24 [PMID: 11931396]
27 Lee MS, Leung CC, Kam KM, Wong MY, Leung MC, Tam CM, Leung EC. Early and late tuberculosis risks among close contacts in Hong Kong.
2008; 12: 281-287 [PMID: 18284833]
28 Leung EC, Leung CC, Kam KM, Yew WW, Chang KC, Leung WM, Tam CM. Transmission of multidrug-resistant and extensively drug-resistant tuberculosis in a metropolitan city.
2013; 41: 901-908 [PMID: 22878878 DOI: 10.1183/09031936.00071212]
29 Dye C, Williams BG. Eliminating human tuberculosis in the twenty-first century.
2008; 5: 653-662 [PMID: 17690054 DOI: 10.1098/rsif.2007.1138]
30 Harisinghani MG, McLoud TC, Shepard JA, Ko JP, Shroff MM, Mueller PR. Tuberculosis from head to toe.
2000; 20: 449-70; quiz 528 [PMID: 10715343 DOI: 10.1148/radiographics.20.2.g00mc12449]
31 Bomanji JB, Gupta N, Gulati P, Das CJ. Imaging in tuberculosis.
2015; 5 [PMID: 25605754 DOI: 10.1101/cshperspect.a017814]
32 Ordonez AA, Tucker EW, Anderson CJ, Carter CL, Ganatra S, Kaushal D, Kramnik I, Lin PL, Madigan CA, Mendez S, Rao J, Savic RM, Tobin DM, Walzl G, Wilkinson RJ, Lacourciere KA, Via LE, Jain SK. Visualizing the dynamics of tuberculosis pathology using molecular imaging.
2021; 131 [PMID: 33645551 DOI: 10.1172/JCI145107]
33 WHO. Chest radiography in tuberculosis detection. [cited 20 January 2022]. Available from: https://apps.who.int/iris/handle/10665/252424
34 Sharma M, Sandhu MS, Gorsi U, Gupta D, Khandelwal N. Role of digital tomosynthesis and dual energy subtraction digital radiography in detection of parenchymal lesions in active pulmonary tuberculosis.
2015; 84: 1820-1827 [PMID: 26071244 DOI: 10.1016/j.ejrad.2015.05.031]
35 Yu TZ, Zhang Y, Zhang WZ, Yang GY. Role of ultrasound in the diagnosis of cervical tuberculous lymphadenitis in children.
2021; 17: 544-550 [PMID: 34472036 DOI: 10.1007/s12519-021-00453-w]
36 Navani N, Molyneaux PL, Breen RA, Connell DW, Jepson A, Nankivell M, Brown JM, Morris-Jones S, Ng B, Wickremasinghe M, Lalvani A, Rintoul RC, Santis G, Kon OM, Janes SM. Utility of endobronchial ultrasound-guided transbronchial needle aspiration in patients with tuberculous intrathoracic lymphadenopathy: a multicentre study.
2011; 66: 889-893 [PMID: 21813622 DOI: 10.1136/thoraxjnl-2011-200063]
37 Wang B, Guo Q, Wang JY, Yu Y, Yi AJ, Cui XW, Dietrich CF. Ultrasound Elastography for the Evaluation of Lymph Nodes.
2021; 11: 714660 [PMID: 34485150 DOI: 10.3389/fonc.2021.714660]
38 Merchant S, Bharati A, Merchant N. Tuberculosis of the genitourinary system-Urinary tract tuberculosis: Renal tuberculosis-Part II.
2013; 23: 64-77 [PMID: 23986619 DOI: 10.4103/0971-3026.113617]
39 Chaubal N, Bam A & Khatdare K. Elastography of Lymph Nodes. In: Richard. G Barr (Ed) Elastography - A Practical Approach. First ed. New York - Stuttgart: Thieme, 2017: 100-114
40 Dietrich CF, Jenssen C, Arcidiacono PG, Cui XW, Giovannini M, Hocke M, Iglesias-Garcia J, Saftoiu A, Sun S, Chiorean L. Endoscopic ultrasound: Elastographic lymph node evaluation.
2015; 4: 176-190 [PMID: 26374575 DOI: 10.4103/2303-9027.162995]
41 Kanagaraju V, Rakshith AVB, Devanand B, Rajakumar R. Utility of Ultrasound Elastography to Differentiate Benign from Malignant Cervical Lymph Nodes.
2020; 28: 92-98 [PMID: 32874867 DOI: 10.4103/JMU.JMU_72_19]
42 ?zel D, ?zel BD. Evaluating the role of strain ratio elastography in determining malignancy potential and calculating objective BIRADS US scores using ultrasonography and elastography features.
2018; 83: e268-e274 [PMID: 30627246 DOI: 10.5114/pjr.2018.76790]
43 Shehata RMA, El-Sharkawy MAM, Mahmoud OM. Qualitative and quantitative strain and shear wave elastography paradigm in differentiation of breast lesions. [cited 20 January 2022]. Available from: https://ejrnm.springeropen.com/articles/10.1186/s43055-022-00697-0
44 Wang Z, Yang T, Wu Z, Tang S, Liang X, Qin A, Ouyang T, Liu P, Liu J. Correlation between elastography score and strain rate ratio in breast small tumor. Zhongnan Daxue Xuebao Yixueban 2010; 35: 928-932 [PMID: 20871156 DOI: 10.3969/j.issn.1672-7347.2010.09.005]
45 Chu J, Zhang Y, Zhang W, Zhao D, Xu J, Yu T, Yang G. The value of multimodal ultrasonography in differential diagnosis of tuberculous and non-tuberculous superficial lymphadenitis. BMC Surg 2021; 21: 416 [PMID: 34906107 DOI: 10.1186/s12893-021-01418-6]
46 Lammers T, Aime S, Hennink WE, Storm G, Kiessling F. Theranostic nanomedicine. Acc Chem Res 2011; 44: 1029-1038 [PMID: 21545096 DOI: 10.1021/ar200019c]
47 Martin KH, Dayton PA. Current status and prospects for microbubbles in ultrasound theranostics. Wiley Interdiscip Rev Nanomed Nanobiotechnol 2013; 5: 329-345 [PMID: 23504911 DOI: 10.1002/wnan.1219]
48 Ma J, Martin K, Dayton PA, Jiang X. A preliminary engineering design of intravascular dual-frequency transducers for contrast-enhanced acoustic angiography and molecular imaging. IEEE Trans Ultrason Ferroelectr Freq Control 2014; 61: 870-880 [PMID: 24801226 DOI: 10.1109/TUFFC.2014.6805699]
49 Duran C, Beltrán VP, González A, Gómez C, Riego JD. Contrast-enhanced Voiding Urosonography for Vesicoureteral Reflux Diagnosis in Children. Radiographics 2017; 37: 1854-1869 [PMID: 29019761 DOI: 10.1148/rg.2017170024]
50 Kiessling F, Fokong S, Bzyl J, Lederle W, Palmowski M, Lammers T. Recent advances in molecular, multimodal and theranostic ultrasound imaging. Adv Drug Deliv Rev 2014; 72: 15-27 [PMID: 24316070 DOI: 10.1016/j.addr.2013.11.013]
51 Palmowski M, Morgenstern B, Hauff P, Reinhardt M, Huppert J, Maurer M, Woenne EC, Doerk S, Ladewig G, Jenne JW, Delorme S, Grenacher L, Hallscheidt P, Kauffmann GW, Semmler W, Kiessling F. Pharmacodynamics of streptavidin-coated cyanoacrylate microbubbles designed for molecular ultrasound imaging. Invest Radiol 2008; 43: 162-169 [PMID: 18301312 DOI: 10.1097/RLI.0b013e31815a251b]
52 Fei C, Chiu CT, Chen X, Chen Z, Ma J, Zhu B, Shung KK, Zhou Q. Ultrahigh Frequency (100 MHz-300 MHz) Ultrasonic Transducers for Optical Resolution Medical Imagining. Sci Rep 2016; 6: 28360 [PMID: 27329379 DOI: 10.1038/srep28360]
53 Willer K, Fingerle AA, Gromann LB, De Marco F, Herzen J, Achterhold K, Gleich B, Muenzel D, Scherer K, Renz M, Renger B, Kopp F, Kriner F, Fischer F, Braun C, Auweter S, Hellbach K, Reiser MF, Schroeter T, Mohr J, Yaroshenko A, Maack HI, Pralow T, van der Heijden H, Proksa R, Koehler T, Wieberneit N, Rindt K, Rummeny EJ, Pfeiffer F, No?l PB. X-ray dark-field imaging of the human lung-A feasibility study on a deceased body. PLoS One 2018; 13: e0204565 [PMID: 30261038 DOI: 10.1371/journal.pone.0204565]
54 Bech M, Tapfer A, Velroyen A, Yaroshenko A, Pauwels B, Hostens J, Bruyndonckx P, Sasov A, Pfeiffer F. In-vivo darkfield and phase-contrast x-ray imaging. Sci Rep 2013; 3: 3209 [PMID: 24220606 DOI: 10.1038/srep03209]
55 Schleede S, Meinel FG, Bech M, Herzen J, Achterhold K, Potdevin G, Malecki A, Adam-Neumair S, Thieme SF, Bamberg F, Nikolaou K, Bohla A, Yildirim A?, Loewen R, Gifford M, Ruth R, Eickelberg O, Reiser M, Pfeiffer F. Emphysema diagnosis using X-ray dark-field imaging at a laser-driven compact synchrotron light source. Proc Natl Acad Sci U S A 2012; 109: 17880-17885 [PMID: 23074250 DOI: 10.1073/pnas.1206684109]
56 Bhalla AS, Goyal A, Guleria R, Gupta AK. Chest tuberculosis: Radiological review and imaging recommendations. Indian J Radiol Imaging 2015; 25: 213-225 [PMID: 26288514]
57 Khan AU, Khanduri S, Tarin Z, Abbas SZ, Husain M, Singh A, Yadav P, Jain S. Dual-Energy Computed Tomography Lung in patients of Pulmonary Tuberculosis. J Clin Imaging Sci 2020; 10: 39 [PMID: 32754374 DOI: 10.25259/JCIS_78_2020]
58 Huang HM, Shih YY. Pushing CT and MR imaging to the molecular level for studying the "omics": current challenges and advancements. Biomed Res Int 2014; 2014: 365812 [PMID: 24738056 DOI: 10.1155/2014/365812]
59 Peprah KO, Andronikou S, Goussard P. Characteristic magnetic resonance imaging low T2 signal intensity of necrotic lung parenchyma in children with pulmonary tuberculosis. J Thorac Imaging 2012; 27: 171-174 [PMID: 21516045 DOI: 10.1097/RTI.0b013e318211abfb]
60 Sodhi KS, Khandelwal N, Saxena AK, Singh M, Agarwal R, Bhatia A, Lee EY. Rapid lung MRI in children with pulmonary infections: Time to change our diagnostic algorithms. J Magn Reson Imaging 2016; 43: 1196-1206 [PMID: 26546472 DOI: 10.1002/jmri.25082]
61 Bharati A, Merchant S, Nagesh C. The ‘Myocarditis-Pericarditis’ Complex - A CMR Sign of Cardiac Tuberculosis and The Spectrum of imaging findings of Cardiac Tuberculosis on CMR. RSNA Annual Conference. Chicago: Radiological Society of North America, 2013. [cited 20 January 2022]. Available from: https://archive.rsna.org/2013/13012394.html
62 Liu J, Bai R, Li Y, Staedtke V, Zhang S, van Zijl PCM, Liu G. MRI detection of bacterial brain abscesses and monitoring of antibiotic treatment using bacCEST. Magn Reson Med 2018; 80: 662-671 [PMID: 29577382 DOI: 10.1002/mrm.27180]
63 Goldenberg JM, Berthusen AJ, Cárdenas-Rodríguez J, Pagel MD. Differentiation of Myositis-Induced Models of Bacterial Infection and Inflammation with T
-Weighted, CEST, and DCE-MRI. Tomography 2019; 5: 283-291 [PMID: 31572789 DOI: 10.18383/j.tom.2019.00009]
64 Campbell-Washburn AE, Ramasawmy R, Restivo MC, Bhattacharya I, Basar B, Herzka DA, Hansen MS, Rogers T, Bandettini WP, McGuirt DR, Mancini C, Grodzki D, Schneider R, Majeed W, Bhat H, Xue H, Moss J, Malayeri AA, Jones EC, Koretsky AP, Kellman P, Chen MY, Lederman RJ, Balaban RS. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology 2019; 293: 384-393 [PMID: 31573398 DOI: 10.1148/radiol.2019190452]
65 Morales H, Alfaro D, Martinot C, Fayed N, Gaskill-Shipley M. MR spectroscopy of intracranial tuberculomas: A singlet peak at 3.8 ppm as potential marker to differentiate them from malignant tumors. Neuroradiol J 2015; 28: 294-302 [PMID: 26246099 DOI: 10.1177/1971400915592077]
66 van Zijl PC, Yadav NN. Chemical exchange saturation transfer (CEST): what is in a name and what isn't? Magn Reson Med 2011; 65: 927-948 [PMID: 21337419 DOI: 10.1002/mrm.22761]
67 Minton LE, Pandit R, Willoughby WR, Porter KK. The Future of Magnetic Resonance Imaging Contrast Agents. Appl Radiol 2022; 51: 7-11 [cited 20 January 2022]. Available from: https://appliedradiology.com/articles/the-future-ofmagnetic-resonance-imaging-contrast-agents
68 Hancu I, Dixon WT, Woods M, Vinogradov E, Sherry AD, Lenkinski RE. CEST and PARACEST MR contrast agents. Acta Radiol 2010; 51: 910-923 [PMID: 20828299 DOI: 10.3109/02841851.2010.502126]
69 Kulanthaivelu K, Jabeen S, Saini J, Raju S, Nalini A, Sadashiva N, Hegde S, Rolla NK, Saha I, M N, Vengalil S, Swaroop S, Rao S. Amide proton transfer imaging for differentiation of tuberculomas from high-grade gliomas: Preliminary experience. Neuroradiol J 2021; 34: 440-448 [PMID: 33823712 DOI: 10.1177/19714009211002766]
70 Biswas A, Santra S, Bishnu D, Dhali GK, Chowdhury A, Santra A. Isoniazid and Rifampicin Produce Hepatic Fibrosis through an Oxidative Stress-Dependent Mechanism. Int J Hepatol 2020; 2020: 6987295 [PMID: 32373368 DOI: 10.1155/2020/6987295]
71 Imajo K, Honda Y, Kobayashi T, Nagai K, Ozaki A, Iwaki M, Kessoku T, Ogawa Y, Takahashi H, Saigusa Y, Yoneda M, Kirikoshi H, Utsunomiya D, Aishima S, Saito S, Nakajima A. Direct Comparison of US and MR Elastography for Staging Liver Fibrosis in Patients With Nonalcoholic Fatty Liver Disease. Clin Gastroenterol Hepatol 2022; 20: 908-917.e11 [PMID: 33340780]
72 Xu C, Howey J, Ohorodnyk P, Roth M, Zhang H, Li S. Segmentation and quantification of infarction without contrast agents via spatiotemporal generative adversarial learning. Med Image Anal 2020; 59: 101568 [PMID: 31622838 DOI: 10.1016/j.media.2019.101568]
73 de Figueiredo EH, Borgonovi AF, Doring TM. Basic concepts of MR imaging, diffusion MR imaging, and diffusion tensor imaging. Magn Reson Imaging Clin N Am 2011; 19: 1-22 [PMID: 21129633 DOI: 10.1016/j.mric.2010.10.005]
74 Jadvar H, Colletti PM. Competitive advantage of PET/MRI. Eur J Radiol 2014; 83: 84-94 [PMID: 23791129 DOI: 10.1016/j.ejrad.2013.05.028]
75 Ordonez AA, Sellmyer MA, Gowrishankar G, Ruiz-Bedoya CA, Tucker EW, Palestro CJ, Hammoud DA, Jain SK. Molecular imaging of bacterial infections: Overcoming the barriers to clinical translation. Sci Transl Med 2019; 11 [PMID: 31484790 DOI: 10.1126/scitranslmed.aax8251]
76 Ordonez AA, Weinstein EA, Bambarger LE, Saini V, Chang YS, DeMarco VP, Klunk MH, Urbanowski ME, Moulton KL, Murawski AM, Pokkali S, Kalinda AS, Jain SK. A Systematic Approach for Developing Bacteria-Specific Imaging Tracers. J Nucl Med 2017; 58: 144-150 [PMID: 27635025 DOI: 10.2967/jnumed.116.181792]
77 Sly LM, Hingley-Wilson SM, Reiner NE, McMaster WR. Survival of Mycobacterium tuberculosis in host macrophages involves resistance to apoptosis dependent upon induction of antiapoptotic Bcl-2 family member Mcl-1. J Immunol 2003; 170: 430-437 [PMID: 12496428 DOI: 10.4049/jimmunol.170.1.430]
78 Chen RY, Dodd LE, Lee M, Paripati P, Hammoud DA, Mountz JM, Jeon D, Zia N, Zahiri H, Coleman MT, Carroll MW, Lee JD, Jeong YJ, Herscovitch P, Lahouar S, Tartakovsky M, Rosenthal A, Somaiyya S, Lee S, Goldfeder LC, Cai Y, Via LE, Park SK, Cho SN, Barry CE 3rd. PET/CT imaging correlates with treatment outcome in patients with multidrugresistant tuberculosis. Sci Transl Med 2014; 6: 265ra166 [PMID: 25473034 DOI: 10.1126/scitranslmed.3009501]
79 Davis SL, Nuermberger EL, Um PK, Vidal C, Jedynak B, Pomper MG, Bishai WR, Jain SK. Noninvasive pulmonary [18F]-2-fluoro-deoxy-D-glucose positron emission tomography correlates with bactericidal activity of tuberculosis drug treatment. Antimicrob Agents Chemother 2009; 53: 4879-4884 [PMID: 19738022 DOI: 10.1128/AAC.00789-09]
80 Lin PL, Maiello P, Gideon HP, Coleman MT, Cadena AM, Rodgers MA, Gregg R, O'Malley M, Tomko J, Fillmore D, Frye LJ, Rutledge T, DiFazio RM, Janssen C, Klein E, Andersen PL, Fortune SM, Flynn JL. PET CT Identifies Reactivation Risk in Cynomolgus Macaques with Latent M. tuberculosis. PLoS Pathog 2016; 12: e1005739 [PMID: 27379816 DOI: 10.1371/journal.ppat.1005739]
81 Esmail H, Lai RP, Lesosky M, Wilkinson KA, Graham CM, Coussens AK, Oni T, Warwick JM, Said-Hartley Q, Koegelenberg CF, Walzl G, Flynn JL, Young DB, Barry Iii CE, O'Garra A, Wilkinson RJ. Characterization of progressive HIV-associated tuberculosis using 2-deoxy-2-[
F]fluoro-D-glucose positron emission and computed tomography. Nat Med 2016; 22: 1090-1093 [PMID: 27595321 DOI: 10.1038/nm.4161]
82 Cherry SR, Jones T, Karp JS, Qi J, Moses WW, Badawi RD. Total-Body PET: Maximizing Sensitivity to Create New Opportunities for Clinical Research and Patient Care. J Nucl Med 2018; 59: 3-12 [PMID: 28935835 DOI: 10.2967/jnumed.116.184028]
83 Jain SK. The Promise of Molecular Imaging in the Study and Treatment of Infectious Diseases. Mol Imaging Biol 2017; 19: 341-347 [PMID: 28155078 DOI: 10.1007/s11307-017-1055-0]
84 Cherry SR, Badawi RD, Karp JS, Moses WW, Price P, Jones T. Total-body imaging: Transforming the role of positron emission tomography. Sci Transl Med 2017; 9 [PMID: 28298419 DOI: 10.1126/scitranslmed.aaf6169]
85 Badawi RD, Shi H, Hu P, Chen S, Xu T, Price PM, Ding Y, Spencer BA, Nardo L, Liu W, Bao J, Jones T, Li H, Cherry SR. First Human Imaging Studies with the EXPLORER Total-Body PET Scanner. J Nucl Med 2019; 60: 299-303 [PMID: 30733314 DOI: 10.2967/jnumed.119.226498]
86 Lv Y, Lv X, Liu W, Judenhofer MS, Zwingenberger A, Wisner E, Berg E, McKenney S, Leung E, Spencer BA, Cherry SR, Badawi RD. Mini EXPLORER II: a prototype high-sensitivity PET/CT scanner for companion animal whole body and human brain scanning. Phys Med Biol 2019; 64: 075004 [PMID: 30620929 DOI: 10.1088/1361-6560/aafc6c]
87 Foss CA, Kulik L, Ordonez AA, Jain SK, Michael Holers V, Thurman JM, Pomper MG. SPECT/CT Imaging of Mycobacterium tuberculosis Infection with [
I]anti-C3d mAb. Mol Imaging Biol 2019; 21: 473-481 [PMID: 29998399 DOI: 10.1007/s11307-018-1228-5]
88 Murooka TT, Mempel TR. Multiphoton intravital microscopy to study lymphocyte motility in lymph nodes. Methods Mol Biol 2012; 757: 247-257 [PMID: 21909917 DOI: 10.1007/978-1-61779-166-6_16]
89 Blanc L, Lenaerts A, Dartois V, Prideaux B. Visualization of Mycobacterial Biomarkers and Tuberculosis Drugs in Infected Tissue by MALDI-MS Imaging. Anal Chem 2018; 90: 6275-6282 [PMID: 29668262 DOI: 10.1021/acs.analchem.8b00985]
90 Niehaus M, Soltwisch J, Belov ME, Dreisewerd K. Transmission-mode MALDI-2 mass spectrometry imaging of cells and tissues at subcellular resolution.
2019; 16: 925-931 [PMID: 31451764 DOI: 10.1038/s41592-019-0536-2]
91 Paine MRL, Ellis SR, Maloney D, Heeren RMA, Verhaert PDEM. Digestion-Free Analysis of Peptides from 30-year-old Formalin-Fixed, Paraffin-Embedded Tissue by Mass Spectrometry Imaging.
2018; 90: 9272-9280 [PMID: 29975508 DOI: 10.1021/acs.analchem.8b01838]
92 Casacio, Catxere and Andrade. Quantum enhanced microscopy. A thesis submitted for the degree of Doctor of Philosophy - The University of Queensland, Australia, 2020. [cited 20 January 2022]. Available from: https://espace.library.uq.edu.au/
93 Martineau AR, Honecker FU, Wilkinson RJ, Griffiths CJ. Vitamin D in the treatment of pulmonary tuberculosis.
2007; 103: 793-798 [PMID: 17223549 DOI: 10.1016/j.jsbmb.2006.12.052]
94 Nnoaham KE, Clarke A. Low serum vitamin D levels and tuberculosis: a systematic review and meta-analysis.
2008; 37: 113-119 [PMID: 18245055 DOI: 10.1093/ije/dym247]
95 Chung C, Silwal P, Kim I, Modlin RL, Jo EK. Vitamin D-Cathelicidin Axis: at the Crossroads between Protective Immunity and Pathological Inflammation during Infection.
2020; 20: e12 [PMID: 32395364 DOI: 10.4110/in.2020.20.e12]
96 Arora VK, Jaiswal AK. Vitamin D receptor polymorphism and active tuberculosis. [cited 20 January 2022]. Available from: http://tbassnindia.org/images/TB_October_2013_issue.pdf
97 Coussens AK, Wilkinson RJ, Hanifa Y, Nikolayevskyy V, Elkington PT, Islam K, Timms PM, Venton TR, Bothamley GH, Packe GE, Darmalingam M, Davidson RN, Milburn HJ, Baker LV, Barker RD, Mein CA, Bhaw-Rosun L, Nuamah R, Young DB, Drobniewski FA, Griffiths CJ, Martineau AR. Vitamin D accelerates resolution of inflammatory responses during tuberculosis treatment.
2012; 109: 15449-15454 [PMID: 22949664 DOI: 10.1073/pnas.1200072109]
98 Sutaria N, Liu CT, Chen TC. Vitamin D Status, Receptor Gene Polymorphisms, and Supplementation on Tuberculosis: A Systematic Review of Case-Control Studies and Randomized Controlled Trials.
2014; 1: 151-160 [PMID: 25599020 DOI: 10.1016/j.jcte.2014.08.001]
99 Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications.
2001; 22: 477-501 [PMID: 11493580 DOI: 10.1210/edrv.22.4.0437]
100 Junaid K, Rehman A. Impact of vitamin D on infectious disease-tuberculosis-a Review. [cited 20 January 2022]. Available from: https://www.clinicalnutritionopenscience.com/article/S2352-9393(19)30017-X/pdf
101 Davies PD. The role of vitamin D in tuberculosis.
1989; 139: 1571 [PMID: 2729764 DOI: 10.1164/ajrccm/139.6.1571]
102 Merchant S, Bharati A, Merchant N. Tuberculosis of the genitourinary system-Urinary tract tuberculosis: Renal tuberculosis-Part I.
2013; 23: 46-63 [PMID: 23986618 DOI: 10.4103/0971-3026.113615]
103 Kathirvel M, Mahadevan S. The role of epigenetics in tuberculosis infection.
2016; 8: 537-549 [PMID: 27035266 DOI: 10.2217/epi.16.1]
104 Gauba K, Gupta S, Shekhawat J, Sharma P, Yadav D, Banerjee M. Immunomodulation by epigenome alterations in Mycobacterium tuberculosis infection.
2021; 128: 102077 [PMID: 33812175 DOI: 10.1016/j.tube.2021.102077]
105 Wang M, Kong W, He B, Li Z, Song H, Shi P, Wang J. Vitamin D and the promoter methylation of its metabolic pathway genes in association with the risk and prognosis of tuberculosis.
2018; 10: 118 [PMID: 30208925 DOI: 10.1186/s13148-018-0552-6]
106 Tarashi S, Badi SA, Moshiri A, Ebrahimzadeh N, Fateh A, Vaziri F, Aazami H, Siadat SD, Fuso A. The inter-talk between
and the epigenetic mechanisms.
2020; 12: 455-469 [PMID: 32267165 DOI: 10.2217/epi-2019-0187]
107 Faulkner V, Cox AA, Goh S, van Bohemen A, Gibson AJ, Liebster O, Wren BW, Willcocks S, Kendall SL. Resensitization of
to Rifampicin Using CRISPR Interference Demonstrates Its Utility for the Study of Non-essential Drug Resistance Traits.
2020; 11: 619427 [PMID: 33597931 DOI: 10.3389/fmicb.2020.619427]
108 Lakhani P, Sundaram B. Deep Learning at Chest Radiography: Automated Classification of Pulmonary Tuberculosis by Using Convolutional Neural Networks.
2017; 284: 574-582 [PMID: 28436741 DOI: 10.1148/radiol.2017162326]
109 Vonasek B, Ness T, Takwoingi Y, Kay AW, van Wyk SS, Ouellette L, Marais BJ, Steingart KR, Mandalakas AM. Screening tests for active pulmonary tuberculosis in children.
2021; 6: CD013693 [PMID: 34180536 DOI: 10.1002/14651858.CD013693.pub2]
110 Shivam A. Edge Computing vs Cloud Computing: What are the Differences. [cited 20 January 2022]. Available from: https://www.simplilearn.com/edge-computing-vs-cloud-computing-article
111 McMahan B, Ramage D. Federated Learning: Collaborative Machine Learning without Centralized Training Data. Google AI Blog [Internet]. Google, 2017. Introducing an additional approach: Federated Learning. [cited 20 January 2022]. Available from: https://ai.googleblog.com/2017/04/federated-learning-collaborative.html
112 Dean JG, Ghemawat S. MapReduce: Simplified Data Processing on Large Clusters. Sixth Symposium on Operating System Design and Implementation. San Francisco: Google Inc, 2004. [cited 20 January 2022]. Available from: https://static.googleusercontent.com/media/research.google.com/en//archive/mapreduce-osdi04.pdf
113 Ng D, Lan X, Yao MM, Chan WP, Feng M. Federated learning: a collaborative effort to achieve better medical imaging models for individual sites that have small labelled datasets.
2021; 11: 852-857 [PMID: 33532283 DOI: 10.21037/qims-20-595]
114 Sheller MJ, Edwards B, Reina GA, Martin J, Pati S, Kotrotsou A, Milchenko M, Xu W, Marcus D, Colen RR, Bakas S. Federated learning in medicine: facilitating multi-institutional collaborations without sharing patient data.
2020; 10: 12598 [PMID: 32724046 DOI: 10.1038/s41598-020-69250-1]
115 Navia-Vazquez A, Vazquez-Lopez M, and Cid-Sueiro J. Double Confidential Federated Machine Learning Logistic Regression for Industrial Data Platforms. In: 37th International Conference on Machine Learning Vienna 2020, Vienna. [cited 20 January 2022]. Available from: https://www.tsc.uc3m.es/~navia/FL-ICML2020/DCFML-FL_ICML2020-A_Navia_Vazquez_et_al.pdf
116 Wikipedia. Quantum Microsocpy. [cited 20 January 2022]. Available from: https://en.wikipedia.org/wiki/Quantum_microscopy
117 Studio TB. [cited 20 January 2022]. Available from: https://techcrunch.com/sponsor/qualcomm/the-future-is-not-theinternet-of-things-it-is-the-connected-intelligent-edge/
118 Ono T, Okamoto R, Takeuchi S. An entanglement-enhanced microscope.
2013; 4: 2426 [PMID: 24026165]
119 Optics. org. Project QUILT reveals far-reaching potential of quantum optics and imaging. [cited 20 January 2022]. Available from: https://optics.org/news/13/1/4 (2022)
120 Fraenhofer-Gesellschaft. Quantum imaging: Pushing the boundaries of optics. [cited 20 January 2022]. Available from: https://phys.org/news/2022-01-quantum-imaging-boundaries-optics.html
121 Shor PW. Algorithms for quantum computation: discrete logarithms and factoring. In: Proceedings 35th Annual Symposium on Foundations of Computer Science 1994: 124-134 [cited 20 January 2022]. Available from: https://ieeexplore.ieee.org/document/365700
122 Sharma M. There’s been another huge quantum computing breakthrough. [cited 20 January 2022]. Available from: https://www.mckinsey.com/business-functions/mckinsey-digital/our-insights/quantum-computing-use-cases-are-gettingreal-what-you-need-to-know
123 Tung L. Quantum computing: Forget about qubits, here come qutrits. [cited 20 January 2022]. Available from: https://www.zdnet.com/article/quantum-computing-now-rigetti-explores-qutrits-as-well-as-qubits/
124 Oikawa A, Ota A. Quantum computing: Japan takes step toward light-based technology. [cited 20 January 2022]. Available from: https://asia.nikkei.com/Business/Technology/Quantum-computing-Japan-takes-step-toward-light-basedtechnology
125 Kahn J. Microsoft Quantum Algorithm Boosts Medical Imaging. [cited 20 January 2022]. Available from: https://fortune.com/2019/07/15/microsoft-quantum-algorithm-boosts-medical-imaging
126 Charles Q, Choi AI. Fuses With Quantum Computing in Promising New Memristor Quantum device points the way toward an exponential boost in “smart” computing capabilities. [cited 20 January 2022]. Available from: https://spectrum.ieee.org/quantum-memristor
127 Spagnolo M, Morris J, Piacentini S. Experimental photonic quantum memristor.
2022; 16: 318-323 [cited 20 January 2022]. Available from: https://www.nature.com/articles/s41566
 World Journal of Radiology2022年6期
World Journal of Radiology2022年6期
- World Journal of Radiology的其它文章
- Comments on "Neonatal infratentorial subdural hematoma contributing to obstructive hydrocephalus in the setting of therapeutic cooling: A case report"
- Do preoperative pancreatic computed tomography attenuation index and enhancement ratio predict pancreatic fistula after pancreaticoduodenectomy?
- Evaluation of the dual vascular supply patterns in ground-glass nodules with a dynamic volume computed tomography
- Artificial intelligence technologies in nuclear medicine
- Recent advances in imaging techniques of renal masses