
Sequential occurrence of T790M mutation and small cell lung cancer transformation in EGFR-positive lung adenocarcinoma:A case report
2022-06-22 08:37:02ErHongXiErChenJiaMaoJingJingZhouLingChenJiaYiXuWeiTao
World Journal of Clinical Cases 2022年9期
lNTRODUCTlON
Lung carcinoma remains a principal reason for cancer-associated mortality worldwide.However,the treatment strategies for lung cancer,particularly those for non-small cell lung cancer(NSCLC)have undergone revolutionary advancement alongside the emergence of epidermal growth factor receptortyrosine kinase inhibitors(EGFR-TKIs).Within the kinase domain of EGFR,these activating mutations,particularly the deletion of exon 19 as well as the mutation in exon 21(L858R),occur in 10%-15% of Caucasian patients with lung adenocarcinoma and in up to 50% of patients of Asian origin[1].Gefitinib and Erlotinib,which are first-generation EGFR-TKIs or Dacomitinib and Afatinib,which are secondgeneration EGFR-TKIs,have been recommended as the first-line treatment strategy for EGFR mutationpositive NSCLC.Although their effectiveness,as well as safety,have been continuously proven,unfortunately,acquired resistance inevitably emerges,which typically occurs after a median period of 9.2-14.7 mo of TKIs therapy[2].Three mechanistic categories of acquired resistance have been identified: Bypass signaling pathway activation,target gene mutation and histological transformation[3].For firstgeneration EGFR-TKIs,a mutation in EGFR-T790M is the primary mechanism regulating acquired resistance,and is observed in nearly 50%-60% of cases,while 10% of tumors exhibiting EGFR-TKIs resistance transform to small cell lung cancer(SCLC)morphology[2].
Herein,we report a case of NSCLC with EGFR-T790M mutation and conversion to SCLC while treated with EGFR-TKIs.The patient underwent comprehensive treatment,including targeted therapy,platinum-containing chemotherapy,antiangiogenic therapy and immunotherapy,with an overall survival of 24 mo.
In the course of a great many journeys to the forest he carried away many rich stuffs and much fine linen36, and set up a shop opposite that of Ali Baba s son
CASE PRESENTATlON
Chief complaints
A 54-year-old male patient presented to the hospital with dyspnea and productive cough on November 5,2016,without fever,hemoptysis and pleuritic pain.
History of present illness
The patient had continuously reported symptoms which had persisted for more than 5 mo and were gradually aggravated.
History of past illness
They went in, and inside the cottage was a tiny hall, and a beautiful sitting-room4, and a bedroom in which stood a bed, a kitchen and a dining-room all furnished with the best of everything, and fitted up with every kind of tin and copper5 utensil6
As the years went by, the eighteen-month gulf14 separating us closed. Vicki was a voracious15 and indiscriminate reader. What she read set the scene for our dolls. Our mother wouldn t let us play with Barbies. Their bosoms16 are too bodacious, she declared.So we had Tiny Tears dolls instead. Vicki s was Tina; mine was Betsy. We also had a homely17, rubber-faced doll we called Brother Deanie. Depending on what Vicki was reading, Tina and Betsy would rescue the hapless Brother Deanie from a prairie fire (our four-poster bed was the stagecoach), change his diaper at Plymouth Rock or present him to King Arthur s Court. It was wearying to play dolls with other girls, who didn t get it and had to be taught how to talk like a Quaker or an Arabian princess. Now we can play! we d exclaim when they went home.
Personal and family history
The patient denied any relevant personal and family history.
Physical examination
Physical examination showed that the patient's body temperature was 36.6°C,pulse rate was 84 bpm,blood pressure was 126/77 mmHg,respiratory rate was 18 breaths/min,and performance status was 0.
Laboratory examinations
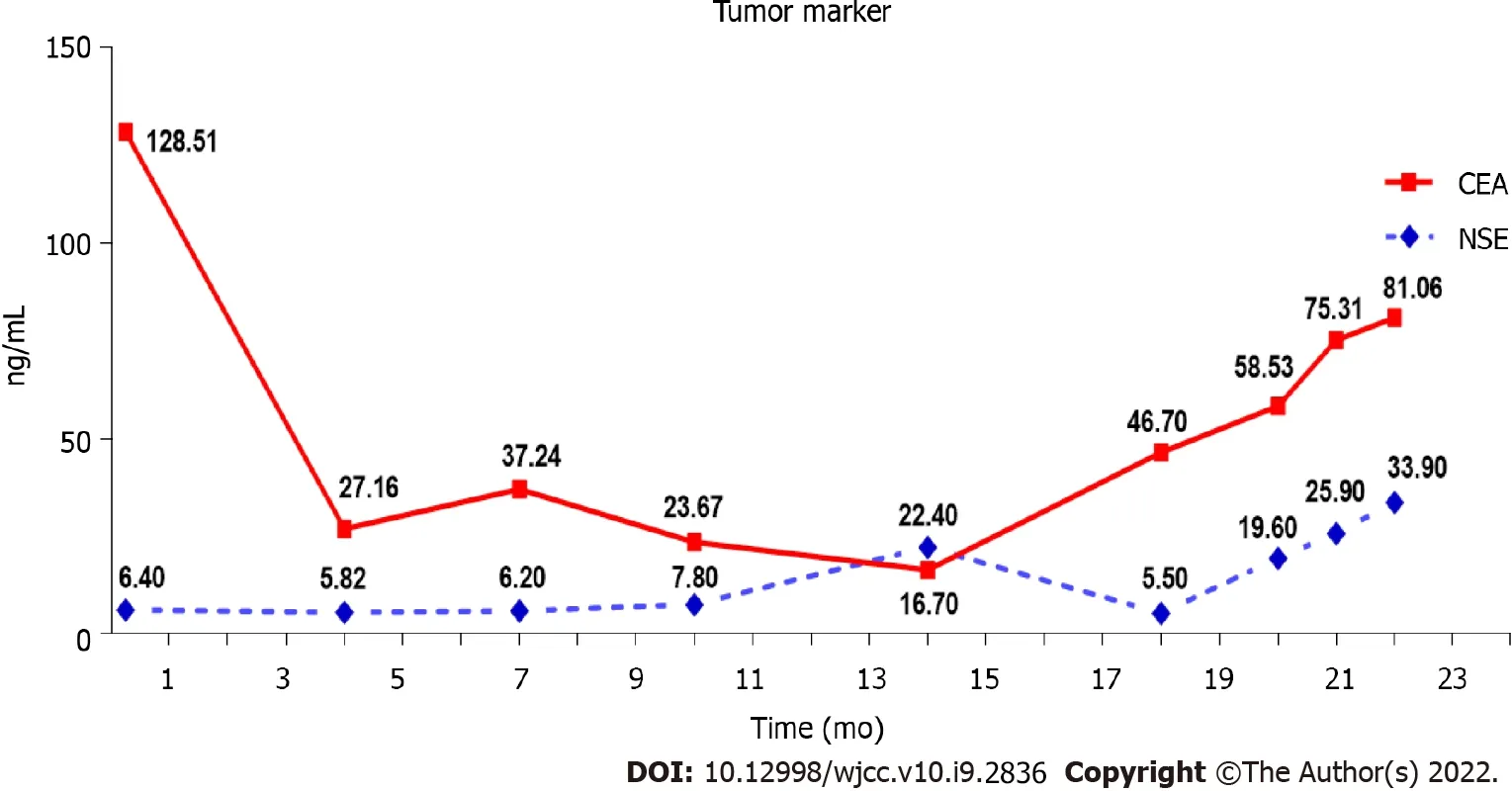
The laboratory results were normal except that the carcinoembryonic antigen(CEA)level was 128.51 ng/mL(the normal range: 0-5.0 ng/mL).
Imaging examinations
Computed tomography(CT)on November 5,2016 revealed a 38 mm × 48 mm tumor in the upper right lobe,with multiple pleural and bilateral pulmonary metastases,mediastinal,and hilar lymphadenopathy(Figure 1A).Cranial magnetic resonance imaging,abdominal ultrasound,and bone emission CT were carried out to confirm the absence of distant metastases.
The patient was diagnosed with stage IV right lung adenocarcinoma bearing a mutation caused by EGFR exon 19 deletion(cT2bN3M1a in accordance with version 8 of TNM staging).
Pathology and genetic testing
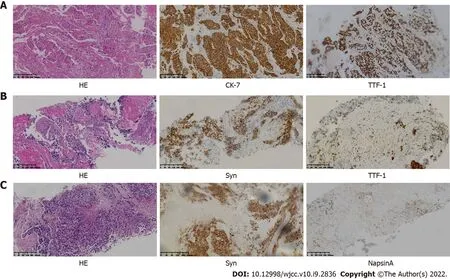
Trans-bronchial biopsy confirmed lung adenocarcinoma on November 10,2016.Immunohistochemical analysis showed positive immunostaining for cytokeratin 7(CK7)and thyroid transcription factor-1(TTF-1)and negative immunostaining for the tumor protein 63(P63),cytokeratin 5/6(CK5/6)and synaptophysin(Syn)(Figure 2A).The amplification refractory mutation system technique identified EGFR exon 19 deletion.
FlNAL DlAGNOSlS
However, the money he obtained in this way enabled him to buy the Queen her flock of sheep, as well as many of the other things which go to make life pleasant, so that they never once regretted their lost kingdom
TREATMENT
As a first-line treatment,250 mg of oral Gefitinib was administered once a day starting on November 17,2016.As per the solid tumor version 1.1(RECIST 1.1)response evaluation criteria,the best efficacy evaluation was a partial response(PR)after 4 mo(Figure 1B).Serum CEA level significantly decreased to 27.16 ng/mL on March 6,2017(Figure 3).After 10.5 mo of progression-free survival(PFS),disease progression was confirmed by CT of the chest on September 3,2017,which demonstrated an enlarged right upper lobe mass and increased metastatic nodules(Figure 1C).Droplet digital PCR(ddPCR)assay was employed to verify the distinct plasma EGFR-T790M.The therapeutic drug AZD9291(80 mg daily),also known as Osimertinib,was used as a second-line treatment on October 4,2017.Unexpectedly,a mixed response was observed after 1 mo,with a growing right upper lobe lesion but the near disappearance of pulmonary metastases(Figure 1D).
We report a patient with sequential occurrence of multiple drug resistance after treatment with gefitinib.Comprehensive treatment regimens according to the drug resistance mechanism significantly improved the prognosis of this patient,including the EGFR-TKIs(Gefitinib,Osimertinib),chemotherapy,antiangiogenic drugs and immunotherapy.In summary,for the majority of patients with TKI-resistance,the resistance mechanisms are largely unknown.Repeated biopsies and application of the dynamic technique for multiple biopsies could disclose more comprehensive resistance mechanisms.Therefore,optimal therapy may be determined accordingly by increasing treatment efficacy and prolonging the duration of survival.

A CT-guided needle puncture of the lesion that had enlarged in size in the upper lobe of the right lung was obtained as the fourth biopsy on September 28,2018 to monitor progression.Interestingly,the morphology of the lung mass showed poorly differentiated mixed histological subtypes of adenocarcinoma and SCLC(Figure 2C).The IHC staining data revealed the following: partially Syn-positive,partially CgA-positive,partially CD56-positive,partially NapsinA-positive,and PD-L1 < 1%(clone 22C3,DAKO,Agilent,Santa Clara,CA,United States).Tissue samples were detectedNGS containing a panel consisting of 420 genes(3D Medicines,Shanghai,China),which revealed EGFR Exon19(mutant abundance: 38.28%),RB1(mutant abundance: 68.48%),TP53(mutant abundance: 76.97%)and tumor mutation burden(TMB): 9.68 Muts/Mb.Nivolumab was added to the previous therapeutic options as a fifth-line treatment on November 1,2018(180 mg intravenously every 2 wk).The entire treatment process is illustrated in Figure 4.
The patient had a history of pulmonary tuberculosis with no history of smoking or malignant tumors.

OUTCOME AND FOLLOW-UP
The inevitable emergence of acquired drug resistance seriously affects the prognosis of patients with NSCLC and mutations having EGFR-sensitivity.The median time to disease progression after initial TKI treatment is 10.2 mo and the most common symptoms are cough and dyspnea[4].Various mechanisms of acquired resistance can be categorized such as the activation of alternative signaling pathways,secondary mutations in EGFR,and phenotypic or histologic transformation[5-7].EGFRT790M mutation is the most common mechanism of acquired resistance,and amounts to 50-60% of resistance acquired during primary EGFR-TKIs therapy[8].Evaluation of EGFR T790M status is imperative for the establishment of first- or second-generation TKI-acquired drug resistance,which is required for the selection of subsequent therapies and later proceeding to clinical trials.Recently,liquid biopsy genotyping of circulating tumor DNA(ctDNA)has become an attractive substitute to re-biopsy of tissues,due to its many potential advantages in comparison to tissue biopsy,such as improved safety of patients,reduced costs,shortened turnaround time,and counteracting the heterogeneity of different metastatic lesions[9].A prospective study revealed that T790M detection based on ctDNA-using ddPCR was up to 77.1% sensitive,with a specificity of 63.2% and a positive predictive value of 79.0%,which indicated an acceptable correlation between tissue re-biopsy and ctDNA[10,11].Due to the presence of tumor heterogeneity,the entire mechanism for resistance cannot be represented by a single tumor biopsy technique.
Well, sir, Grandfather chuckled12, you could practically see what people were thinking. They were the people who were saying to themselves and to everybody else, Well, what did I tell you??And then there were those who made it perfectly13 plain that they thought it was mighty14 tactful() of their host not to make an ostentatious() parade of his money before a lot of neighbors and friends.
DlSCUSSlON
Unfortunately,although the patient underwent the best supportive care due to continuous deterioration in his general condition after 2 cycles of a previous combination treatment(performance status score > 2),he died on December 22,2018.
The scientific community has increasingly acknowledged that EGFR-mutant NSCLC can undergo SCLC transformation[12].The conversion of tumor phenotype has been demonstrated to be a targetindependent drug resistance mechanism.For patients with unsuccessful EGFR-TKIs treatment,up to 10% of tumors have transformed into SCLC[8,13].These transformed tumor cells show similar molecular characteristics to SCLC,including the disappearance of TP53 and RB activity[14,15].Interestingly,these transformed tumors still possess the original EGFR mutation,with a marked reduction in the expression of EGFR,which may suggest that the EGFR signaling pathway is no longer the driving force for the origination of these tumors[14].
In our case,the patient who had advanced lung adenocarcinoma with EGFR 19Del was treated with Gefitinib for a period of 10.0 mo and developed secondary drug resistance.Osimertinib(thirdgeneration TKI)was administered as the second-line TKI treatment at the time of detection of plasma T790M.A dramatic clinical response was observed during treatment with Osimertinib.The main lesion in the right upper lung continued to progress but the metastatic lesions in both lungs significantly regressed.Pathology of the upper right lung lesion biopsy indicated SCLC transformation.The EGFR Exon19 mutation was persistent,while T790M mutation had disappeared as shown by NGS,accompanied by the concurrence of RB1 and TP53 mutations.The above findings suggest that tumor cells tend to successively develop target-dependent and target-independent drug resistance mechanisms due to tumor heterogeneity and TKI selection pressure.
Hong E,Chen XE and Tao W collaborated in data collection,literature review and writing the manuscript;Mao J,Zhou JJ analyzed the data from the patient;Chen L and Xu JY were responsible for the treatment and management of the patient;All authors read and approved the final manuscript.
I see that same twinkle in her eye that I used to see as Roma says, Yes, I will marry you, and we embrace, the embrace we longed to share for so many months, but barbed wire came between us. Now, nothing ever will again.
Marcoux[12]recently reported the largest retrospective investigation comprising 58 patients bearing EGFR-mutant NSCLC that exhibited transformation into SCLC following one or more types of EGFR-TKIs treatments.The median overall survival from the time of diagnosis was found to be 31.5 mo(24.8 to 41.3 mo,95%CI),whereas the median survival time from the initiation of SCLC transformation was 10.9 mo(8.0 to 13.7 mo,95%CI).Following transformation,clinical behavior was identical to classical SCLC in many aspects,with responses to taxanes and platinum-etoposide except for immune checkpoint inhibitors.There is still insufficient evidence for a standard therapy for relapsed SCLC.The unique TKI,Anlotinib has a highly selective inhibitory impact on multiple targets,particularly on fibroblast growth factor receptor,stem cell growth factor receptor(c-Kit),vascular endothelial growth factor receptor,and platelet-derived growth factor receptors,and can inhibit tumor angiogenesis and tumor growth.The outcomes of the ALTER1202 study showed that compared to the placebo arm(4.1 mo0.7 mo;HR = 0.19;0.12-0.32;< 0.0001,95%CI),the median PFS in the Anlotinib arm was considerably prolonged,which should be considered as further-line treatment[16,17].In our case,the response duration for this patient with PR was 5.0 mo,who underwent six cycles of etoposide plus carboplatin after SCLC transformation.The response to treatment for relapsed SCLC with Anlotinib in combination with docetaxel and carboplatin chemotherapy was more than 3.0 mo.Unfortunately,his disease responded less well to Nivolumab.The length of time from the initial diagnosis to transformation was almost 14.0 mo and the patient's overall survival duration was 24.0 mo.
CONCLUSlON
Following 3 mo of Osimertinib treatment,chest CT showed a further enlargement of the right upper lobe lesion(58 mm × 36 mm),a sizable mass in the right lung situated in the middle lobe,a local pleural mass with rib destruction,and an enlarged right axillary lymph node(34 mm × 36 mm)on January 5,2018(Figure 1E),following a 3.0 mo PFS.Blood tests showed an increase in the serum level of neuronspecific enolase(NSE)to 22.4 ng/mL and persistent decreasing levels of CEA to 16.70 ng/mL(Figure 3).Biopsy of the progressive right upper lobe mass was repeated and showed SCLC transformation according to immunohistochemistry(IHC)and revealed the following: positive Syn and TTF-1 expression,and NapsinA-negative(Figure 2B).Tissues were obtained for next-generation sequencing(NGS)using a panel consisting of 80 genes(3D Medicines,Shanghai,China),which revealed EGFR Exon19(mutant abundance 58.00%),RB1(mutant abundance 43.60%),TP53(mutant abundance 82.60%)mutation and disappearance of EGFR-T790M.Intravenous etoposide 100 mg/mfrom the 1d to the 3d,in combination with carboplatin(EC)(with an area of 5 mg/mL/min under the concentration-time curve,administered intravenously every 21 d on day 1)was used as a third-line treatment.Following the four chemotherapy cycles,the serum NSE level markedly decreased to 5.5 ng/mL(Figure 3),and efficacy evaluation was a partial response(Figure 1F).Unfortunately,the disease progressed after six cycles of EC on June 25,2018(Figure 1G).The patient attained a PFS of 5 mo.Oral Anlotinib(12 mg/d,from day 1 to day 14,21 d)plus 75 mg/mdocetaxel(injected intravenously on day 1)and intravenous carboplatin(5 mg/mL/min area under the concentration-time curve every 21 d on day 1)were administered as a fourth-line treatment.Lung lesions were stable for more than 3 mo(Figure 1H).
ACKNOWLEDGEMENTS
We thank the patient and his family for giving permission for his inclusion in this study.
FOOTNOTES
As I walked down the slope towards the beach, in my mind s eyes I could still vividly24 envision the playfully sublime25 look on her face -- her gentle smile and communicative eyes -- even if ten years had passed
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflicts of interest.
The authors have read the CARE Checklist(2016),and the manuscript was prepared and revised according to the CARE Checklist(2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Er Hong 0000-0003-1163-0561;Xi-Er Chen 0000-0003-4089-4689;Jia Mao 0000-0001-6538-2933;Jing-Jing Zhou 0000-0001-9153-3950;Ling Chen 0000-0002-7839-7787;Jia-Yi Xu 0000-0002-5109-0064;Wei Tao 0000-0002-8573-2598.
Wu YXJ
Filipodia
10. First she looked in at the window, and then she peeped in at the keyhole; and seeing nobody in the house, she lifted the latch: Goldilocks doesn t knock on the door first. She cases the joint and then enters when she determines no one is home. These are not the actions of someone planning to do good. These are the actions of someone far from innocent and inexperienced.Return to place in story.
Wu YXJ
 World Journal of Clinical Cases2022年9期
World Journal of Clinical Cases2022年9期
- World Journal of Clinical Cases的其它文章
- Malignant struma ovarii with papillary carcinoma combined with retroperitoneal lymph node metastasis:A case report
- Upper gastrointestinal bleeding from a Mallory-Weiss tear associated with transesophageal echocardiography during successful cardiopulmonary resuscitation:A case report
- lpsilateral hemifacial microsomia with dextrocardia and pulmonary hypoplasia:A case report
- Esophageal myoepithelial carcinoma:Four case reports
- Turner syndrome with primary myelofibrosis,cirrhosis and ovarian cystic mass:A case report
- Acute coronary artery stent thrombosis caused by a spasm:A case report