
Comparing complications of outpatient management of slipped capital femoral epiphysis and Blount’s disease: A database study
2022-05-30 08:01AchrafJardalyTimothyTorrezGeraldMcGwinShawnGilbert
World Journal of Orthopedics 2022年4期
lNTRODUCTlON
In recent years, an increasing number of orthopaedic surgeries have been performed in an outpatient setting[1]. A study examining pediatric fracture trends demonstrated a threefold increase in the use of outpatient services for the surgical fixation of fractures from 1996 to 2006[2]. Though outpatient surgery provides a lower initial cost, several factors like patient safety, complications, and readmissions need to be considered[3].
Obesity in children has reached epidemic proportions. According to the Centers of Disease Control and Prevention, 1 out of 5 individuals less than 19 years of age are obese[4]. As such, it is anticipated that adverse health outcomes related to obesity will increase. From an orthopaedic perspective, childhood obesity is considered to be a significant risk factor for both slipped capital femoral epiphysis (SCFE) and Blount’s disease[5,6]. A better understanding of both diseases and their respective treatment options would benefit children and their families.
Far away in the east country, there lived a king who loved hunting so much that, when once there was a deer in sight, he was careless of his own safety
Later, when she mentioned to her husband how she missed those lilacs, he popped up from his chair. I know where we can find you all you want, he said. Get the kids and c mon.
Despite the surgical options for SCFE and Blount’s disease being well-studied, to our knowledge, there is no literature comparing inpatientoutpatient management of either condition[6,7]. Therefore, we sought to use a large pediatric database to compare the complication and readmission rates between treatment in the inpatient and outpatient setting. Our hypothesis was that there would be no increased risk of adverse outcomes associated with the outpatient treatment of both conditions.
MATERlALS AND METHODS
The American College of Surgeons National Surgical Quality Improvement Program (NSQIP) Pediatric Registry was queried for the years 2015, 2016, and 2017[8]. As information in this database is deidentified and HIPAA compliant, institutional review board approval is not required.
NSQIP prospectively collects data on patient demographics, risk factors, and operative details. The database follows patients for 30 d after surgeries to document discharge status, complications, readmission, and reoperation. The 2017 NSQIP Pediatric database includes 113922 cases from 109 hospitals. Cases with codes corresponding for the International Classification of Diseases, ninth and tenth revisions (ICD-9 and ICD-10) primary diagnosis of SCFE or Blount’s disease were selected. Procedures were defined as outpatient if patients were discharged on the day of the surgery.
In conclusion, our results indicate that performing outpatient surgeries for SCFE and Blount’s disease is a viable option. Careful selection criteria need to be applied, but a large number of children can be surgically-treated as outpatients which does not affect the odds for early postoperative complications or readmissions.
In addition to the common complications documented in the database, we considered a discharge to an acute care setting or facility which was not home as a complication. If a case had multiple related complications, then it was recorded as one complication. For example, a patient with both superficial wound dehiscence and superficial surgical site infection (SSI) was counted as one complication under superficial SSI. No patient had multiple unrelated complications. We included both reoperations and readmissions not requiring an operation in “readmissions.”.
Today we buried our 20-year-old son. He was killed instantly in a motorcycle accident on Friday night. How I wish I had known when I talked to him last that it would be the last time. If I had only known I would have said, Jim, I love you and I m so very proud of you.
Statistical analysis was carried out using IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, N.Y., USA). ANOVA, Wilcoxon signed rank-test, Fisher’s exact tests, andtests were used to compare variables between the outpatient and the inpatient settings. Odds ratios (OR) with 95%CI were calculated when differences in adverse outcomes were exhibited between the inpatient and outpatient settings.values < 0.05 were considered to be statistically significant.
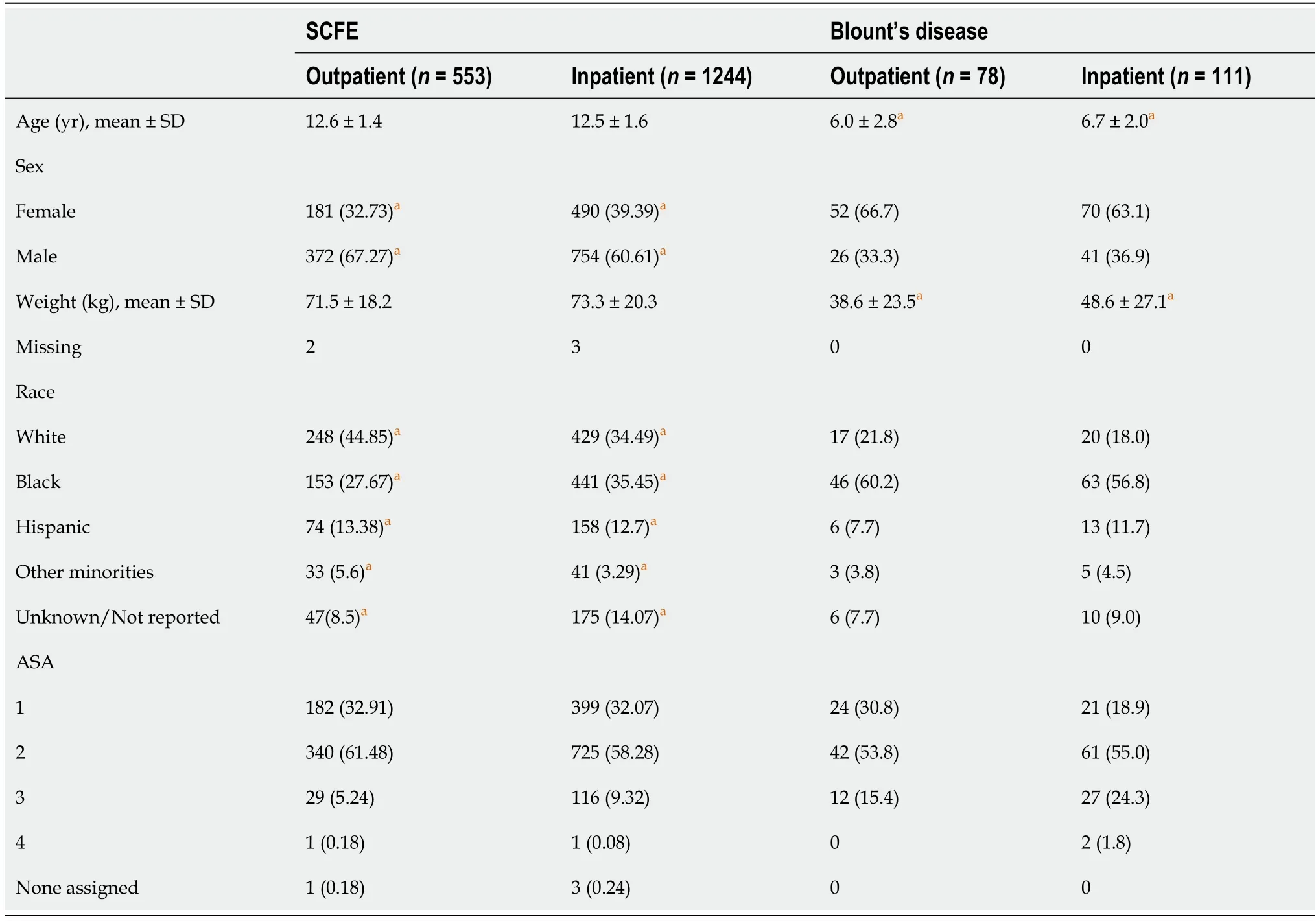
Out of 1797 procedures for SCFE, 46% were performed as an outpatient. 93.6% of children admitted postoperatively were discharged within 3 days, with 47.7% being discharged on postop day (POD) 1 and 39.4% on POD 2. Patients in both settings were similar with respect to age. Small differences existed regarding the weight, sex, and race of patients. There were more males and white patients receiving outpatient surgeries in comparison to the inpatient setting noting more female and black patients. Outpatients had a higher percentage of American Society of Anesthesiologists Classification (ASA) classes 1 and 2 and a lower percentage of ASA class 3 compared to inpatients. Patient details can be found in Table 1.pinning was the most common procedure, constituting 98.5% of outpatient surgeries and 87.8% of inpatient surgeries (< 0.0001).
RESULTS
SCFE
But the host went around as if he didn t notice anything, though Grandfather always insisted that he detected a little twinkle in the rich man s eyes as he shook hands with all his fellow parishioners and wished them good night.
Careful patient selection is still needed to limit complications and readmissions. Patients with ASA 1 or 2 are considered suitable for outpatient surgery[17]. 90.3% of all the patients included in this study meet this requirement. Those with ASA 3 can still receive outpatient surgery, but they might have an increased risk of admission[17]. In addition, attention should be given to comorbidities and prior surgical or anesthetic complications. Nonetheless, a large portion of children with SCFE and Blount’s disease can benefit from outpatient surgery.
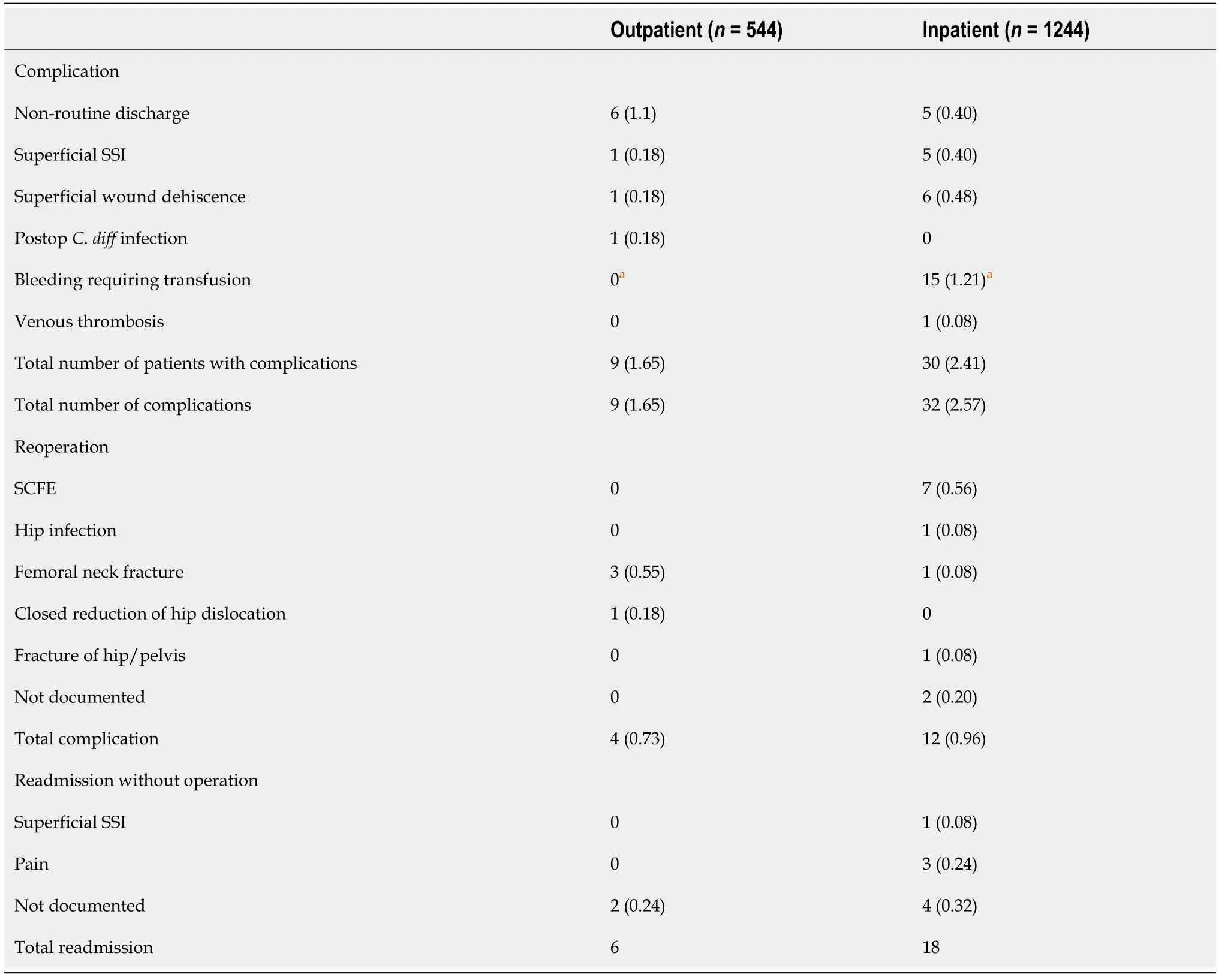
There were 3.5x the total number of complications in the inpatient SCFE group but the mean number of complications between the two groups was not significant (= 0.292). There were 3.3x the number patients that developed complications but OR was not statistically significant (OR = 0.66, 95%CI: 0.31-1.41). Similarly, no difference was found regarding odds of readmission (OR = 1.12, 95%CI: 0.20-6.16).
Blount’s disease
Total 189 procedures for Blount’s disease were included. 41.2% were performed in an outpatient setting. 54.1% of admitted patients were discharged on POD 1, and 30.6% were discharged on POD 2. Patients in both settings had similar sex, race, BMI, and ASA distributions, but statistically significant differences were found in their age. Outpatients were younger by (0.7 year) (Table 1). There were also differences in the procedures used in both settings (< 0.0001). Osteotomy was the most common procedure among inpatients (64%), whereas it was not performed in an outpatient setting. 98.7% of outpatients were treated with physeal arrest, as compared to 34.2% of inpatients.1.3% of inpatients and 1.8% of outpatients were treated with external fixation.
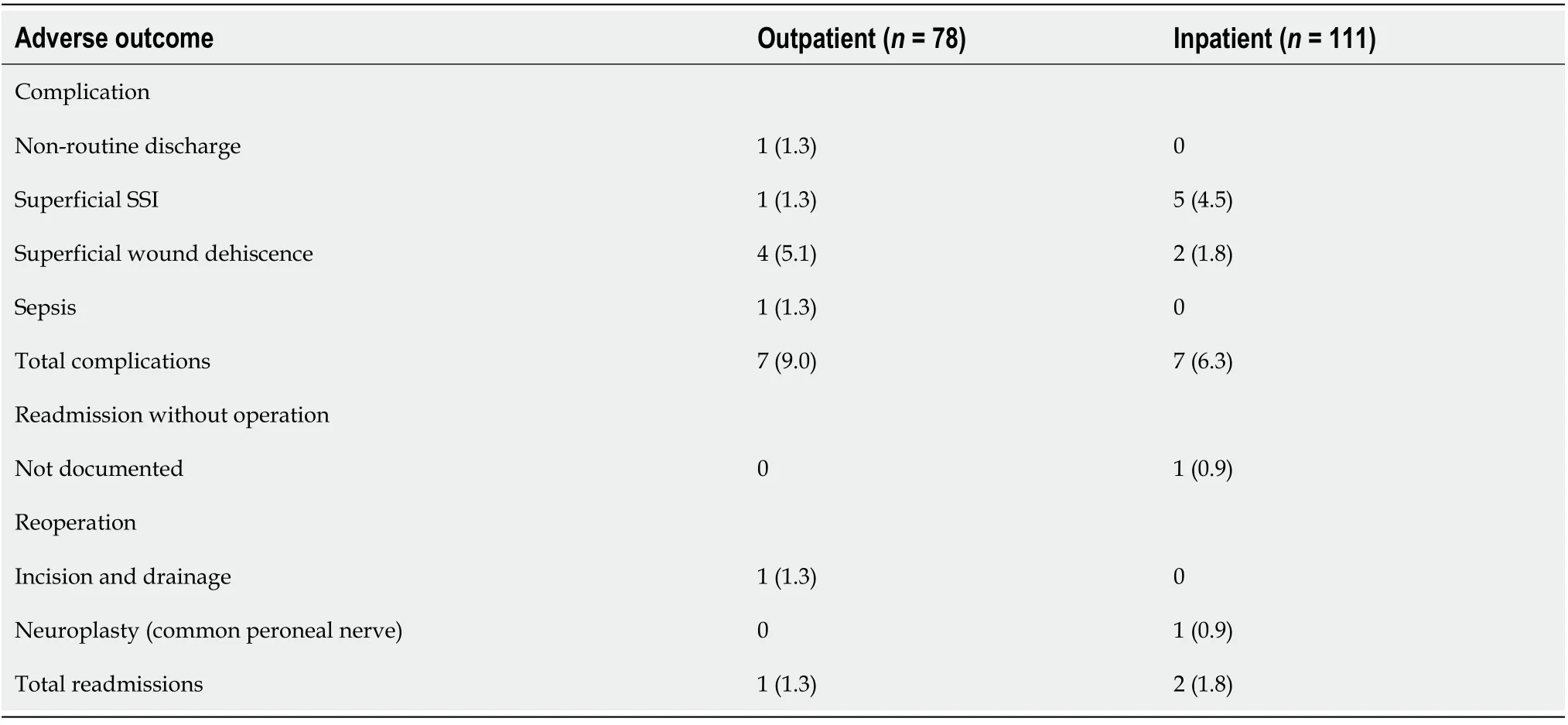
7 .4% of patients experienced complications (Table 3). Superficial SSI and wound dehiscence were the most frequent complications. Individual and total risk of complications and readmissions were not different between both settings (> 0.05) so no ORs were calculated.
DlSCUSSlON
There is a shifting trend towards performing procedures in an outpatient setting[9]. In the current study based on results from the NSQIP Pediatric database, 46% of SCFE procedures and 41% of Blount’s procedures were performed as outpatients.
Several studies report a decline in the incidence of SCFE[10-12]. As obesity rates have been increasing, it is unusual for fewer children to suffer from SCFE. One thing to consider is the methodology of the studies, which rely on databases. Most large registries report inpatient admissions. Same-day surgeries and procedures performed in ambulatory surgery centers are more difficult to capture, but the shift towards outpatient surgery could contribute to the apparent decrease in the incidence of SCFE. In 2000, outpatient SCFE procedures represented 23% of operatively treated SCFEs[13]. This percentage more than doubled according to our results. In addition, NSQIP does not include data from ambulatory centers, so outpatient procedures might constitute more than half of all SCFE surgical correction. Future studies investigating the true incidence of SCFE with outpatient adjustment would provide valuable information.
Surgery for Blount’s disease, though technically difficult, is not commonly associated with major complications other than recurrence[24]. Infections, nerve injuries, and compartment syndromes can still occur[25]. 7.4% of Blount’s patients had a complication in this study, most commonly superficial SSI and wound dehiscence. Patients selected to be treated in an outpatient setting can benefit from education about meticulous wound care and early signs of infection, and our results showed that rates of infections and overall complications were not different between both settings. This confirms our hypothesis that outpatient procedures are not associated with increased morbidity.
Jardaly A contributed to the manuscript preparation, data collection, revisions; Torrez TW contributed to the manuscript preparation, data collection, revisions; McGwin G contributed to the data analysis and statistics; Gilbert SR contributed to the manuscript preparation and was the principal investigator.
Disease-specific and surgery-specific considerations also need to be investigated. One such consideration is the early return to weight-bearing which could increase the risk of femoral neck fractures in patients with SCFE[22]. Femur fractures in our SCFE population were rare and did not differ significantly based on the treatment setting. Nonetheless, for unstable slips where physician judgment deems strict non-weight-bearing to be necessary, patients might benefit from hospital admission (with inpatient physical therapy) to help enforce weight-bearing restrictions when compliance is an issue. The most common complications of SCFE include osteonecrosis, chondrolysis, fixation failure, and slip progression[23]. Osteonecrosis and chondrolysis are largely related to the nature of the slips rather than the surgical approach[23]. 0.56% of patients required a reoperation for SCFE, indicating fixation failure and/or slip progression. This rate was not different based on the setting of the surgery. Other common complications like SSI and wound dehiscence were also similar between the groups. The only individual complication that was different between both groups was bleeding requiring a transfusion. However, this was confounded with open procedures. Open procedures are more invasive, and bleeding is a well-known complication[7]. Such procedures are reserved for severe slips requiring more complex procedures, and it is recommended that they be admitted for inpatient monitoring. After adjusting the analysis for the type of surgery, the inpatient and outpatient settings did not have different odds ratio of complications or readmissions.
Performing procedures in an outpatient setting has several advantages. One significant benefit is the lower patient and hospital cost associated with early patient discharge[14]. In addition, several studies showed that patient satisfaction is inversely correlated with the length of hospital stay[15]. A study comparing inpatients and outpatients satisfaction following hip and knee arthroplasty demonstrated that satisfaction was high in both groups, but in areas of differences, outpatients had higher scores[16]. For children, this effect might be more pronounced, and performing outpatient surgeries can benefit their psychological well-being[17]. However, outpatient surgeries can have higher rates of adverse outcomes in some contexts, particularly with SSI[18]. Arshi[19] found that outpatient total knee arthroplasties had a higher chance of revision compared with inpatient care. Therefore, comparative studies for specific conditions are needed in this area.
Suddenly, it dawned on me that I was dog-tired. I simply couldn t work as long as I could when I was younger. I ve got to rest for a minute, I told my husband, Roy, as I collapsed2 into my favorite rocking chair. Music was playing, my dog and cat were chasing each other and the telephone rang.
Total 1.6% of outpatients and 1.2% of inpatients had complications (= 0.50), and the readmissions rates were 1.1% and 1.44%, respectively (= 0.89). The nature of complications and causes of readmission are found in Table 2. There was no statistically significant difference in individual adverse outcomes except for bleeding. Bleeding was the most common complication among inpatients and did not occur in outpatients. None of these patients had a preoperative bleeding disorder. 12 of the 15 cases of bleeding requiring transfusion occurred with open procedures (Osteotomy and internal fixation) while 3 occurred during in situ pinning (< 0.0083). The overall risks of SCFE recurrence and femoral neck fractures for outpatient and inpatient was 0.55% and 0.64% respectively. Three inpatients initially discharged on POD 1 required readmission for postop pain management.
To capture a large number of procedures, we used the NSQIP Pediatric Database. This is not without limitations. Data collected was from numerous hospitals, so there could be differences in the surgical techniques, indications for surgery, and selection criteria for inpatientoutpatient procedures. Also, all cases included are surgeries performed in a hospital setting. Cases from ambulatory surgery centers are not part of the database. This means that even more procedures are performed in the outpatient setting. However, numerous studies have shown that ambulatory centers have similar outcomes to hospital outpatients, so the conclusion that outpatient surgery does not increase the risk of complications is not undermined[25,26]. In addition, patients were followed for 30 d. Long term complications like growth arrest and femoroacetabular impingement for SCFE and recurrence of Blount’s disease may differ. Symptoms before and after surgery are not available. Despite these limitations, this study provides a representative sample of surgically managed cases of SCFE and Blount’s disease and is the first to investigate short-term readmission and complication rates between of these outpatient procedures. Additionally, the prospective data collection and a priori definitions of complications improve the quality of data regarding complications compared to retrospective data collection or databases utilizing only coded complications.
CONCLUSlON
For SCFE, patients from 9 to 16 years were included. Treatment options were divided intopinning and open treatment. Open treatment includes osteotomy, open reduction, and internal fixation. For pediatric Blount’s disease, patients older than 10 years were excluded. Treatment was categorized as external fixation, osteotomy, or physeal arrest. Osteotomy includes proximal tibial osteotomy with or without fibular osteotomy or excision. Physeal arrest includes epiphysiodesis and hemiepiphysiodesis with any method (guided growth). Patients were excluded if their primary surgery was not congruent with their primary diagnosis (distal femur lengthening for SCFE, or tumor/cyst excision for Blount’s disease).
ARTlCLE HlGHLlGHTS
Research background
Currents trends in pediatric orthopaedics has seen an increase in surgeries being successfully completed in an outpatient setting.
Helen the Beautiful, being roughly awakened, and seeing Tsarevitch Ivan dead, was greatly frightened and cried with bitter tears: I am the Tsar s daughter, Helen the Beautiful, and I belong to Tsarevitch Ivan whom ye have put to a cruel death. If ye were brave knights41, ye had ridden against him in the open field; then might ye have been victorious42 over him with honor; but instead of that ye have slain43 him when he was asleep. What praise will such an act receive?
Research motivation
Limited data is available on safety and efficacy of managing slipped capital femoral epipphysis and Blount’s disease in the outpatient setting.
37. Her girdle: In this instance, a girdle is a band of material around the waist that strengthens a skirt or trousers (WordNet). The girdle is not part of her underwear but an outer garment, often embroidered or decorated for women. The girdle would be one of her more valuable articles of clothing.Return to place in story.
Research objectives
Is outpatient management safe and effective for slipped capital femoral epipphysis and Blount’s disease in the outpatient setting.
Research methods
Retrospective analysis of a large multi-institutional database.
The little hyaena gazed at him in surprise, saying to herself, What! was it really this tiny beast who put to death all our best people? when suddenly a gust37 of wind rustled38 the reeds that surrounded the enclosure, and the little hare, in a fright, hastily sprang back into Big Lion s skin
After five or six months of hearing the mail orderly - announcing the availability of To any service member” mail, I decided5 to take a few of the letters. I planned, as time permitted, to drop them a line telling them Thanks for their support.
Research results
In summary complications were minimal in outpatient surgical management for slipped capital femoral epiphysis and Blount’s disease in the outpatient setting.
Research conclusions
Surgeons should consider outpatient management for both slipped capital femoral epiphysis and Blount’s disease.
Research perspectives
This study should prompt future research in outcomes of outpatient management of other previous inpatient pediatric orthopaedic procedures.
Then one hug changed all that. One month before my 40th birthday my dad had heart surgery. As he came round, days later, he grabbed me and hugged me so hard I had to push with all my might to keep my head from pressing down on his newly stitched torso() .
Though an outpatient setting is an attractive option for patients and physicians, postoperative pain needs be considered[17]. Previous studies showed that children discharged home at the day of surgery had higher pain score than inpatients[20]. Even in admitted patients, Mather and Mackie reported that 17% of children had severe pain on POD 1[21]. In the present analysis, only 3 SCFE patients (0.24%) required readmission for pain. These patients were initially discharged on POD 1. None of the SCFE outpatients or any patients treated for Blount’s disease had pain requiring readmission. Therefore, it is possible for the vast majority of surgical patients to benefit from early discharge without the need for inpatient management of pain. Techniques for anesthesia have improved significantly, and adequate postoperative analgesia can be achieved by giving caregivers ample pediatric-specific instructions and using multimodal medications[20].
This study was institutional review board exempt.
Informed consent was waived as per the University of Alabama at Birmingham’s IRB guidelines.
The authors do not endorse any conflict of interests.
Technical appendix, statistical code, and dataset available from the corresponding author at achraf.jardaly@lau.edu.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
The night before Easter, we were so excited we could hardly sleep. We didn’t care that we wouldn’t have new clothes for Easter; we had seventy dollars for the sacrificial offering. We could hardly wait to get to church! On Sunday morning, rain was pouring. We didn’t own an umbrella, and the church was over a mile from our home, but it didn’t seem to matter how wet we got. Darlene had cardboard7 in her shoes to fill the holes. The cardboard came apart, and her feet got wet.
United States
Achraf Jardaly 0000-0003-2779-9994; Timothy W Torrez 0000-0002-5929-3608; Gerald McGwin 0000-0001-9592-1133; Shawn R Gilbert 0000-0002-0683-3172.
Wang JL
A
Wang JL
 World Journal of Orthopedics2022年4期
World Journal of Orthopedics2022年4期
- World Journal of Orthopedics的其它文章
- Antibiotic-free antimicrobial poly (methyl methacrylate) bone cements: A state-of-the-art review
- Lateral epicondylitis: New trends and challenges in treatment
- ls it necessary to fuse to the pelvis when correcting scoliosis in cerebral palsy?
- Minimally invasive outpatient management of iliopsoas muscle abscess in complicated spondylodiscitis
- Direct anterior approach hip arthroplasty: How to reduce complications - A 10-years single center experience and literature review
- lntegrity of the hip capsule measured with magnetic resonance imaging after capsular repair or unrepaired capsulotomy in hip arthroscopy