
Hyper-accuracy three-dimensional reconstruction as a tool for better planning of retroperitoneal liposarcoma resection: A case report
2022-02-11 05:29:14MuShiYeHaoKaiWuXingZhangQinFanLuoZhuoLi
World Journal of Clinical Cases 2022年1期
INTRODUCTION
Retroperitoneal pathologic processes might be asymptomatic and often present as large masses at initial imaging evaluation[1]. Retroperitoneal sarcomas accounts for 9% to 15% of all adult soft-tissue sarcomas[2], including liposarcoma, leiomyosarcoma, and malignant fibrous histiocytoma/undifferentiated pleomorphic sarcoma[3]. Retroperitoneal liposarcoma is the second most common, accounting for 45%[4]. Hyper-accuracy three-dimensional (3D) reconstruction is based on contrast-enhanced computed tomography (CT), including arterial and delayed phases. It provides surgeons with three key anatomic aspects, including 3D surface-rendered and semitransparent organs and tumors, and the 3D course of extra- and intrarenal arteries[5]. It is now widely used in robotic partly nephrectomy owing to its ability to visualize overlapping anatomy[6,7].
CASE PRESENTATION
Chief complaints
A 54-year-old man was admitted to our department for progressive abdominal distension over the preceding 2 mo.
History of present illness
The patient started to feel abdominal distension and noted his abdomen’s volume increasing 2 mo before presentation. He denied diarrhea, vomiting, abdominal pain, or constipation. He also denied any changes in bowel habits. He lost approximately 5 kg in the previous 2 mo.
Long after them came Esben riding on his stick, and he also wanted to get a place in the palace, but no one had any use for him, and he was told that he could just go back the way he had come
History of past illness
The patient was previously healthy.
Abdominal CT angiography revealed a 32 cm × 21 cm × 12 cm lipoma-like mass extending from the sub-hepatic space to the pelvic cavity. There were no enlarged lymph nodes. Radiocontrast agent confirmed the displacement of the right kidney to the left lower quadrant (Figure 1). Because of the complex relationship between the mass and nearby tissue, we performed a hyper-accuracy three-dimensional reconstruction (Figure 2). This study revealed that the mass received blood vessels from a branch of the right renal artery. The celiac trunk, the superior mesenteric, the inferior vena cava, and the pancreas were displaced and compressed.
Personal and family history
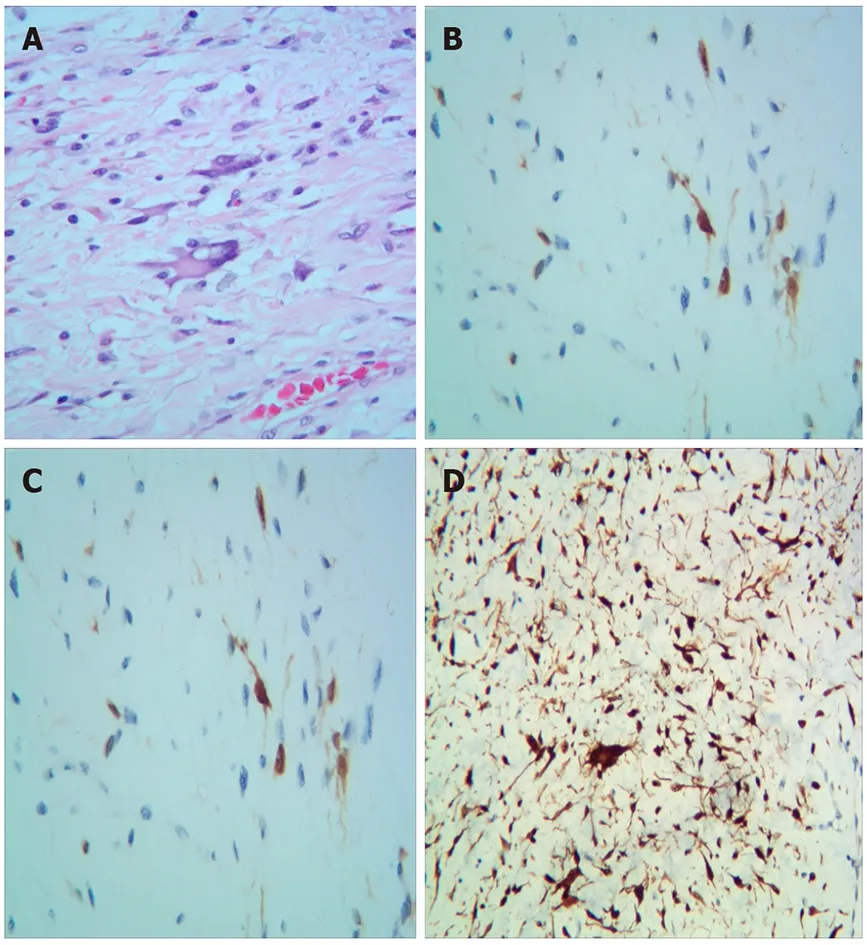
Pathological examination revealed well-differentiated liposarcoma (WDLPS). Macroscopically, the mass appeared oval but was separated into irregular lobulations. Its size was 37 cm × 26 cm × 10 cm and it weighed approximately 11 kg. The surface of the mass was covered with a smooth and grayish capsule. The mass wrapped the adrenal gland. Microscopically, the tumor was composed of well-differentiated adipocytes and spindle-shaped cells. Areas of necrosis were rare. Nuclear degeneration was found in some areas (1/10 high-powered fields). Immunohistochemically, the tumor was partly positive for MDM2, S100, CK34, and CKD4, with a low grade of dedifferentiation (Ki-67: 20%) (Figure 3).
Laboratory tests showed a normal white count and hemoglobin level of 103.0 g/L (reference range, 120-160 g/L for man). His 8 AM cortisol level was 2.06 μg/dL (reference range, 8.7-22.4 μg /dL) and adrenocorticotrophic hormone level was 6.14 pg/mL (reference range, 0-46 pg/mL). The albumin level decreased slightly (30.9 g/L; reference range, 35.0-54.0 g/L), with no other liver function and kidney function abnormalities.
WDLPS.
Physical examination
The patient was afebrile with stable vital signs. He was 163 cm in height and 56 kg in weight. Abdominal physical examination revealed a fixed abdominal mass with illdefined margins occupying the entire abdomen. No other abnormal signs were found.
Laboratory examinations
We planned to leave immediately after lunch. I noticed Daniel, who will be ten in November, and Wes, who will be seven in December, scramble1 for() their gear. They had spent the morning pouring over outdoor outfitter catalogs looking at sophisticated equipment that would be sufficient to thru-hike the Appalachian Trail.
Imaging examinations
Give this some thought. Remember both Karen and I love you and want our family ties to be restored. Remember that in your absence, we established strong family ties with Gordon, and it would be unfair to all of us to expect that to stop.

Histological examination
The patient had smoked for approximately 30 years, and his family history was unremarkable.

FINAL DIAGNOSIS
I held out the chain. She took it in both her hands, reached forward, and secured the simple clasp at the back of my neck. She stepped back then as if to see that all was well. I looked down at the shiny piece of glass and the tarnished13 golden chain, then back at the giver. I meant it when I whispered, Oh, Maria, it is so beautiful. She would have loved it. Neither of us could stop the tears. She stumbled into my arms and we wept together. And for that brief moment I became her mother, for she had given me the greatest gift of all: herself.
TREATMENT
Explorative laparotomy was performed. We chose a median abdominal incision from the xiphoid process to the pubic symphysis. No signs of infiltration or metastasis were found in the abdominal cavity. Because we ensured that the tumor was localized in the retroperitoneum, we opened the retroperitoneum in the paracolic recess. After liberating the ascending colon and partial transverse colon and fully exposing the tumor, we began to liberate the tumor from the right iliac vessel. Finally, we released the tumor from the right kidney, inferior vena cava, and abdominal aorta. The operation took 6 h and the volume of blood loss was 100 mL approximately.
OUTCOME AND FOLLOW-UP
The hemoglobin level was 91.0 g/L (reference range, 120-160 g/L in men) on the 1postoperative day. The postoperative course was uneventful, and the patient was discharged on the 6postoperative day. At the final follow-up (about 16 mo after surgery), he was in good general condition, and a CT scan revealed no signs of tumor recurrence (Figure 4).

DISCUSSION
WDLPS is the second most common liposarcoma arising in the retroperitoneum[8]. WDLPS in the retroperitoneum carries higher risks of relapse[9-11]. Surgical resection is the standard of cure[11,12]. Macroscopic complete resection is essential to curative treatment[13]. Compared to complete resection, aggressive surgical policies reduce the local recurrence rate of primary retroperitoneal sarcomas, but it has not improved overall survival[14,15]. As for its asymptomatic nature in the early stage, WDLPS in the retroperitoneum is often diagnosed with a massive size[16]. Resection in such situations may involve multiple organs and vasculature, making it difficult to achieve clear resection margins[17]. It also carries a high risk of massive hemorrhage and hemodynamic instability. Contrast-enhanced CT is the most useful and widely available primary imaging technique[18]. The appearance of WDLPS on CT is a bland fat density mass[18]. CT provides size, consistency, and relations between the tumor and the adjacent tissue[19]. Hyper-accuracy three-dimensional reconstruction is a tool that provides more full-scale information of organs than does traditional CT. Threedimensional reconstruction is also more helpful for diagnosis and operative planning[20]. It provides the surgeon with more detail regarding anatomical structures and more macroscopic images to select better surgery approaches and determine resection ranges. In our case, hyper-accuracy three-dimensional reconstruction of the abdomen revealed the intimate relationships between the adjacent organs and crucial vascular structures. This modality revealed that the right renal artery’s feeding artery had three branches, from the upper to the lower pole of the tumor. We also noted that the inferior vena cava and the right kidney adhered extensively with the tumor but had defined borders. The right kidney was displaced to the left lower quadrant and was partly involved by the tumor. The anatomical position of the left kidney was not affected. Because its density was similar to that of the tumor, we could not observe the right adrenal gland. We speculated that the tumor had already invaded the adrenal gland. According to the three-dimensional images, we identified and ligated the feeding artery precisely; this allowed us to minimize bleeding during the separation of the tumor and shortened the operative time substantially. Just as we observed preoperatively, the adventitia of the inferior vena cava and capsule of the right kidney were completely enclosed. Finally, we released the tumor from the adhesions to organs including the inferior vena cava, abdominal aorta, pancreas, and right kidney, with subsequent removalwith the adrenal gland, which we confirmed on postoperative pathology.
CONCLUSION
Surgical resection of WDLPS is critical because of the high risk of recurrence. Retroperitoneal masses can complicate anatomical relationships, especially with blood vessels. Hyper-accuracy three-dimensional reconstruction of the abdomen or tumor is useful for operative planning owing to its intuitiveness and precise information regarding anatomical structures in both the tumor and nearby tissues. We recommend hyper-accuracy three-dimensional reconstruction when the tumor is large, and its anatomical relationships with nearby tissue are complex.
 World Journal of Clinical Cases2022年1期
World Journal of Clinical Cases2022年1期
- World Journal of Clinical Cases的其它文章
- Omicron variant (B.1.1.529) of SARS-CoV-2: Mutation, infectivity,transmission, and vaccine resistance
- Clinical manifestations and prenatal diagnosis of Ullrich congenital muscular dystrophy: A case report
- Lunate dislocation with avulsed triquetral fracture: A case report
- Protein-losing enteropathy caused by a jejunal ulcer after an internal hernia in Petersen's space: A case report
- Eustachian tube teratoma: A case report
- Cerebral venous sinus thrombosis in pregnancy: A case report