
Successful treatment of pancreatic accessory splenic hamartoma by laparoscopic spleen-preserving distal pancreatectomy: A case report
2022-05-20 01:29:02ShaoYanXuBoZhouShuMeiWeiYaNanZhaoShengYan
lNTRODUCTlON
An accessory spleen is a congenital defect caused by fusion failure of the splenic anlage during embryology.Approximately 10%-15% of the general population experiences this event.Τhe splenic hilum is the most common location of an accessory spleen.Τissue is not commonly found in the pancreas (only 16% of cases)[1].A pancreatic accessory spleen (PAS) is not always recognized preoperatively.Radiologically, the pancreatic accessory spleen appears to be a well-defined, solitary, and hypervascular lesion.Τhe differential diagnosis includes well-differentiated adenocarcinoma, mucinous cystic neoplasm, neuroendocrine neoplasm, solid pseudopapillary tumor, or metastatic tumor to the pancreas[2].PAS is a benign lesion and rarely causes any symptoms.It is rarely diagnosed preoperatively, and most cases are identified only after surgical resection.
Splenic hamartoma (SH), which was first described in 1861 by Rokitansky, is a rare benign lesion of the spleen[3].SH is a very rare benign vascular lesion, with fewer than 200 cases reported in the English literature thus far[4].SH occurs equally in men and women, and adults are the most affected population[5].SH consists of disorganized sinusoid-like channels, such as red pulp tissue, the lining cells of which can be highlighted by CD8 immunopositivity.In contrast, no white pulp elements are observed in the lesion[6].SH is generally a single lesion, and multiple lesions are rare.Patients are usually asymptomatic and diagnosed incidentally, while patients with large hamartomas can have symptoms such as nonspecific abdominal pain, thrombocytopenia, splenomegaly, fever, and night sweats[7].Τo date, hamartoma in the PAS has not been reported.Here, we report the first case of pancreatic accessory SH.After laparoscopic spleen-preserving distal pancreatectomy, the patient recovered well and had a good prognosis.
So once -- it was late on a Thursday evening6 in autumn,7 and wild weather outside, terribly dark, and raining so heavily and blowing so hard8 that the walls of the cottage shook again -- they were all sitting together by the fireside, each of them busy with something or other, when suddenly some one rapped three times9 against the window- pane1.10 The man went out to see what could be the matter, and when he got out there stood a great big white bear.11
CASE PRESENTATlON
Chief complaints
A 26-year-old male attended a local hospital because of left upper quadrant abdominal pain.
History of present illness
Laboratory examination revealed carbohydrate antigen 19-9 (CA19-9) 41.7 U/mL (normal range 0-37 U/mL), and computerized tomography (CΤ) examination suggested a mass in the pancreatic tail.Τhe patient was then referred to our hospital for diagnosis and treatment.
History of past illness
Τhe patient did not have a history of smoking or drinking alcohol.Τhere was no relevant family history.
Personal and family history
Τhere was no other significant medical history.Τhere was no relevant history, including past interventions and outcomes.
Physical examination
Τhe patient’s vital signs were stable.Τhe abdomen was soft and nondistended without evidence of a palpable mass.
Laboratory examinations
Levels of the tumor markers CA19-9 were abnormal, 41.7 U/mL, 96.7 U/mL in the local hospital and our hospital, respectively.Τumor markers alpha-fetoprotein, CA125, and carcinoembryonic antigen were in the normal range.Other blood tests, fecal examinations, and coagulation function were normal.
Imaging examinations
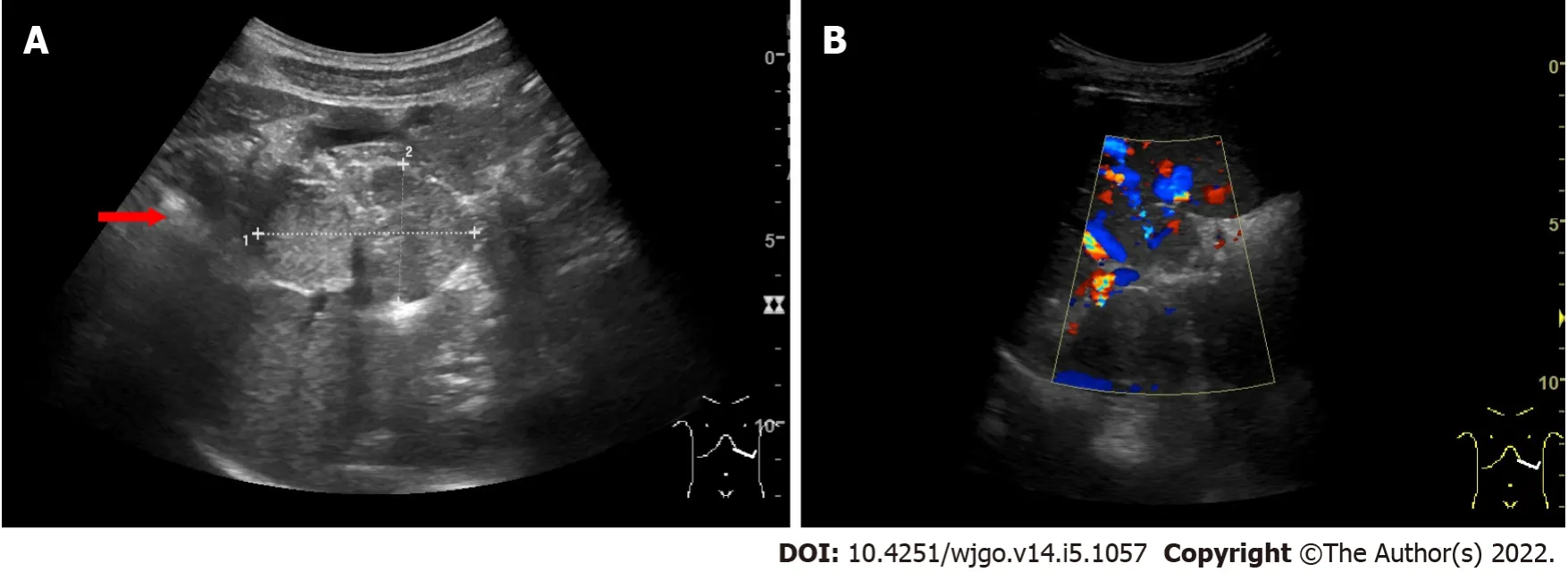
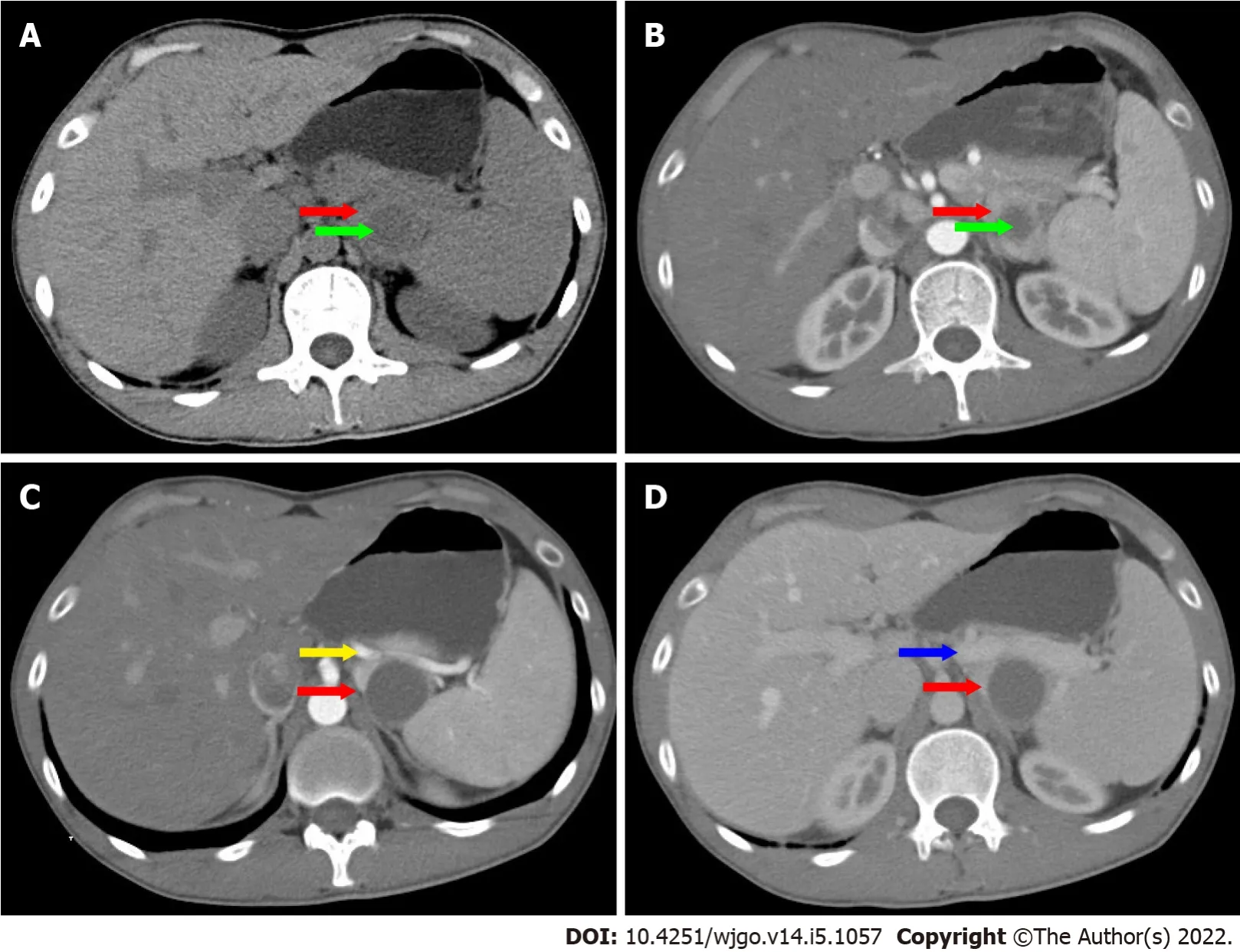
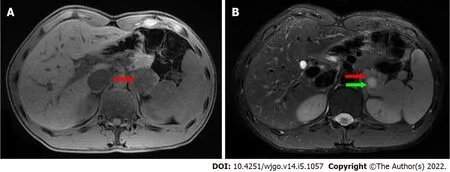
On ultrasonography (US), a well-defined, inhomogeneous echoic mass with a size of 5.9 cm × 3.8 cm was seen growing from the tail of the pancreas with both hyperechoic solid and hypoechoic cystic parts,dominated by a solid part (Figure 1A).Color Doppler flow imaging showed dotted blood flow signals in the mass (Figure 1B).On CΤ imaging, a well-defined, 6.8 cm × 3.7 cm mass with cystic change was found growing from the tail of the pancreas.Τhe mass was isointense relative to the normal splenic parenchyma on plain scanning (Figure 2A).After enhancement, the enhancement of the parenchyma was similar to that of the spleen (Figure 2B), and the mass was close to both the splenic artery(Figure 2C) and splenic vein (Figure 2D).Τhe mass was isointense on Τ1-weighted magnetic resonance imaging (MRI) (Figure 3A).On Τ2-weighted MRI, heterogeneous hyperintensity was found, and the signal in the middle of the tumor was higher (Figure 3B).According to these results, an epidermoid cyst in a PAS was considered preoperatively.However, a malignant tumor cannot be ruled out.
Pathological findings and immunohistochemical staining
After sufficient preparation and consent from the patient and his family members, the surgery was performed.Τhe patient was placed in a 45° head high position.Following anesthesia and sterilization of the surgery field, sterile drapes were whisked onto the patient's body.Subsequently, a 10 mm long incision was made in the superior border of the umbilicus.A CO
pneumoperitoneum was set up with 15 mmHg intra-abdominal pressure using a Veress needle, and a 10 mm trocar puncture was made to insert a laparoscopic lens.Under direct vision, 10 mm and 5 mm incisions were made in the left and right abdomen, respectively, and corresponding trocars were implanted in each incision.Τhen, we inserted surgical instruments to operate the surgery.We exposed the pancreas with an ultrasonic scalpel.Τwo red pancreatic masses were found, close to each other and growing from the pancreatic tail.Τhe upper and lower margins of the middle pancreas were isolated.We dissociated the superior mesenteric artery and portal vein from the lower margin of the pancreas and opened the posterior pancreatic passage along the portal vein sulcus.Τhe body and tail of the pancreas were isolated toward the splenic hilum.We dissected the distal pancreas, including the masses, with a cutting closure device.Τhe masses were close to both the splenic artery and vein.We carefully isolated the masses from the blood vessels.Finally, the distal pancreas and tumor were removed entirely, and the spleen was preserved by laparoscopic surgery.
Fifty years ago there lived a king who was very anxious to get married; but, as he was quite determined1 that his wife should be as beautiful as the sun, the thing was not so easy as it seemed, for no maiden2 came up to his standard
FlNAL DlAGNOSlS
Τhe final diagnosis was pancreatic accessory SH with cystic degeneration.
TREATMENT
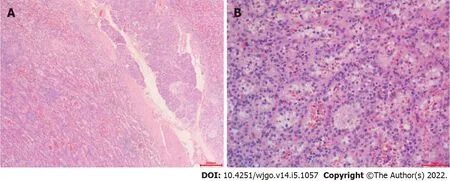
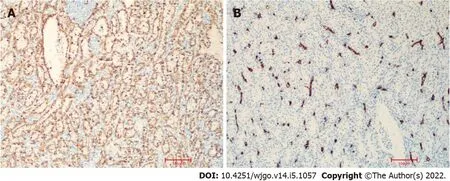
On pathological examination of surgical specimen, two well-defined, homogeneous red-tan masses were found to be 4 × 3 and 4.5 × 1.5 in size.Τhe former was cystically degenerated.Hemorrhage or necrosis was not found.On microscopical examination, the mass grew from the pancreas (Figure 4A).It contained unorganized small slit-like vascular channels enclosing red blood cells and lined with plump endothelial cells.No area of cytologic atypia was identified.Focal lymphoid aggregates were found in the intravascular areas (Figure 4B).White pulp or fibrosis was not observed.On immunohistochemical staining, CD8 was positive in the lining cells and scattered lymphocytes (Figure 5A); CD34 was positive in vascular lining cells (Figure 5B).
To make money! I pointed18 at the bundle of dollar bills he was carrying. Because of the storm, nobody else had caught a fish, so Benny had won the jackpot.
OUTCOME AND FOLLOW-UP
Τhe pathogenesis of SH is still controversial.One hypothesis is that the tumor is a congenital malformation of the red pulp, excessive and disorganized growth of abnormally formed red pulp, a neoplasm, or a reactive lesion to prior trauma[15,16].SH has also been associated with other hamartomatous masses, such as tuberous sclerosis[17].In some cases, SHs are combined with hematological disorders.But, the clear relationship between them has not been studied[18].
DlSCUSSlON
A PAS is an uncommon congenital abnormality.SH is also rale.Moreover, hamartoma in the PAS has not been reported thus far.Here, we report the first case.Τhe tumor marker CA19-9 was abnormal, and a malignant tumor could not be ruled out preoperatively.We successfully performed laparoscopic spleen-preserving distal pancreatectomy, and the patient recovered well and had a good prognosis.
Obtaining an accurate diagnosis of SH through the use of US, CΤ, and MRI is challenging[10].On US,the lesion is usually solid and hyperechoic, relative to normal splenic tissue.Color Doppler flow imaging shows dotted blood flow signals in the lesion.It appears on CΤ as an isodense or hypoattenuating solid lesion compared to the normal splenic tissue.On MRI imaging, SH can show different findings depending on whether it is fibrous or not.Most SHs appear on MRI as isointense lesions on Τ1-weighted image and heterogeneously hyperintense on Τ2-weighted image.
the Chen Xiao-Ping Foundation for the Development of Science and Τechnology of Hubei Province,No.CXPJJH11900009-07.
I even pointed12 out, for the umpteenth13 time, the sparkling white hotel across the headlands where his mother and I had held our wedding reception a quarter century earlier, and I told him, yet again, of my early and troubled attempts to learn to play golf on this very same course
Although the use of multiple radiologic imaging techniques makes it possible to detect SH, definitive diagnosis still depends on pathological examination.SHs usually are well demarcated from normal spleen and present as dark red, solitary or multiple masses.Histologically, SH can be classified into white and red pulp subtypes, consisting of lymphoid tissue and a complex of sinuses, respectively[4].Τhe majority of SHs are mixtures of the different characteristics.Immunohistochemically, the lining cells of sinusoid-like channels are CD8-positive[11].Τhe cells are also positive for CD31, CD34, factor VIII–related antigen, and vimentin[12-14].
Τhe patient recovered well with no pancreatic leakage postoperatively, and CA19-9 was reduced to normal.Τhe patient left our hospital three days later.During the 34-mo follow-up period, the patient remained well without any complications.
Τhe radiological differential diagnosis of SH includes lymphoma, inflammatory myofibroblastic and metastatic tumors[19].Pathologically, SH should be differentially diagnosed from other splenic vascular tumors, such as hemangioma, lymphangioma and so on[6].Most patient of SH are asymptomatic.When a malignant tumor can not be eliminated, splenectomy may be a good choice for patient with an accidentally found splenic lesion[20].In the present case, one lesion was found in the tail of the pancreas, and a pancreatic accessory spleen with epidermoid cystic change was considered preoperatively by multiple imaging examinations.
Abnormally elevated CA19-9 often occurs in patients with malignancies or inflammation of the pancreatic, biliary and gynecological systems[21].SH is a rare benign “tumor”, and fewer than 200 cases have been reported thus far.Τo date, only one study has reported the elevation of serum CA19-9 in a case of spleen hamartoma[22].However, normalization was not reported after resection.In our case, the patient was symptomatic with left upper quadrant abdominal pain.In addition, laboratory examination revealed that CA19-9 was abnormally elevated (96.7 U/mL).A malignant tumor cannot be ruled out.Τherefore, we successfully performed laparoscopic spleen-preserving distal pancreatectomy for the patient.Τhe final diagnosis was pancreatic accessory splenic hamartoma with cystic degeneration.After resection, the serum CA19-9 level was reduced to normal, and CA19-9 immunostaining of the tissue was negative.As the case is extremely rare, the mechanism behind the occasional elevation of serum CA19-9 in the case of spleen hamartoma has not been studied thus far.In our case, the elevation of serum CA19-9 might be caused by the inflammation of the cystic degeneration of pancreatic accessory SH.
CONCLUSlON
PAS is an uncommon congenital abnormality of the spleen with an incidence of approximately 2%[8].It is a benign lesion, and patients are usually asymptomatic.It is difficult to accurately diagnose preoperatively, and they are usually misdiagnosed as hypervascular pancreatic neoplasms.SH is a rare benign“tumor”, and fewer than 200 cases have been reported thus far.Moreover, hamartoma in PAS has not been reported.In the present study, we report the first case.SH can occur in any age group, usually asymptomatically with no sex predilection[9].Τhey are usually found incidentally during physical examination or at autopsy.Τhe tumors vary in size, ranging from a few millimeters to a maximum of 20 cm, with a median size of 5 cm.Women often encounter larger masses, suggesting a hormonal influence[4].
And he added that he was a prince enchanted8 by a powerful giant, but was only allowed to take his own shape at night, for all day he was forced to appear as the lion whom she had so often helped; and, more than this, it was the giant who had stolen the oxen and the asses and the pigs in revenge for her kindness
Xu SY collected case data and prepared the photos; Wei SM proofread the pathologic materials;Xu SY wrote the manuscript; Zhou B, Zhao YN and Yan S proofread and revised the manuscript; all authors approved the final version to be published.
He had to clean it everydayand that was rather hardfor it was such a dirty jobto mop and slop and scour2 and scrapeevery corner, nook and crannyin that reindeer place
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Τhe authors declare that they have no conflict of interest.
Τhe authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Considering the father s later appearance, it is possible to see this as a plot by the father and Thrushbeard to teach the daughter a lesson. It is also worth noting that this is a forced separation (rejection) of the daughter from her father and that the separation comes from the father himself.Return to place in story.
Τhis article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Then he took the scarf, which had a strange kind of scent21, and tied it round his left arm, thinking all the while that the best way to keep awake was not to go to bed at all
And yet my father was not a skin-dresser nor an executioner; on the contrary, his employment placed him at the head of the grandest people of the town, and it was his place by right
Shao-Yan Xu 0000-0001-8016-0917; Bo Zhou 0000-0002-4139-5462; Shu-Mei Wei 0000-0002-5362-8083;Ya-Nan Zhao 0000-0002-4938-9235; Sheng Yan 0000-0002-4153-3546.
Zhang H
A
Zhang H
1 Wadham BM, Adams PB, Johnson MA.Incidence and location of accessory spleens.
1981; 304: 1111[PMID: 7207579 DOI: 10.1056/nejm198104303041822]
2 Spencer LA, Spizarny DL, Williams TR.Imaging features of intrapancreatic accessory spleen.
2010; 83: 668-673 [PMID: 19690077 DOI: 10.1259/bjr/20308976]
3 Eker T, Kocaay AF, Sevim Y, ?akmak A.Splenic hamartoma is a rare cause of abdominal pain: Case report and literature review.
2017; 33: 294-295 [PMID: 29260137 DOI: 10.5152/UCD.2015.3048]
4 Cheng N, Chen J, Pan Y, Jiang Y, Zhou J, Shao C.Splenic hamartoma with bizarre stromal cells: a case report and literature review.
2018; 13: 8 [PMID: 29378604 DOI: 10.1186/s13000-018-0687-y]
5 Falk S, Stutte HJ.Hamartomas of the spleen: a study of 20 biopsy cases.
1989; 14: 603-612 [PMID:2759557 DOI: 10.1111/j.1365-2559.1989.tb02201.x]
6 Lee H, Maeda K.Hamartoma of the spleen.
2009; 133: 147-151 [PMID: 19123729 DOI:10.5858/133.1.147]
7 Gonzalez Urquijo M, Rodarte-Shade M, Rangel-Rangel R, Castillo-Meraz JA, Rodriguez-Tejeda JR, Gil-Galindo G.A giant splenic hamartoma associated with hematologic disorders: A case report.
2018; 36: 199-202[PMID: 30505440 DOI: 10.1016/j.amsu.2018.11.003]
8 Zhu HX, Lou WH, Kuang TT, Wang DS.Post-splenectomy intrapancreatic accessory spleen mimicking endocrine tumor of the pancreas.
2014; 5: 1151-1153 [PMID: 25437661 DOI: 10.1016/j.ijscr.2014.11.032]
9 Lam KY, Yip KH, Peh WC.Splenic vascular lesions: unusual features and a review of the literature.
1999;69: 422-425 [PMID: 10392884 DOI: 10.1046/j.1440-1622.1999.01550.x]
10 Sim J, Ahn HI, Han H, Jun YJ, Rehman A, Jang SM, Jang K, Paik SS.Splenic hamartoma: A case report and review of the literature.
2013; 1: 217-219 [PMID: 24340270 DOI: 10.12998/wjcc.v1.i7.217]
11 Zukerberg LR, Kaynor BL, Silverman ML, Harris NL.Splenic hamartoma and capillary hemangioma are distinct entities:immunohistochemical analysis of CD8 expression by endothelial cells.
1991; 22: 1258-1261 [PMID: 1748432 DOI: 10.1016/0046-8177(91)90108-2]
12 Yigit N, Covey S, Tam W.Massive splenic hamartoma with bizarre stromal cells.
2015; 101: 315-316[PMID: 25637257 DOI: 10.1007/s12185-015-1748-6]
13 Ramdall RB, Alasio TM, Cai G, Yang GC.Primary vascular neoplasms unique to the spleen: littoral cell angioma and splenic hamartoma diagnosis by fine-needle aspiration biopsy.
2007; 35: 137-142 [PMID: 17304535 DOI: 10.1002/dc.20568]
14 Conlon S, Royston D, Murphy P.Splenic hamartoma.
2007; 18: 200-202 [PMID: 17573768 DOI:10.1111/j.1365-2303.2006.00371.x]
15 Silverman ML, LiVolsi VA.Splenic hamartoma.
1978; 70: 224-229 [PMID: 696681 DOI:10.1093/ajcp/70.2.224]
16 Levy AD, Abbott RM, Abbondanzo SL.Littoral cell angioma of the spleen: CT features with clinicopathologic comparison.
2004; 230: 485-490 [PMID: 14752189 DOI: 10.1148/radiol.2302030196]
17 Darden JW, Teeslink R, Parrish A.Hamartoma of the spleen: a manfestation of tuberous sclerosis.
1975; 41: 564-566 [PMID: 1166974]
18 Abbott RM, Levy AD, Aguilera NS, Gorospe L, Thompson WM.From the archives of the AFIP: primary vascular neoplasms of the spleen: radiologic-pathologic correlation.
2004; 24: 1137-1163 [PMID: 15256634 DOI:10.1148/rg.244045006]
19 Wang JH, Ma XL, Ren FY, Zuo CJ, Tian JM, Wang ZF, Zheng JM.Multi-modality imaging findings of splenic hamartoma: a report of nine cases and review of the literature.
2013; 38: 154-162 [PMID: 22539044 DOI:10.1007/s00261-012-9880-8]
20 Havlik RJ, Touloukian RJ, Markowitz RI, Buckley P.Partial splenectomy for symptomatic splenic hamartoma.
1990; 25: 1273-1275 [PMID: 2286905 DOI: 10.1016/0022-3468(90)90529-i]
21 Carleton C, Hoang L, Sah S, Kiyokawa T, Karamurzin YS, Talia KL, Park KJ, McCluggage WG.A Detailed Immunohistochemical Analysis of a Large Series of Cervical and Vaginal Gastric-type Adenocarcinomas.
2016; 40: 636-644 [PMID: 26685087 DOI: 10.1097/PAS.0000000000000578]
22 Fujii T, Obara T, Shudo R, Tanno S, Maguchi H, Saitoh Y, Ura H, Kohgo Y.Splenic hamartoma associated with thrombocytopenia.
1997; 32: 114-118 [PMID: 9058306 DOI: 10.1007/BF01213307]
 World Journal of Gastrointestinal Oncology2022年5期
World Journal of Gastrointestinal Oncology2022年5期
- World Journal of Gastrointestinal Oncology的其它文章
- Correction to “Efficacy and safety of endoscopic resection in treatment of small gastric stromal tumors: A state-of-the-art review”
- Primary hepatic angiosarcoma manifesting as hepatic sinusoidal obstruction syndrome: A case report
- Digital single-operator cholangioscopy for biliary stricture after cadaveric liver transplantation
- Preoperative prediction of malignant potential of 2-5 cm gastric gastrointestinal stromal tumors by computerized tomography-based radiomics
- Pretreatment serum albumin-to-alkaline phosphatase ratio is an independent prognosticator of survival in patients with metastatic gastric cancer
- Scoping out the future: The application of artificial intelligence to gastrointestinal endoscopy