
Biomarkers for response to immune checkpoint inhibitors in gastrointestinal cancers
2022-01-25 02:55:14MengLiDenisKailiLeiShi
INTRODUCTION
Gastrointestinal (GI) cancers are common among all cancer types,and the incidence and mortality rates of GI cancers are increasing year by year,especially in colorectal cancer (CRC),which is also accompanied by a tendency of rejuvenation[1].GI cancers mainly occur in the GI system and related digestive organs,including the esophagus,stomach,biliary tract system,liver,pancreas,small intestine,rectum,and anus.Among them,hepatocellular carcinoma (HCC) has the highest morbidity and mortality rate.For example,from 2000 to 2016,the mortality rate for HCC increased by 43% (from 7.2 to 10.3
100000),with a 5-year survival rate of only 18% in the United States[2].Treatment strategies for GI cancers include surgery,chemotherapy,radiotherapy,targeted therapy,and immunotherapy,among which immunotherapy is a hot topic in recent years.
Immunotherapy is a relatively new therapeutic strategy that has received widespread attention,mainly including immune checkpoint inhibitors (ICIs),tumor vaccines,and immune cell therapy.Among these,ICIs are most widely used[3].Immune checkpoints are used by normal cells to regulate immune cytotoxic functions,thus avoiding the destruction of normal tissues.However,this mechanism can also be borrowed by tumor cells to escape the body's immune surveillance and clearance[4].ICIs can eliminate this inhibitory effect,allowing immune cells to be reactivated to a working state and destroy tumor cells.
The better studied ICIs are CTLA-4 inhibitors and programmed cell death protein 1/programmed cell death ligand 1 (PD-1/PD-L1) inhibitors.Ipilimumab (anti-CTLA-4) was approved by the FDA in 2011 for the treatment of melanoma,followed by the PD-1 inhibitors pembrolizumab and nivolumab for the treatment of melanoma,metastatic non-small cell lung cancer (NSCLC),and DNA mismatch repair-deficient/microsatellite instability-high (dMMR/MIS-H) tumors[5,6].Although there are many immune checkpoints,not limited to those mentioned above,they have a relatively similar mechanism of action.For example,PD-1 is able to bind to PD-L1 in tumor cells,disabling the ability of T cells to attack cancer cells.Their binding acts as a co-inhibitory signal for T cells and negatively regulates the body's immune response.In turn,tumor cells can upregulate the expression of PD-L1 to inhibit the activation of T cells.This suppression can be abolished after ICI treatment,and in turn,T cells are able to perform their normal functions[7].In this regard,immunotherapy is now becoming a prospective treatment for GI cancers.
39.Puss became a great lord: Basile s version of this tale, Cagliuso (also known as Gagliuso), makes a social commentary about court life and ends much differently than Perrault s. Cagliuso betrays his cat after she pretends to die, and throws her out a window rather than placing her in a golden coffin, as he had promised. Basile s tale parodies the social dynamics usually at the heart of the fairy tale,...exemplified just as much by the lack of gratitude toward the helper cat...as by the ridiculous figure of Cagliuso, to whose new noble title corresponds no such noble spirit. The extratextual comments on Cagliuso...stress the prevalence of ingratitude in society at large, and, in particular in the world of the courts. (Canepa 1999, 146). KHReturn to place in story.
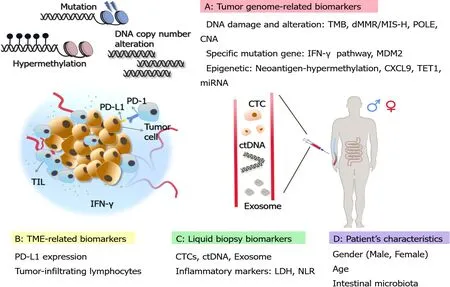
Although immunotherapy has provided sustained clinical benefits,studies have found limitations in the effectiveness of immunotherapy and it is extremely important to study biomarkers to predict more accurate clinical responses[8].Biomarkers for predicting ICI response have been extensively explored and developed.A variety of biomarkers for GI malignancies have been clinically applied,which can help patients to choose the appropriate targeted therapeutic options.This review highlights biomarkers for predicting the response to ICIs for the treatment of GI tumors.Some biomarkers applied to other tumors are also presented,intending to provide further reference and validation for GI tumors (Figure 1).In addition,we present some new approaches that have emerged in recent years,such as single-cell analysis and machine learning.
TUMOR GENOME BIOMARKERS
Tumor mutation burden
The tumor mutation burden (TMB) represents the density of distribution of nonsynonymous mutations in the protein-coding region,or simply the number of mutations present in the tumor (Table 1).It is usually defined as the total number of mutations
megabase of substitutions and insertions or deletions in the exon coding region of the gene evaluated in the tumor sample and is usually detected as mutations
million bases (Mut/Mb)[9].Traditionally,whole-exome sequencing (WES) has been used to measure TMB,which is considered the standard for TMB determination.However,due to the high cost and relatively slow speed of detection using WES,the accurate determination of TMB by next-generation sequencing (NGS) panels has recently been applied[10].Quantifying the number of non-synonymous single nucleotide variants (SNVs) by NGS,followed by algorithmic validation and extension to WES,is also one of the feasible approaches in recent years[11].
The non-invasive nature of liquid biopsy reduces patient suffering compared to sampling of surgery,while adding advantages that tissue biopsy does not offer.Liquid biopsy overcomes the inevitable heterogeneity of tissue biopsy,allowing for multiple sampling and providing real-time data on tumor changes and relatively more comprehensive results[70].Circulating tumor DNA (ctDNA),circulating tumor cells (CTCs),and exosomes are commonly promising biomarkers for liquid biopsy.
After school, the girls invited me to join them in front of the school. I was thrilled to be a member of the club, however tentative. We waited. For what, I didn’t yet know. Oh, how I wish I had gone home, but I had a lesson to learn.
After all, six hundred years is an eternity14! Ah, dear king, replied the young man, your offer is very tempting15! But at the end of six hundred years we should have to die, so we should be no better off! No, I must go on till I find the country where there is no death at all
In another retrospective study,TMB levels of patients with various types of melanoma as well as NSCLC were also classified as low (1-5 Mut/Mb),medium (6-19 Mut/Mb),and high (≥ 20 Mut/Mb).Their analysis indicated that patients with high levels of TMB had the highest response rate to ICI treatment,reaching 58%,and also had the longest duration of progression-free survival (PFS) at 12.8 mo.The other two treatment groups had a response rate of only 20% and a PFS of only 3.3 mo[15].Another study detected TMB (cut-off value of 20 Mut/Mb) in 4064 NSCLC patients and found that patients with high levels of TMB (TMB-H) had a significantly higher overall survival (OS) and disease control rate (DCR) when treated with anti-PD-1/L1 agents compared to patients with low levels of TMB (TMB-L)[16].Similar results were presented in another study showing significantly better durable clinical benefit (DCB)and PFS in the TMB-H population in a cohort with 78 NSCLC patients treated with anti-PD-1/L1 antibodies[17].Additionally,in a prospective analysis of KEYNOTE-158,Marabelle
[18] assessed the association of pembrolizumab monotherapy in terms of TMB (tTMB) and clinical outcome across ten different advanced solid tumors types,including anal,biliary,
The results revealed that in terms of efficacy,the ORR (29%
6%) was better in the tTMB-high group (defined as ≥ 10 Mut/Mb) than in the tTMBlow group (<10 Mut/Mb),and the median durable response (follow-up of approximately 3 years) was not reached,while the tTMB-low group only reached 33.1 mo[18].
ctDNA is mainly released by dead cancer cells,or can also be secreted directly by CTCs,reflecting information about the entire tumor genome,and the variability of its data provides the feasibility of dynamic monitoring of tumor progression throughout the treatment regimen[71].Several studies have shown that high ctDNA mutations are associated with a poor OS and prognosis in patients with different cancer types treated with ICIs[24].Lee
[72] showed that melanoma patients with persistently elevated ctDNA during anti-PD-1 therapy exhibited less favorable responses with a shorter PFS and OS[72].Also for GI cancers,among 25 patients with stages I-III CRC,the 2-year RFS was 66% in ctDNA-positive patients compared with 100% in negative patients.In addition,ctDNA showed a negative tendency of recurrence rates,in agreement with the previous result[73].In a study of 46 advanced GC patients treated with anti-PD-1,the mutational status of baseline ctDNA affected the PFS of patients with a median of 7.4 mo (undetectable ctDNA)
4.9 mo (detectable ctDNA)[74].This suggests that ctDNA may serve as a potential negative biomarker for response to ICI therapy in patients with advanced GC.Recent reports have also linked the detection of CTCs to tumor metastasis.The results showed that PD-L1 was overexpressed in CTCs of patients with advanced head and neck cancers,revealing that combined detection of PD-L1 and CTC may have potential as a biomarker for ICI efficacy prediction[75].
The name Falada has become well associated with this tale, however, and almost as easily identifies the story as the Goose Girl herself.Return to place in story.
Several studies presented at the 2020 American Society of Clinical Oncology meeting confirmed the predictive value of TMB in immunotherapy or combination therapy,although TMB still has limitations as a biomarker.In addition,several general issues deserve further attention,both in the application of GI cancers and in a wide range of other tumor types.First,there is no clear TMB cut-off value as a criterion to accurately determine which patients can benefit from ICI treatment[22].Second,testing at the proteomic level may provide a clear picture of the mutational load on the membrane of tumor cells,as some mutations that cause an immune response may originate from only a small subset of genes[23].Third,factors such as allele frequency might be considered for further and more accurate prediction of ICI efficacy[24].
dMMR/MSI-H
MSI refers to microsatellite instability and MMR refers to mismatch repair function.They are closely related,
,when the MMR functions are in a proficient state(pMMR),MSI can be repaired to maintain stability (MSS).In contrast,when the expression of any of the MMR-related proteins goes wrong and the MMR function is in a deficient state (dMMR),it leads to defects in cellular repair functions,allowing DNA to accumulate mutations during replication,ultimately leading to the development of MSI[25].MSI can be broadly classified as highly unstable (MSI-H),lowly unstable (MSI-L),and stable (MSS).The dMMR and MSI-H can be roughly equated,as can pMMR and MSS[26].
33.Mice:Walt Disney gave the mice personalities86 and made them important characters in his well-known film of the story. In the older versions, the mice only exist for their necessary transformation87 into part of Cinderella s grand transportation to the ball.Return to place in story.
The dMMR occurs in a variety of tumor types,especially common in GI cancers,including colorectum,stomach,small intestine,prostate,
[27].It has been shown that dMMR/MSI-H tumors have a much higher somatic mutation rate compared to pMMR tumors and are thought to express a large number of shift-code peptides that act as neoantigens and enhance the immune response[28].In 2017,the United States FDA first approved the PD-1 inhibitor pembrolizumab for the treatment of patients with solid dMMR/MSI-H tumors[29].Several clinical trials,including KEYNOTE-012,016,028,and 158,which included multiple tumor types,have shown that pembrolizumab has promising durable outcomes in treating patients with dMMR/MSI-H tumors[24].
In the treatment of GI cancers,especially in CRC,dMMR/MSI-H is considered to be a relatively well-established group of biomarkers.In the KEYNOTE-164 clinical trial study,the efficacy of pembrolizumab was evaluated in three cohorts of 11 dMMRCRC,21 pMMR-CRC,and 9 dMMR non-CRC patients.An immune-related ORR of 40% and a 20-wk PFS of 78% were observed in the dMMR-CRC cohort,while an ORR of 0 and a 20-wk PFS of 11% were observed in the pMMR-CRC cohort.Median PFS and OS were not achieved in the dMMR-CRC cohort,but were 2.2 mo and 5.0 mo,respectively,in the pMMR-CRC cohort.These results demonstrated that dMMR patients are favorable candidates for treatment with ICIs[30].Lu
[31] investigated the clinical benefit of ICIs in GI patients.They indicated that the incidence of DCB was significantly higher in dMMR/MSI-H patients (59.1%) than in MSI-L/MSS/pMMR patients (28.6%).In addition,the median PFS time was significantly longer in dMMR/MSI-H patients (7.24 mo) than in MSI-L/MSS/pMMR patients (2.67 mo)[31].These data reveal that dMMR/MSI-H patients have a more favorable ICI response than the other groups.The dMMR/MSI-H has reliable clinical data as a wellestablished biomarker in GI cancers,especially in CRC.Its application in other GI cancers also deserves attention and further exploration.
Copy number alteration
Recently,it has also been shown that copy number alterations (CNA),including copy number gain (CNgain) and copy number loss (CNloss),have a predictive role in ICI therapy.In melanoma patients treated with ICIs,CNLoss was found to be lower in responders[32].Some ICI-related immune features were also found to be negatively correlated with CNA in GC and CRC of the Cancer Genome Atlas (TCGA) datasets[33].Detailed data are presented for elaboration in the study by Lu
[31].In their study,tumor samples from 93 patients with GI cancers treated with ICIs were tested.CNA load included measures of total CNA,CNgain,and CNloss,while CNgain/CNloss was defined as the total number of genes with CNgain/CNloss present in each sample[31].They found a significant difference in the CNA burden index between DCB and NDB (no durable benefit) patients treated in the GI group,with DCB patients having a significantly lower CNA burden than NDB patients,suggesting that a low CNA burden may be correlated with better ICIs outcomes.DCB rates were more pronounced in the low and high groups with the same low level of CNgain/CNloss.Further exploration of OS and PFS also led to more favorable data in the low burden group.Based on the study,the group with lower CNA showed a longer median OS(not achieved in all cohorts).For PFS,it was also suggested that the lower CNA group had a longer PFS,all at more than 10 mo[31].Furthermore,a study by Smeet
[34]on CRC treated with bevacizumab combination therapy also illustrated another perspective on the possibility of CNA as a potential biomarker for ICI treatment.Their study,which also defined three CNA groups,showed that tumors in the low-load CNA group did not benefit from this combination therapy,while in turn confirmed that ICI therapy is the superior choice.Likewise,the potential of low-load CNA as a predictive biomarker for ICIs was also confirmed[34].
As a noteworthy point,considering the combination of TMB and CNA,a significantly higher proportion of patients with DCB were in the TMB-High/CNA-Low subgroup (12/14) compared to the TMB-Low/CNA-High subgroup (1/28).The median OS (not achieved) was also significantly longer in the TMB-high/CNA-low subgroup than in the other three subgroups (TMB-Low/CNA-Low,17.3 mo;TMBHigh/CNA-High,12.37 mo;TMB-Low/CNA-High,6.23 mo)[31].This result suggests that the combined use of these two biomarkers may have a higher accuracy.
IFN-γ signal and MDM2
Alterations within the tumor-associated signaling pathways also affect the efficacy of ICIs,related to the mechanism of checkpoint inhibitor drugs as well as drug resistance[35].IFN-γ is a cytokine that stimulates the immune response and is one of the key signals for the activation of immune cells.IFN-γ is also able to trigger a series of events leading to tumor cell death by linking to receptors on the cell surface.Moreover,IFN-γ is able to increase the expression of PD-L1 in tumors and increase the expression of MHC,promoting antigen presentation in antigen presenting cells[36].
Grasso
[37] showed that IFN-γ released by T cells contributes to the amplification of nascent anti-tumor immune response[37].A study by Karachaliou
[38],which included seven NSCLC patients treated with pembrolizumab,showed that high expression of IFN-γ may be associated with a better PFS and OS in NSCLC patients[38].Higgs
[39] similarly showed that patients with elevated IFN-γassociated signaling had a longer median OS (18.1-22.7 mo
6.5-7.7 mo) and better ORR (6-fold higher) in advanced NSCLC[39].The above results revealed a trend towards the application of IFN-γ in GI cancers.
KEYNOTE-028 is a phase Ib trial of pembrolizumab in patients with 20 different tumor types,including GI cancers.In the esophageal cohort,23 patients were enrolled and an IFN-γ signature was detected,showing a trend towards predicting response to ICIs[40].In GC,Epstein-Barr virus (EBV) is involved in approximately 10% of GC progression,and PD-L1 overexpression is presented as a feature of EBV GC.In addition,IFN-γ signaling was also shown to be involved in a study by Sasaki
[41].Similarly,in the KEYNOTE-012 clinical trial,which included GC patients treated with pembrolizumab,IFN-γ-related genes were shown to be correlated with OS and PFS[42].Overall,these results provide useful information revealing the role of IFN-γ in predicting the efficacy of ICIs in GI cancers.
Mutations in genes related to the IFN-γ pathway,such as
,
and
,also lead to poor outcomes and resistance in patients receiving ICI therapy[35,43].The JAKs are key kinases in this pathway,and JAK1/2 shift mutations lead to deficient production of IFN-γ.Shin
[44] indicated that JAK1/2 mutations were associated with resistance to anti-PD-1 therapy in CRC patients[44].These results suggest that mutations in JAK can lead to poor efficacy of ICIs[44,45].
MDM2 is known as the mouse double minute 2 homolog and is an E3 ubiquitin ligase.When MDM2 is overexpressed due to amplification or improper regulation,it inhibits the activation of P53,which in turn accelerates tumor growth and progression[46].Kato
[47] analyzed the genomic profiles of 155 patients with multiple tumor types and found that six patients with MDM2 amplification have a time to treatment failure (TTF) less than 2 mo.Four of the six cases (all with MDM2 amplification)showed 2.3 to 42.3-fold hyperprogression compared to ICI pre-treatment[47].A recent study also showed that cell lines with high MDM2 expression were more potent against T cell-mediated tumor killing,and that targeting MDM2 improve the efficacy of ICIs[48].These imply that there may be a negative correlation between amplified variants of MDM2 and the efficacy of ICIs,allowing tumors to develop hyperprogression after receiving treatment.
Second, the heroine is accomplishing a difficult task, removing a settled stain from clothing. Psyche, in Cupid and Psyche, has to perform three impossible tasks to prove her devotion to Cupid.
Dysfunction of the MDM2-P53 axis is a major contributor to GI cancers.The main risk factors for HCC include chronic viral infections and metabolic diseases,all of which may contribute to HCC through dysfunction of the MDM2-P53 axis[49].The results by Wu
[50] on prognostic markers for HCC showed that MDM2 was able to directly act on BIRC5 as well as the downstream transcription factors to regulate its expression,thereby reducing the sensitivity and effectiveness of ICI therapy[50].Based on the association from the available clinical data,MDM2 is expected to be a more specific negative biomarker for predicting ICIs in HCC,although further prospective studies are needed to corroborate this.
Since it has ended in my meeting you, said the Princess, I cannot regret the step I have taken, and if you will let me stay with you, I shall be perfectly happy
TUMOR IMMUNE MICROENVIRONMENT-RELATED BIOMARKERS
PD-L1 expression
Tumor-infiltrating lymphocytes (TILs) represent an effective mechanism of adaptive immunity with anti-tumor potential and have been shown to be associated with prognosis and response to immunotherapy in various types of cancer[61].TILs originate from areas of tumor tissue,have specific recognition of autologous tumors,and have specific MHC-restricted tumor lysis activity[62].Among the different types of tumor immune infiltration,the relationship between immune inflammation and ICI treatment is more evident.
Nevertheless,PD-L1 expression remains limited and somewhat controversial as a comprehensive,stand-alone biomarker.In the trials mentioned above,both Keynote-059 and Attraction-02 did show higher response activity in PD-L1-positive patients,but the data equally showed response activity in PD-L1-negative patients[55].Concerning the limitations of PD-L1 expression,the following points are noteworthy.First,in the tumor microenvironment,PD-L1 expression displays dynamics and diversity with spatial and temporal heterogeneity[56].PD-L1 expression detected at a single time point cannot be fully used to assess ICI response[57].Second,PD-L1 detection criteria are not standardized,with no exact positive scores and thresholds to define[56,58].Issues such as inconsistent antibody usage and inconsistent detection thresholds make it difficult to standardize staining systems as well[59].At the molecular level,PD-L1 expression has two components:Tumor cell-associated gene variants and PD-L1 expression induced by IFN-γ secreted by infiltrating T cells.The former has constitutive expression,which is not significantly related to the efficacy of ICIs,while the latter is inducible expression,which is concentrated in the region near the T cells of tumor tissues,and is closely related to the efficacy of ICIs.However,these two types of PD-L1 are not strictly differentiated,which can easily lead to the incorrect conclusion that patients with high PD-L1 expression cannot benefit[60].Third,the detection methods for PD-L1 expression are not sensitive and precise enough.In an analysis of relevant studies,the response rate to ICIs ranged from 36%to 100% for PD-L1 expression-positive tumors,whereas for PD-L1 expression-negative tumors,the response rate ranged from 0% to 17%[52].
Tumor-infiltrating lymphocytes
PD-L1 is one of the most studied biomarkers with abundant data in clinical studies[51].The expression of PD-L1 in tumors measured by immunohistochemistry was one of the first biomarkers developed to predict the benefit of ICIs[52].In GI cancers such as GC,CRC,and HCC,there is a positive correlation between PD-L1 expression and the efficacy of ICIs[53,54].Many clinical trials have provided data demonstrating the feasibility of PD-L1 (Keynote-059,Keynote-010,Attraction-02,Checkmate-057,Checkmate-012,
),and the FDA has approved the application of PD-L1 expression as a biomarker for adjuvant or second-line treatment.
Immunoinflammation is characterized by the presence of CD8
and CD4
T lymphocytes in the tumor parenchyma and is accompanied by the expression of immune checkpoint molecules,revealing that ICI treatment may generate a tumor immune response[63].Analysis of pre-treatment samples showed a relative abundance of CD8
T cells at the infiltrative margins of responders,and serial sampling during treatment showed increased infiltration of CD8
T cells into the tumor parenchyma[64].Other data showed that patients with high CD8
TIL density achieve a longer PFS and OS compared to those with low density[65].Similarly,in a retrospective study of a series of patients including some with GI cancers,TILs in tumor biopsy samples were shown to be associated with improved survival[66].In a study by Xiao
[67] on CRC liver metastases,patients with high CD8
TIL had a significantly longer recurrence-free survival (RFS) than those with low CD8+TIL (median RFS:Unmet
55.8 mo,3-year RFS 71.6%
55.3%)[67].And the prognostic value of TILs was demonstrated by the higher accuracy of combining with PD-L1 expression.In addition,in esophageal cancer,a cohort with PD-L1 expression combined with high CD8
TILs showed a longer OS[68].In a peripheral blood analysis of a CRC patient treated with pembrolizumab who had a rapid response,high CD39 expression in CD8
TILs was also found,suggesting that CD39
CD8
TILs may be a promising predictive biomarker in GI cancers[69].
Then, for the rest of the wedding feast they gave him bread made with salt, and dishes with seasoning, and he said they were the very best he had ever eaten
LIQUID BIOPSY BIOMARKERS
Circulating tumor DNA,circulating tumor cells,and exosomes
According to several reports in recent years,increased TMB is associated with the response to ICI therapy,and high TMB was significantly associated with the efficacy of ICIs[12].There are many data supporting the use of increased TMB as a biomarker for ICI therapy in many pan-cancer treatments.According to a retrospective study that included 27 cancer types,patients with higher TMB were found to have better clinical outcomes and objective response rates (ORR) when treated with PD-1 antibody[13].In a phase II study of pembrolizumab in Korea,high TMB was defined as more than 400 SNVs in the WES.The results showed that elevated levels of TMB were associated with a high ORR (89%);the moderate TMB group (100-400 SNVs) had an ORR of 20%,while the low TMB group had an ORR of only 7%,indicating a similar positive correlation between high levels of TMB and ICI efficacy,
,higher values of TMB represent a higher overall response rate for patients[14].
Data from the above-mentioned studies have demonstrated the significant role of high levels of TMB in predicting ICI efficacy,and the results of TMB in GI cancers are no exception to other tumor types.In a phase I study with the anti-PD-1 antibody toripalimib,patients with metastatic gastric cancer (GC) with high TMB (>20 Mut/Mb) had a better response in survival compared to those with low TMB (15 mo
4 mo)[19,20].In patients with advanced GC,patients with high TMB (≥ 12 Mut/Mb)had significantly better efficiency (33.3%
7.1%) and OS time (14.6
4.0 mo) than patients with low TMB (<12 Mut/Mb)[20].In a study of metastatic CRC,none of the TMB-H group had achieved PFS (median follow-up>18 mo),while the TMB-L group had a PFS of only 2 mo and approximately 66% of TMB-L patients developed further disease[21].In conclusion,high levels of TMB in ICI therapy represent improved patient treatment efficiency and better prognostic outcomes.
Exosomes are extracellular vesicles carrying tumor-associated proteins,metabolites,RNA,DNA,and lipids,which cover most of the information needed for biopsy and can serve as important biomarkers[76,77].Zhang
[78] found elevated levels of exosomes in GC patients with liver metastases.Serum exosome levels were higher in GC patients than in healthy subjects,and the number of exosomes in serum was positively correlated with the stage of GC[78].It has been further revealed that the mRNA expression of
in plasma exosomes correlates with the efficacy of ICIs,which may lead to the suppression of effector lymphocytes involved in antitumor immunity,making ICIs less effective[79].Still in GC,according to Fan
[80],OS was significantly lower in the high exosomal PD-L1 group than in the low group.In their subgroup analysis,this difference was found to be even more pronounced in early GC,suggesting that high exosomal PD-L1 could be used as a predictor of the early stage of GC[80].The combination of exosome and PD-L1 assays has informative implications in GI cancers;however,it remains to be noted that exosomes still face challenges as biomarkers,and need to be further explored to accurately measure their quantity and purity.
OTHER BIOMARKERS OF WORTH IN GI CANCERS
Trusty John lifted him up, carried him to bed, and thought sorrowfully: The curse has come upon us; gracious heaven! what will be the end of it all? Then he poured wine down his throat till he came to himself again
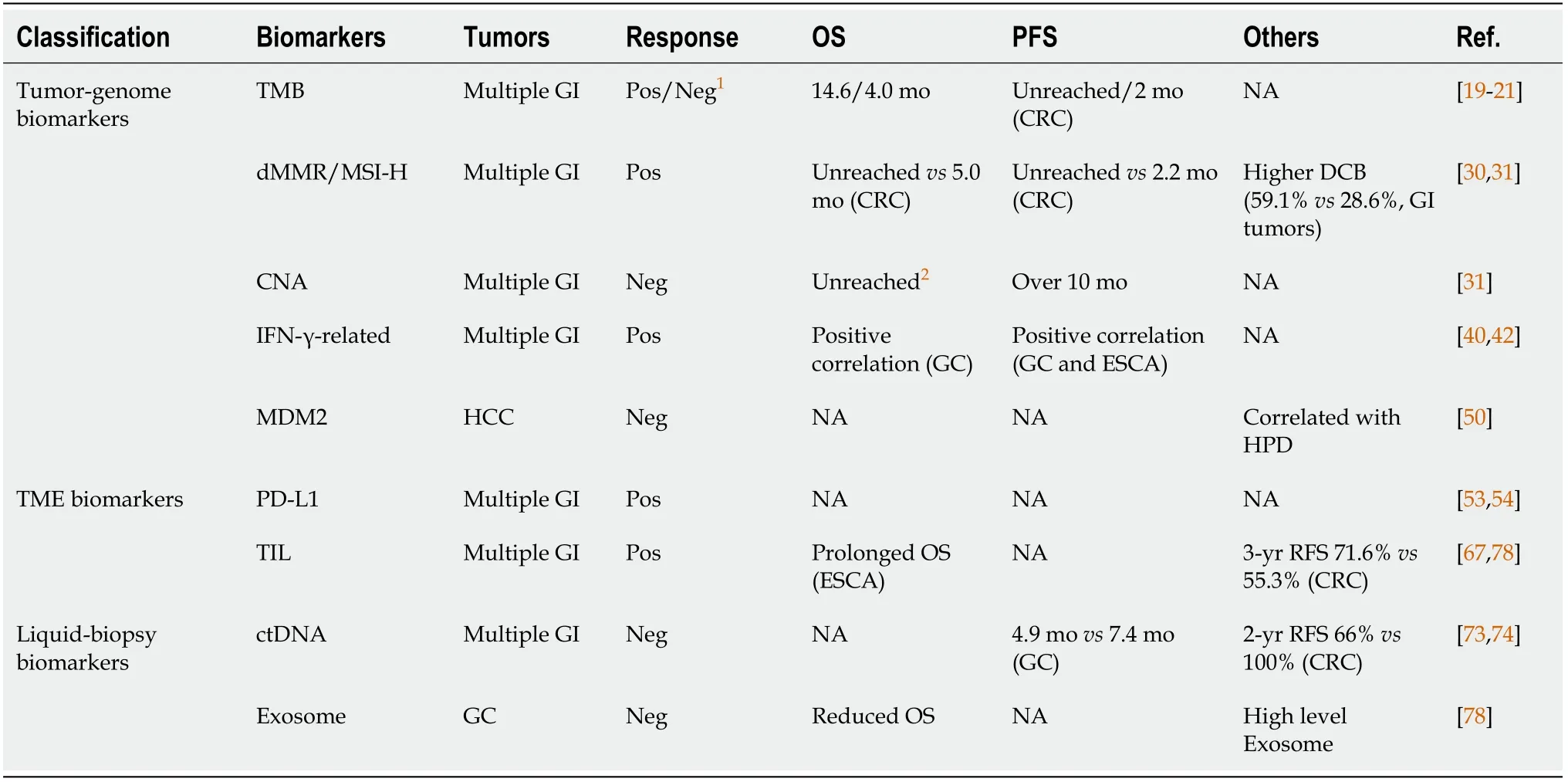
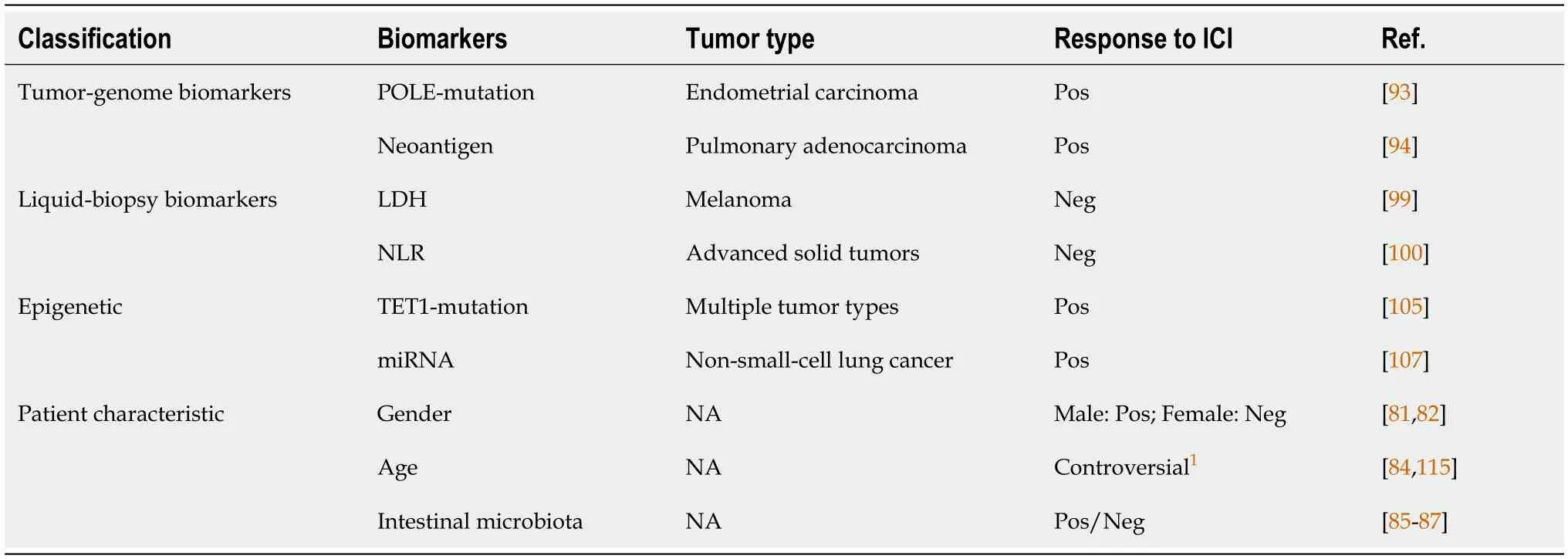
The details of the above biomarkers that have been studied or applied in GI cancers are summarized in Table 1.And in addition to the biomarkers mentioned above,here we also discuss and summarize some of the biomarkers that appear more frequently in a variety of other tumors,including patient characteristics,neoantigens,inflammatory indicators,and epigenetics (Table 2).These biomarkers deserve further prospective study and development in ICI-treated GI cancers,and provide new ideas for the identification of novel biomarkers as well.
Factors related to the patient's characteristics
The efficacy of ICI treatment is also highly dependent on patient's characteristics,such as gender,age,and the homeostasis of the body's internal environment.The application of these characteristics in GI cancers is not yet supported by a large amount of data,but the correlation of these characteristics with the efficacy of ICI treatment provides a novel idea for future studies,which can be combined with other markers to improve the predictive accuracy.The first point worth mentioning is the possible correlation between the efficacy of ICIs and the gender of the patient.A metaanalysis including 20 randomized controlled trials conducted by Conforti
[81]reported better efficacy of ICIs in male patients than in females[81].Schreiber
[82]suggested that women have more effective immunosurveillance mechanisms compared to men,and this immunosurveillance capacity allows women to be less immunogenic in advanced tumors.They further implied that women may have stronger immune escape mechanisms,and thus they may be more resistant to immunotherapy[82].
Age is also an important marker.There is a relationship between aging and restricted immune function,with significant effects on both innate and acquired immune responses[83].Nishijima
[84] reported an association with better ORR in patients aged less than 75 years treated with ICIs[84].In addition,the fraction and diversity of the intestinal microbiota were likewise found to be associated with the efficacy of ICIs,where effective patients tend to have high levels of polyphenism and ruminal cocci family[85].The intestinal microbiota can influence the process of cancer development and progression by altering the host immune system and regulating metabolism[86].It was evidenced that patients treated with antibiotics for 2 mo before or after ICI treatment had a significantly lower clinical benefit than those without antibiotics,probably because antibiotics disrupted the homeostasis of gut microbiota and certain dominant intestinal flora in patients[87].
POLE and neoantigen
As mentioned above,TMB and dMMR/MSI-H were biomarkers at the tumor genome level,and correspondingly,another one of interest needs to be presented here,which is POLE.Polymerase ε (encoded by the
gene) performs error correction during DNA replication,ensuring the accuracy of the replication process[88,89].Mutations in POLE severely affect the error correction function,leading to the accumulation of a large number of somatic mutations and elevated TMB.CD8
lymphocyte infiltration in tumors is also significantly increased,promoting the production of tumor-specific neoantigens[90-92].From a retrospective study conducted by Domingo
[90]including 6517 CRC patients,66 of them (1.0%) were found to have POLE mutations with the highest mutational burden,all with MSS[90].However,it is worth mentioning that even patients with the MSS type carry a highly mutated profile.Howitt
[93] reported that POLE mutations in endometrial carcinoma lead to an elevated tumor neoantigen load and PD-1 overexpression in tumor-infiltrating cells[93].These results indicated that POLE mutations have a role as prognostic markers,and the detection of POLE can also be applied to GI cancers to predict the survival benefit of ICI therapy.
TMB,dMMR/MSI-H,and POLE are all valid indicators as biomarkers,and there is a link between these three.As previously mentioned,mutations in POLE can lead to high levels of TMB[11].Chalmers
[11] indicated that MSI-H can be usually used as a subset of high TMB,and the vast majority of MSI-H samples also had high levels of TMB (83%),with 97% of them having TMB ≥ 10 Mut/Mb.Nevertheless,it depends on the tumor type,and in GI cancers such as gastric,duodenal,and small intestinal adenocarcinomas,MSI-H and high TMB are found almost simultaneously[11].Both can be used as combined biomarkers to predict the response to ICIs in GI cancers.
Common to all three biomarkers mentioned above is that they all increase neoantigen generation.Higher levels of TMB may increase the chance of immunogenic neoantigens[94].High levels of somatic mutations in MSI-H and POLE also lead to an increase in neoantigens[30].It means that these tumor cells are more likely to be recognized by immune cells,in which case the efficacy of ICIs is also more pronounced.It has been suggested that hypermethylation of the neoantigen gene promoter may be important for immune editing and tumor immune escape[95].Therefore,neoantigens are also in the scope of exploring ICIs biomarkers for GI cancers.Neoantigens are not only highly specific and strongly immunogenic,but are also ideal targets for immunotherapy.The presentation and recognition of neoantigens largely influence the outcome of ICI treatment,making it undoubtedly an important target for predicting the efficacy of ICIs[96].Studies have shown that in primary pulmonary adenocarcinoma,clonal neoantigen load is associated with a longer OS[94].The relationship between neoantigens and the clinical benefit of treating GI cancers needs to be supported by additional and more specific data.
Inflammatory indicators
GI cancers are similar to other types of tumors in that tumor-associated inflammatory processes often establish immune tolerance,promote tumor growth and metastasis,and activate oncogenic signal transduction pathways[97].Some conventional inflammatory indicators,such as neutrophil-to-lymphocyte ratio (NLR) and lactate dehydrogenase (LDH),have been used as ICI response biomarkers for a variety of tumors,which could also serve as promising markers in GI cancers[98].In a blood test performed on 66 melanoma patients treated with ICIs,baseline values of serum LDH and changes in LDH during ICI treatment were found to correlate with patient response and survival outcomes,with higher baseline serum LDH values and a 10%increase from baseline during treatment likely indicating inferior ICI efficacy[99].NLR has also been more established as a biomarker.According to the NLR kinetics study in patients with advanced solid tumors treated with PD-1/L1 inhibitors,the median OS of patients with high NLR was 8.5 mo,while the median OS of patients with low NLR was 19.4 mo[100].Similar results were found by Jiang
[101],showing that high NLR was associated with a poor OS and PFS[101].
Epigenetic markers
Epigenetic alterations are also an area of interest as potential biomarkers.As mentioned above,high levels of TMB tend to be correlated with a better ICI response,but some tumors with low-level TMB may improve the immunogenicity of their tumor neoplastic antigens through epigenetic modifications,when the efficacy of ICIs is instead better[102].In GC,alterations in the somatic epigenetic promoter have also been described to be associated with immune editing and tumor escape[103].It has also been shown that the CC family chemokine ligand 9 (CXCL9) is epigenetically modified to suppress its biological function,ultimately blocking effector T cells from infiltrating into the tumor bed for its immune function[104].In a report examining the relevance of DNA methylation-regulated genes to ICI response,mutated TET1 was significantly enriched among the 21 related genes studied in patients responding to ICIs.Moreover,mutant TET1 was strongly associated with a higher ORR,longer PFS,and better OS and DCB,which could serve as a novel predictive biomarker across multiple cancer types[105].
In addition to modifications such as methylation,miRNAs are also of interest for further development.In epigenetics,miRNA quantification is one of the most accessible markers.MiRNAs can be direct or indirect regulators of PD-L1 expression,as well as of many other immune checkpoints,such as LAG-3,TIM-3,BTLA,or CTLA-4[106].A study in NSCLC showed that serum miRNA profiles can discriminate responders to ICIs.In that study,Fan
[107] found that increased expression of miR-93,-200,-27a,-28,-424,and other miRNAs were significantly associated with prognosis,highlighting the predictive value of miRNAs[107].The emergence of TET1,miRNAs,and other epigenetic examples suggests that there are still more possibilities that need to be further explored in the field of GI tumors.
Then no time must be lost, said Hyacinthia, and she immediately turned herself into a river, Prince Milan into an iron bridge, and the charger into a blackbird
EMERGING TECHNOLOGIES FOR OPTIMIZING BIOMARKERS
Single-cell sequencing analysis
Moreover,with the evolving concept of precision medicine,biomarker research is facing the same trend.Tumors contain different and evolving cell populations,a property also known as tumor heterogeneity,which is a major driver of resistance to treatment and tumor metastasis and one of the factors affecting the efficacy of ICIs[108].It is essential to fully understand heterogeneity,especially in the TME.Analysis of TME heterogeneity and the phenotypes of various cell types by single-cell analysis techniques can help optimize existing therapeutic strategies or discover new ones,and improve the efficacy of the currently used biomarkers,although some limitations remain.In uveal melanoma,the single-cell analysis revealed that CD8
T cells predominantly express LAG3 rather than conventional PD-L1,revealing the limited availability of ICIs for treating this type of tumor[109].It illustrates that the selection of biomarkers in different tumor contexts should be further categorized and considered.In GI cancers,single-cell analysis techniques have also made a notable impact.In the study of GI stromal tumors,Mao
[110] applied single-cell transcriptome analysis to reveal their heterogeneity.They also observed that tumor cell related signatures with high proliferation rates were associated with a high risk of tumor malignancy and metastasis,suggesting that this may serve as a prognostic marker or complement[110].In a study of CRC by Di
[111],T-cell phenotypes were mapped by single-cell mass cytometry.They identified increased heterogeneity of T cells and immunosuppressive T-cell phenotypes in tumor lesions.Altering this immunosuppressive TME is important to improve the ICI response,and single-cell analysis provides very valuable information to improve the immune response in CRC[111].
One day, eight-year-old Rachel was helping3 me complete five (count ’em, five) emergency treatment forms for school. She would fill in the generic4 information (name, address, phone number), and I would add the rest (insurance numbers, doctor’s name, date, signature). After signing the forms, I checked them for accuracy. It was then that I noticed on each card, in the slot beside Mother’s Business Phone, Rachel had written “1-800-HEAVEN.
Apart from the transcriptomics mentioned above,multi-omics is more noteworthy in single-cell analysis.In a study by Zhou
[112],the percentage of fibroblasts with altered somatic copy number was found to be much higher in CRC than in adjacent normal tissues by using single-cell multi-omics sequencing.Five genes (
and
) were also identified as fibroblast-specific biomarkers of poorer prognosis in CRC[112].This study further explored new CAN-based biomarkers,of which single-cell multi-omics analysis is an essential and important part,which also provides us with new ideas in studying ICI response biomarkers in GI cancers as well.
Machine learning
Along with the growing development of bioinformatics,machine learning,and artificial intelligence,biomarkers will be further improved.For example,in the work of Lu
[113],tumor samples from patients with metastatic GI cancers treated with ICIs were sequenced for immuno-oncology (IO)-related gene targets and combined with the application of linear support vector machine learning strategy to construct an RNA signature (IO score) as a predictive model.Notably,its overall accuracy in discriminating DCB and NDB reached 94% and 83%,respectively,and the IO-score showed superior predictive value with higher odds ratio than the traditional biomarker[113].
CONCLUSION
Research in the field of ICIs has been steadily increasing.In GI cancers,ICI-related studies have also been emerging,addressing the importance of ICIs in tumor immunotherapy from different perspectives.Many recent ongoing studies in GI cancers also highlight the potential for diversification of ICIs,particularly in combination or neoadjuvant therapy,where the utility of ICIs has been further investigated.By combining chemotherapy and targeted agents,these studies provide insight into eradicating micrometastatic GI cancers,overcoming resistance to ICIs,and improving ICI treatment
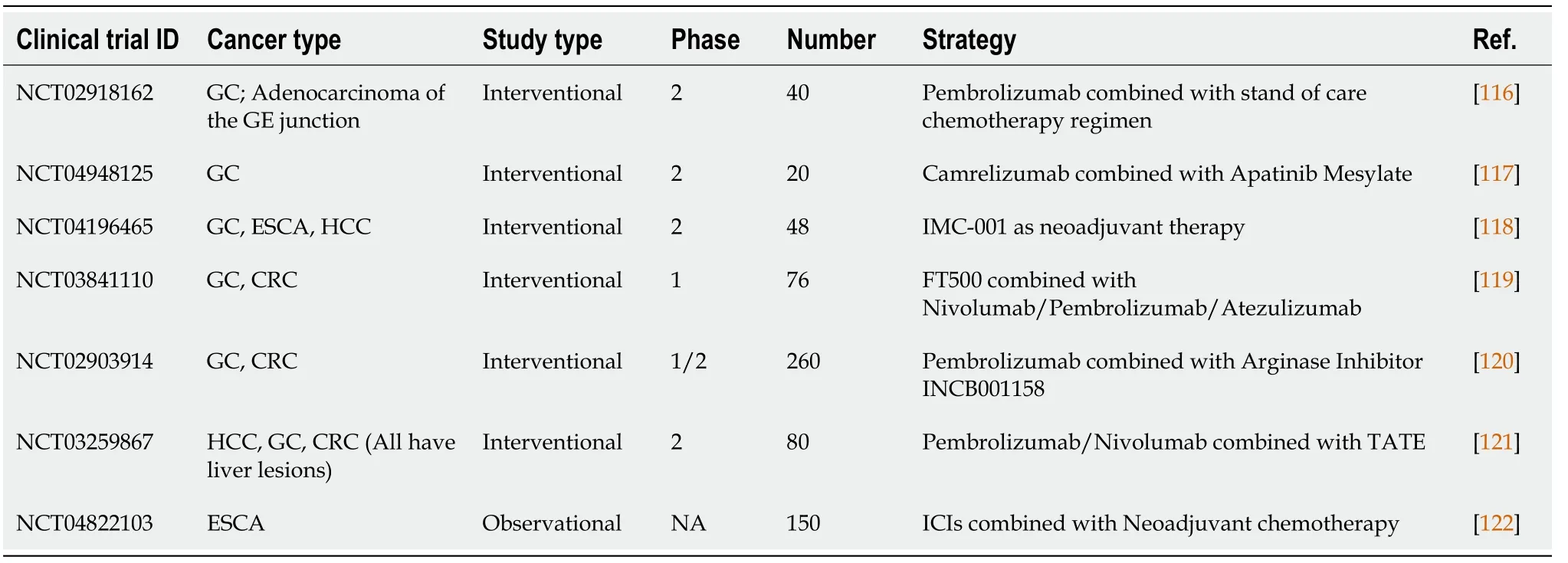
We summarize in Table 3 a number of clinical studies that are currently ongoing to provide a valuable reference for this purpose.However,it needs to be noticed that these ongoing clinical trials do not specifically target one or more biomarkers to predict response to ICIs.Rather,it is more about the combination of ICI therapy with other therapies,which may have little relevance to our topic.Nonetheless,these clinical trials can provide us with a wealth of useful information that we can use in subsequent data analysis for biomarker identification.
Although many new biomarkers have been identified in GI cancers,there is a relative lack of research compared to other tumor types such as melanoma and NSCLC,and validation from clinical trials is still lacking.In this review,we summarize not only biomarkers that are supported by studies in GI cancers,but also biomarkers that are informed in other tumors,in terms of tumor genomic information,TME,liquid biopsies,and epigenetic and patients' characteristics in relation to ICI response.Among these markers,studies on TMB and PD-L1 need to be further improved,and the delineation of cut-off values is not sufficiently clear,especially for PD-L1 expression,which has been shown in a number of studies to respond to ICIs in PD-L1-negative patients[52].As a stand-alone biomarker,PD-L1 is still considered to be controversial.In addition,markers associated with patient characteristics also have conflicting data,and current studies are not systematic and not clear enough and need to be confirmed by some large-scale prospective studies[114,115].Another key point that needs attention is that the current ICI predictive biomarkers for GI cancers are mostly focused on CRC cases,while they have relatively little application in other GI cancers such as GC and HCC,and more research investment is needed.
For the future trend of biomarkers,considering that a single biomarker is mostly insufficient,the strategy of combining two or more biomarkers is noteworthy,such as combining information from epigenetics and tumor genome,TMB and CNA in subgroup analysis,
The integration of multiple factors is necessary to improve accuracy.And along with the continuous research on ICIs therapy,biomarkers for combination therapy or neoadjuvant therapy also need to keep pace with the development to further promote precision therapy.Meanwhile,with the development of big data and bioinformatics,an increasing number of cutting-edge technologies such as machine learning,artificial intelligence,and single-cell analysis will also be applied for further optimization and refinement,making the efficacy of tumor immunotherapy steadily improved.For the current research,more prospective studies are needed,and more data will help to optimize these computational models.From this point of view,the identification of biomarkers that can be used to accurately predict ICI is just beginning,and much more remains to be done,which could become a major trend and focus in the future.
1 Arnold M,Abnet CC,Neale RE,Vignat J,Giovannucci EL,McGlynn KA,Bray F.Global Burden of 5 Major Types of Gastrointestinal Cancer.
2020;159:335-349.e15 [PMID:32247694 DOI:10.1053/j.gastro.2020.02.068]
2 Villanueva A.Hepatocellular Carcinoma.
2019;380:1450-1462 [PMID:30970190 DOI:10.1056/NEJMra1713263]
3 Abbott M,Ustoyev Y.Cancer and the Immune System:The History and Background of Immunotherapy.
2019;35:150923 [PMID:31526550 DOI:10.1016/j.soncn.2019.08.002]
4 Topalian SL,Drake CG,Pardoll DM.Immune checkpoint blockade:a common denominator approach to cancer therapy.
2015;27:450-461 [PMID:25858804 DOI:10.1016/j.ccell.2015.03.001]
5 Hazarika M,Chuk MK,Theoret MR,Mushti S,He K,Weis SL,Putman AH,Helms WS,Cao X,Li H,Zhao H,Zhao L,Welch J,Graham L,Libeg M,Sridhara R,Keegan P,Pazdur R.U.S.FDA Approval Summary:Nivolumab for Treatment of Unresectable or Metastatic Melanoma Following Progression on Ipilimumab.
2017;23:3484-3488 [PMID:28087644 DOI:10.1158/1078-0432.CCR-16-0712]
6 Ramagopal UA,Liu W,Garrett-Thomson SC,Bonanno JB,Yan Q,Srinivasan M,Wong SC,Bell A,Mankikar S,Rangan VS,Deshpande S,Korman AJ,Almo SC.Structural basis for cancer immunotherapy by the first-in-class checkpoint inhibitor ipilimumab.
2017;114:E4223-E4232 [PMID:28484017 DOI:10.1073/pnas.1617941114]
7 Postow MA,Callahan MK,Wolchok JD.Immune Checkpoint Blockade in Cancer Therapy.
2015;33:1974-1982 [PMID:25605845 DOI:10.1200/JCO.2014.59.4358]
8 Couzin-Frankel J.Breakthrough of the year 2013.Cancer immunotherapy.
2013;342:1432-1433 [PMID:24357284 DOI:10.1126/science.342.6165.1432]
9 Frampton GM,Fichtenholtz A,Otto GA,Wang K,Downing SR,He J,Schnall-Levin M,White J,Sanford EM,An P,Sun J,Juhn F,Brennan K,Iwanik K,Maillet A,Buell J,White E,Zhao M,Balasubramanian S,Terzic S,Richards T,Banning V,Garcia L,Mahoney K,Zwirko Z,Donahue A,Beltran H,Mosquera JM,Rubin MA,Dogan S,Hedvat CV,Berger MF,Pusztai L,Lechner M,Boshoff C,Jarosz M,Vietz C,Parker A,Miller VA,Ross JS,Curran J,Cronin MT,Stephens PJ,Lipson D,Yelensky R.Development and validation of a clinical cancer genomic profiling test based on massively parallel DNA sequencing.
2013;31:1023-1031 [PMID:24142049 DOI:10.1038/nbt.2696]
10 Rizvi H,Sanchez-Vega F,La K,Chatila W,Jonsson P,Halpenny D,Plodkowski A,Long N,Sauter JL,Rekhtman N,Hollmann T,Schalper KA,Gainor JF,Shen R,Ni A,Arbour KC,Merghoub T,Wolchok J,Snyder A,Chaft JE,Kris MG,Rudin CM,Socci ND,Berger MF,Taylor BS,Zehir A,Solit DB,Arcila ME,Ladanyi M,Riely GJ,Schultz N,Hellmann MD.Molecular Determinants of Response to Anti-Programmed Cell Death (PD)-1 and Anti-Programmed Death-Ligand 1 (PD-L1)Blockade in Patients With Non-Small-Cell Lung Cancer Profiled With Targeted Next-Generation Sequencing.
2018;36:633-641 [PMID:29337640 DOI:10.1200/JCO.2017.75.3384]
11 Chalmers ZR,Connelly CF,Fabrizio D,Gay L,Ali SM,Ennis R,Schrock A,Campbell B,Shlien A,Chmielecki J,Huang F,He Y,Sun J,Tabori U,Kennedy M,Lieber DS,Roels S,White J,Otto GA,Ross JS,Garraway L,Miller VA,Stephens PJ,Frampton GM.Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden.
2017;9:34 [PMID:28420421 DOI:10.1186/s13073-017-0424-2]
12 Sholl LM,Hirsch FR,Hwang D,Botling J,Lopez-Rios F,Bubendorf L,Mino-Kenudson M,Roden AC,Beasley MB,Borczuk A,Brambilla E,Chen G,Chou TY,Chung JH,Cooper WA,Dacic S,Lantuejoul S,Jain D,Lin D,Minami Y,Moreira A,Nicholson AG,Noguchi M,Papotti M,Pelosi G,Poleri C,Rekhtman N,Tsao MS,Thunnissen E,Travis W,Yatabe Y,Yoshida A,Daigneault JB,Zehir A,Peters S,Wistuba II,Kerr KM,Longshore JW.The Promises and Challenges of Tumor Mutation Burden as an Immunotherapy Biomarker:A Perspective from the International Association for the Study of Lung Cancer Pathology Committee.
2020;15:1409-1424 [PMID:32522712 DOI:10.1016/j.jtho.2020.05.019]
13 Yarchoan M,Hopkins A,Jaffee EM.Tumor Mutational Burden and Response Rate to PD-1 Inhibition.
2017;377:2500-2501 [PMID:29262275 DOI:10.1056/NEJMc1713444]
14 Kim ST,Cristescu R,Bass AJ,Kim KM,Odegaard JI,Kim K,Liu XQ,Sher X,Jung H,Lee M,Lee S,Park SH,Park JO,Park YS,Lim HY,Lee H,Choi M,Talasaz A,Kang PS,Cheng J,Loboda A,Lee J,Kang WK.Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer.
2018;24:1449-1458 [PMID:30013197 DOI:10.1038/s41591-018-0101-z]
15 Goodman AM,Kato S,Bazhenova L,Patel SP,Frampton GM,Miller V,Stephens PJ,Daniels GA,Kurzrock R.Tumor Mutational Burden as an Independent Predictor of Response to Immunotherapy in Diverse Cancers.
2017;16:2598-2608 [PMID:28835386 DOI:10.1158/1535-7163.MCT-17-0386]
16 Singal G,Miller PG,Agarwala V,Li G,Kaushik G,Backenroth D,Gossai A,Frampton GM,Torres AZ,Lehnert EM,Bourque D,O'Connell C,Bowser B,Caron T,Baydur E,Seidl-Rathkopf K,Ivanov I,Alpha-Cobb G,Guria A,He J,Frank S,Nunnally AC,Bailey M,Jaskiw A,Feuchtbaum D,Nussbaum N,Abernethy AP,Miller VA.Association of Patient Characteristics and Tumor Genomics With Clinical Outcomes Among Patients With Non-Small Cell Lung Cancer Using a Clinicogenomic Database.
2019;321:1391-1399 [PMID:30964529 DOI:10.1001/jama.2019.3241]
17 Fang W,Ma Y,Yin JC,Hong S,Zhou H,Wang A,Wang F,Bao H,Wu X,Yang Y,Huang Y,Zhao H,Shao YW,Zhang L.Comprehensive Genomic Profiling Identifies Novel Genetic Predictors of Response to Anti-PD-(L)1 Therapies in Non-Small Cell Lung Cancer.
2019;25:5015-5026 [PMID:31085721 DOI:10.1158/1078-0432.CCR-19-0585]
18 Marabelle A,Fakih M,Lopez J,Shah M,Shapira-Frommer R,Nakagawa K,Chung H C,Kindler H L,Lopez-Martin J A,Miller W H,Jr.,Italiano A,Kao S,Piha-Paul S A,Delord J P,McWilliams R R,Fabrizio D A,Aurora-Garg D,Xu L,Jin F,Norwood K,Bang Y J.Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab:Prospective biomarker analysis of the multicohort,open-label,phase 2 keynote-158 study.
2020;21:1353-1365 [DOI:10.1016/s1470-2045(20)30445-9]
19 Xu R-H,Wang F,Wei X-L,Xu N,Shen L,Dai G,Yuan X,Chen Y,Yang S,Shi J,Hu X-C,Lin X,Zhang Q,Feng J F,Ba Y,Liu Y,Wu H,Feng H,Yao S.Tumor mutational burden identifies chemorefractory gastric cancer with overall survival advantage after receiving toripalimab,a pd-1 antibody.
2019;37:4021-4021 [DOI:10.1200/jco.2019.37.15_suppl.4021]
20 Wang F,Wei XL,Wang FH,Xu N,Shen L,Dai GH,Yuan XL,Chen Y,Yang SJ,Shi JH,Hu XC,Lin XY,Zhang QY,Feng JF,Ba Y,Liu YP,Li W,Shu YQ,Jiang Y,Li Q,Wang JW,Wu H,Feng H,Yao S,Xu RH.Safety,efficacy and tumor mutational burden as a biomarker of overall survival benefit in chemo-refractory gastric cancer treated with toripalimab,a PD-1 antibody in phase Ib/II clinical trial NCT02915432.
2019;30:1479-1486 [PMID:31236579 DOI:10.1093/annonc/mdz197]
21 Schrock AB,Ouyang C,Sandhu J,Sokol E,Jin D,Ross JS,Miller VA,Lim D,Amanam I,Chao J,Catenacci D,Cho M,Braiteh F,Klempner SJ,Ali SM,Fakih M.Tumor mutational burden is predictive of response to immune checkpoint inhibitors in MSI-high metastatic colorectal cancer.
2019;30:1096-1103 [PMID:31038663 DOI:10.1093/annonc/mdz134]
22 Addeo A,Friedlaender A,Banna GL,Weiss GJ.TMB or not TMB as a biomarker:That is the question.
2021;163:103374 [PMID:34087341 DOI:10.1016/j.critrevonc.2021.103374]
23 Topalian SL,Taube JM,Anders RA,Pardoll DM.Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy.
2016;16:275-287 [PMID:27079802 DOI:10.1038/nrc.2016.36]
24 Bai R,Lv Z,Xu D,Cui J.Predictive biomarkers for cancer immunotherapy with immune checkpoint inhibitors.
2020;8:34 [PMID:32864131 DOI:10.1186/s40364-020-00209-0]
25 Svrcek M,Lascols O,Cohen R,Collura A,Jonchère V,Fléjou JF,Buhard O,Duval A.MSI/MMRdeficient tumor diagnosis:Which standard for screening and for diagnosis?
2019;106:119-128 [PMID:30713006 DOI:10.1016/j.bulcan.2018.12.008]
26 Li K,Luo H,Huang L,Zhu X.Microsatellite instability:a review of what the oncologist should know.
2020;20:16 [PMID:31956294 DOI:10.1186/s12935-019-1091-8]
27 Salem ME,Puccini A,Grothey A,Raghavan D,Goldberg RM,Xiu J,Korn WM,Weinberg BA,Hwang JJ,Shields AF,Marshall JL,Philip PA,Lenz HJ.Landscape of Tumor Mutation Load,Mismatch Repair Deficiency,and PD-L1 Expression in a Large Patient Cohort of Gastrointestinal Cancers.
2018;16:805-812 [PMID:29523759 DOI:10.1158/1541-7786.MCR-17-0735]
28 Schwitalle Y,Kloor M,Eiermann S,Linnebacher M,Kienle P,Knaebel HP,Tariverdian M,Benner A,von Knebel Doeberitz M.Immune response against frameshift-induced neopeptides in HNPCC patients and healthy HNPCC mutation carriers.
2008;134:988-997 [PMID:18395080 DOI:10.1053/j.gastro.2008.01.015]
29 Solomon BL,Garrido-Laguna I.Upper gastrointestinal malignancies in 2017:current perspectives and future approaches.
2018;14:947-962 [PMID:29542354 DOI:10.2217/fon-2017-0597]
30 Le DT,Uram JN,Wang H,Bartlett BR,Kemberling H,Eyring AD,Skora AD,Luber BS,Azad NS,Laheru D,Biedrzycki B,Donehower RC,Zaheer A,Fisher GA,Crocenzi TS,Lee JJ,Duffy SM,Goldberg RM,de la Chapelle A,Koshiji M,Bhaijee F,Huebner T,Hruban RH,Wood LD,Cuka N,Pardoll DM,Papadopoulos N,Kinzler KW,Zhou S,Cornish TC,Taube JM,Anders RA,Eshleman JR,Vogelstein B,Diaz LA Jr.PD-1 Blockade in Tumors with Mismatch-Repair Deficiency.
2015;372:2509-2520 [PMID:26028255 DOI:10.1056/NEJMoa1500596]
31 Lu Z,Chen H,Li S,Gong J,Li J,Zou J,Wu L,Yu J,Han W,Sun H,Jiao X,Zhang X,Peng Z,Lu M,Wang Z,Zhang H,Shen L.Tumor copy-number alterations predict response to immunecheckpoint-blockade in gastrointestinal cancer.
2020;8 [PMID:32792358 DOI:10.1136/jitc-2019-000374]
32 Roh W,Chen PL,Reuben A,Spencer CN,Prieto PA,Miller JP,Gopalakrishnan V,Wang F,Cooper ZA,Reddy SM,Gumbs C,Little L,Chang Q,Chen WS,Wani K,De Macedo MP,Chen E,Austin-Breneman JL,Jiang H,Roszik J,Tetzlaff MT,Davies MA,Gershenwald JE,Tawbi H,Lazar AJ,Hwu P,Hwu WJ,Diab A,Glitza IC,Patel SP,Woodman SE,Amaria RN,Prieto VG,Hu J,Sharma P,Allison JP,Chin L,Zhang J,Wargo JA,Futreal PA.Integrated molecular analysis of tumor biopsies on sequential CTLA-4 and PD-1 blockade reveals markers of response and resistance.
2017;9 [PMID:28251903 DOI:10.1126/scitranslmed.aah3560]
33 Budczies J,Seidel A,Christopoulos P,Endris V,Kloor M,Gy?rffy B,Seliger B,Schirmacher P,Stenzinger A,Denkert C.Integrated analysis of the immunological and genetic status in and across cancer types:impact of mutational signatures beyond tumor mutational burden.
2018;7:e1526613 [PMID:30524909 DOI:10.1080/2162402X.2018.1526613]
34 Smeets D,Miller IS,O'Connor DP,Das S,Moran B,Boeckx B,Gaiser T,Betge J,Barat A,Klinger R,van Grieken NCT,Cremolini C,Prenen H,Mazzone M,Depreeuw J,Bacon O,Fender B,Brady J,Hennessy BT,McNamara DA,Kay E,Verheul HM,Maarten N,Gallagher WM,Murphy V,Prehn JHM,Koopman M,Punt CJA,Loupakis F,Ebert MPA,Ylstra B,Lambrechts D,Byrne AT.Copy number load predicts outcome of metastatic colorectal cancer patients receiving bevacizumab combination therapy.
2018;9:4112 [PMID:30291241 DOI:10.1038/s41467-018-06567-6]
35 Possick JD.Pulmonary Toxicities from Checkpoint Immunotherapy for Malignancy.
2017;38:223-232 [PMID:28477635 DOI:10.1016/j.ccm.2016.12.012]
36 Garcia-Diaz A,Shin DS,Moreno BH,Saco J,Escuin-Ordinas H,Rodriguez GA,Zaretsky JM,Sun L,Hugo W,Wang X,Parisi G,Saus CP,Torrejon DY,Graeber TG,Comin-Anduix B,Hu-Lieskovan S,Damoiseaux R,Lo RS,Ribas A.Interferon Receptor Signaling Pathways Regulating PD-L1 and PD-L2 Expression.
2017;19:1189-1201 [PMID:28494868 DOI:10.1016/j.celrep.2017.04.031]
37 Grasso CS,Tsoi J,Onyshchenko M,Abril-Rodriguez G,Ross-Macdonald P,Wind-Rotolo M,Champhekar A,Medina E,Torrejon DY,Shin DS,Tran P,Kim YJ,Puig-Saus C,Campbell K,Vega-Crespo A,Quist M,Martignier C,Luke JJ,Wolchok JD,Johnson DB,Chmielowski B,Hodi FS,Bhatia S,Sharfman W,Urba WJ,Slingluff CL,Jr Diab A,Haanen J,Algarra SM,Pardoll DM,Anagnostou V,Topalian SL,Velculescu VE,Speiser DE,Kalbasi A,Ribas A.Conserved interferonγ signaling drives clinical response to immune checkpoint blockade therapy in melanoma.
2020;38:500-515.e503 [DOI:10.1016/j.ccell.2020.11.015]
38 Karachaliou N,Gonzalez-Cao M,Crespo G,Drozdowskyj A,Aldeguer E,Gimenez-Capitan A,Teixido C,Molina-Vila MA,Viteri S,De Los Llanos Gil M,Algarra SM,Perez-Ruiz E,Marquez-Rodas I,Rodriguez-Abreu D,Blanco R,Puertolas T,Royo MA,Rosell R.Interferon gamma,an important marker of response to immune checkpoint blockade in non-small cell lung cancer and melanoma patients.
2018;10:1758834017749748 [PMID:29383037 DOI:10.1177/1758834017749748]
39 Higgs BW,Morehouse CA,Streicher K,Brohawn PZ,Pilataxi F,Gupta A,Ranade K.Interferon Gamma Messenger RNA Signature in Tumor Biopsies Predicts Outcomes in Patients with Non-Small Cell Lung Carcinoma or Urothelial Cancer Treated with Durvalumab.
2018;24:3857-3866 [PMID:29716923 DOI:10.1158/1078-0432.CCR-17-3451]
40 Doi T,Piha-Paul SA,Jalal SI,Saraf S,Lunceford J,Koshiji M,Bennouna J.Safety and Antitumor Activity of the Anti-Programmed Death-1 Antibody Pembrolizumab in Patients With Advanced Esophageal Carcinoma.
2018;36:61-67 [PMID:29116900 DOI:10.1200/JCO.2017.74.9846]
41 Sasaki S,Nishikawa J,Sakai K,Iizasa H,Yoshiyama H,Yanagihara M,Shuto T,Shimokuri K,Kanda T,Suehiro Y,Yamasaki T,Sakaida I.EBV-associated gastric cancer evades T-cell immunity by PD-1/PD-L1 interactions.
2019;22:486-496 [PMID:30264329 DOI:10.1007/s10120-018-0880-4]
42 Muro K,Chung HC,Shankaran V,Geva R,Catenacci D,Gupta S,Eder JP,Golan T,Le DT,Burtness B,McRee AJ,Lin CC,Pathiraja K,Lunceford J,Emancipator K,Juco J,Koshiji M,Bang YJ.Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012):a multicentre,open-label,phase 1b trial.
2016;17:717-726 [PMID:27157491 DOI:10.1016/S1470-2045(16)00175-3]
43 Darnell JE,Kerr IM,Stark GR.Jak-stat pathways and transcriptional activation in response to ifns and other extracellular signaling proteins.
1994;264:1415-1421 [DOI:10.1126/science.8197455]
44 Shin D S,Zaretsky JM,Escuin-Ordinas H,Garcia-Diaz A,Hu-Lieskovan S,Kalbasi A,Grasso CS,Hugo W,Sandoval S,Torrejon DY,Palaskas N,Rodriguez GA,Parisi G,Azhdam A,Chmielowski B,Cherry G,Seja E,Berent-Maoz B,Shintaku IP,Le DT,Pardoll DM,Diaz LA,Jr Tumeh PC,Graeber TG,Lo RS,Comin-Anduix B,Ribas A.Primary resistance to pd-1 blockade mediated by jak1/2 mutations.
2017;7:188-201 [DOI:10.1158/2159-8290.cd-16-1223]
45 Albacker LA,Wu J,Smith P,Warmuth M,Stephens PJ,Zhu P,Yu L,Chmielecki J.Loss of function JAK1 mutations occur at high frequency in cancers with microsatellite instability and are suggestive of immune evasion.
2017;12:e0176181 [PMID:29121062 DOI:10.1371/journal.pone.0176181]
46 Gudikote JP,Cascone T,Poteete A,Sitthideatphaiboon P,Wu Q,Morikawa N,Zhang F,Peng S,Tong P,Li L,Shen L,Nilsson M,Jones P,Sulman EP,Wang J,Bourdon JC,Johnson FM,Heymach JV.Inhibition of nonsense-mediated decay rescues p53β/γ isoform expression and activates the p53 pathway in MDM2-overexpressing and select p53-mutant cancers.
2021;297:101163[PMID:34481841 DOI:10.1016/j.jbc.2021.101163]
47 Kato S,Goodman A,Walavalkar V,Barkauskas DA,Sharabi A,Kurzrock R.Hyperprogressors after Immunotherapy:Analysis of Genomic Alterations Associated with Accelerated Growth Rate.
2017;23:4242-4250 [PMID:28351930 DOI:10.1158/1078-0432.CCR-16-3133]
48 Sahin I,Zhang S,Navaraj A,Zhou L,Dizon D,Safran H,El-Deiry WS.AMG-232 sensitizes high MDM2-expressing tumor cells to T-cell-mediated killing.
2020;6:57 [PMID:32655895 DOI:10.1038/s41420-020-0292-1]
49 Cao H,Chen X,Wang Z,Wang L,Xia Q,Zhang W.The role of MDM2-p53 axis dysfunction in the hepatocellular carcinoma transformation.
2020;6:53 [PMID:32595984 DOI:10.1038/s41420-020-0287-y]
50 Wu L,Quan W,Luo Q,Pan Y,Peng D,Zhang G.Identification of an Immune-Related Prognostic Predictor in Hepatocellular Carcinoma.
2020;7:567950 [PMID:33195412 DOI:10.3389/fmolb.2020.567950]
51 Doroshow DB,Bhalla S,Beasley MB,Sholl LM,Kerr KM,Gnjatic S,Wistuba II,Rimm DL,Tsao MS,Hirsch FR.PD-L1 as a biomarker of response to immune-checkpoint inhibitors.
2021;18:345-362 [PMID:33580222 DOI:10.1038/s41571-021-00473-5]
52 Patel SP,Kurzrock R.PD-L1 Expression as a Predictive Biomarker in Cancer Immunotherapy.
2015;14:847-856 [PMID:25695955 DOI:10.1158/1535-7163.MCT-14-0983]
53 Cui C,Yu B,Jiang Q,Li X,Shi K,Yang Z.The roles of PD-1/PD-L1 and its signalling pathway in gastrointestinal tract cancers.
2019;46:3-10 [PMID:30161295 DOI:10.1111/1440-1681.13028]
54 Das S,Cimino S,Davis S,Ciombor K.All in the Levels-Programmed Death-Ligand 1 Expression as a Biomarker for Immune Checkpoint Inhibitor Response in Patients with Gastrointestinal Cancer.
2021;26:e186-e188 [PMID:32945067 DOI:10.1002/onco.13526]
55 Stein A,Moehler M,Trojan J,Goekkurt E,Vogel A.Immuno-oncology in GI tumours:Clinical evidence and emerging trials of PD-1/PD-L1 antagonists.
2018;130:13-26[PMID:30196908 DOI:10.1016/j.critrevonc.2018.07.001]
56 Nishino M,Ramaiya NH,Hatabu H,Hodi FS.Monitoring immune-checkpoint blockade:response evaluation and biomarker development.
2017;14:655-668 [PMID:28653677 DOI:10.1038/nrclinonc.2017.88]
57 Meng X,Huang Z,Teng F,Xing L,Yu J.Predictive biomarkers in PD-1/PD-L1 checkpoint blockade immunotherapy.
2015;41:868-876 [PMID:26589760 DOI:10.1016/j.ctrv.2015.11.001]
58 Sacher AG,Gandhi L.Biomarkers for the Clinical Use of PD-1/PD-L1 Inhibitors in Non-Small-Cell Lung Cancer:A Review.
2016;2:1217-1222 [PMID:27310809 DOI:10.1001/jamaoncol.2016.0639]
59 Hutarew G.PD-L1 testing,fit for routine evaluation?
2016;9:201-206 [PMID:28058063 DOI:10.1007/s12254-016-0292-2]
60 Ribas A,Hu-Lieskovan S.What does PD-L1 positive or negative mean?
2016;213:2835-2840 [PMID:27903604 DOI:10.1084/jem.20161462]
61 Garber K.Pursuit of tumor-infiltrating lymphocyte immunotherapy speeds up.
2019;37:969-971 [PMID:31485043 DOI:10.1038/d41587-019-00023-6]
62 Halapi E.Oligoclonal T cells in human cancer.
1998;15:203-211 [PMID:9951682 DOI:10.1007/BF02787202]
63 Llosa NJ,Cruise M,Tam A,Wicks EC,Hechenbleikner EM,Taube JM,Blosser RL,Fan H,Wang H,Luber BS,Zhang M,Papadopoulos N,Kinzler KW,Vogelstein B,Sears CL,Anders RA,Pardoll DM,Housseau F.The vigorous immune microenvironment of microsatellite instable colon cancer is balanced by multiple counter-inhibitory checkpoints.
2015;5:43-51 [PMID:25358689 DOI:10.1158/2159-8290.CD-14-0863]
64 Tumeh PC,Harview CL,Yearley JH,Shintaku IP,Taylor EJ,Robert L,Chmielowski B,Spasic M,Henry G,Ciobanu V,West AN,Carmona M,Kivork C,Seja E,Cherry G,Gutierrez AJ,Grogan TR,Mateus C,Tomasic G,Glaspy JA,Emerson RO,Robins H,Pierce RH,Elashoff DA,Robert C,Ribas A.PD-1 blockade induces responses by inhibiting adaptive immune resistance.
2014;515:568-571 [PMID:25428505 DOI:10.1038/nature13954]
65 Tokito T,Azuma K,Kawahara A,Ishii H,Yamada K,Matsuo N,Kinoshita T,Mizukami N,Ono H,Kage M,Hoshino T.Predictive relevance of PD-L1 expression combined with CD8+ TIL density in stage III non-small cell lung cancer patients receiving concurrent chemoradiotherapy.
2016;55:7-14 [PMID:26771872 DOI:10.1016/j.ejca.2015.11.020]
66 Gibney GT,Weiner LM,Atkins MB.Predictive biomarkers for checkpoint inhibitor-based immunotherapy.
2016;17:e542-e551 [PMID:27924752 DOI:10.1016/S1470-2045(16)30406-5]
67 Xiao B,Peng J,Wang Y,Deng Y,Ou Q,Wu X,Lin J,Pan Z,Zhang L.Prognostic value of tumor infiltrating lymphocytes combined with PD-L1 expression for patients with solitary colorectal cancer liver metastasis.
2020;8:1221 [PMID:33178753 DOI:10.21037/atm-20-2762a]
68 Yagi T,Baba Y,Ishimoto T,Iwatsuki M,Miyamoto Y,Yoshida N,Watanabe M,Baba H.PD-L1 Expression,Tumor-infiltrating Lymphocytes,and Clinical Outcome in Patients With Surgically Resected Esophageal Cancer.
2019;269:471-478 [PMID:29206673 DOI:10.1097/SLA.0000000000002616]
69 Simoni Y,Becht E,Fehlings M,Loh CY,Koo SL,Teng KWW,Yeong JPS,Nahar R,Zhang T,Kared H,Duan K,Ang N,Poidinger M,Lee YY,Larbi A,Khng AJ,Tan E,Fu C,Mathew R,Teo M,Lim WT,Toh CK,Ong BH,Koh T,Hillmer AM,Takano A,Lim TKH,Tan EH,Zhai W,Tan DSW,Tan IB,Newell EW.Bystander CD8
T cells are abundant and phenotypically distinct in human tumour infiltrates.
2018;557:575-579 [PMID:29769722 DOI:10.1038/s41586-018-0130-2]
70 Poulet G,Massias J,Taly V.Liquid Biopsy:General Concepts.
2019;63:449-455[PMID:31091522 DOI:10.1159/000499337]
71 Wu X,Li J,Gassa A,Buchner D,Alakus H,Dong Q,Ren N,Liu M,Odenthal M,Stippel D,Bruns C,Zhao Y,Wahba R.Circulating tumor DNA as an emerging liquid biopsy biomarker for early diagnosis and therapeutic monitoring in hepatocellular carcinoma.
2020;16:1551-1562 [PMID:32226301 DOI:10.7150/ijbs.44024]
72 Lee JH,Long GV,Boyd S,Lo S,Menzies AM,Tembe V,Guminski A,Jakrot V,Scolyer RA,Mann GJ,Kefford RF,Carlino MS,Rizos H.Circulating tumour DNA predicts response to anti-PD1 antibodies in metastatic melanoma.
2017;28:1130-1136 [PMID:28327969 DOI:10.1093/annonc/mdx026]
73 Lecomte T,Berger A,Zinzindohoué F,Micard S,Landi B,Blons H,Beaune P,Cugnenc PH,Laurent-Puig P.Detection of free-circulating tumor-associated DNA in plasma of colorectal cancer patients and its association with prognosis.
2002;100:542-548 [PMID:12124803 DOI:10.1002/ijc.10526]
74 Jin Y,Chen DL,Wang F,Yang CP,Chen XX,You JQ,Huang JS,Shao Y,Zhu DQ,Ouyang YM,Luo HY,Wang ZQ,Wang FH,Li YH,Xu RH,Zhang DS.The predicting role of circulating tumor DNA landscape in gastric cancer patients treated with immune checkpoint inhibitors.
2020;19:154 [PMID:33126883 DOI:10.1186/s12943-020-01274-7]
75 Kulasinghe A,Perry C,Kenny L,Warkiani ME,Nelson C,Punyadeera C.PD-L1 expressing circulating tumour cells in head and neck cancers.
2017;17:333 [PMID:28511705 DOI:10.1186/s12885-017-3316-3]
76 Bobrie A,Colombo M,Raposo G,Théry C.Exosome secretion:molecular mechanisms and roles in immune responses.
2011;12:1659-1668 [PMID:21645191 DOI:10.1111/j.1600-0854.2011.01225.x]
77 Colombo M,Raposo G,Théry C.Biogenesis,secretion,and intercellular interactions of exosomes and other extracellular vesicles.
2014;30:255-289 [PMID:25288114 DOI:10.1146/annurev-cellbio-101512-122326]
78 Zhang H,Deng T,Liu R,Bai M,Zhou L,Wang X,Li S,Yang H,Li J,Ning T,Huang D,Li H,Zhang L,Ying G,Ba Y.Exosome-delivered EGFR regulates liver microenvironment to promote gastric cancer liver metastasis.
2017;8:15016 [PMID:28393839 DOI:10.1038/ncomms15016]
79 Del Re M,Marconcini R,Pasquini G,Rofi E,Vivaldi C,Bloise F,Restante G,Arrigoni E,Caparello C,Bianco MG,Crucitta S,Petrini I,Vasile E,Falcone A,Danesi R.PD-L1 mRNA expression in plasma-derived exosomes is associated with response to anti-PD-1 antibodies in melanoma and NSCLC.
2018;118:820-824 [PMID:29509748 DOI:10.1038/bjc.2018.9]
80 Fan Y,Che X,Qu J,Hou K,Wen T,Li Z,Li C,Wang S,Xu L,Liu Y,Qu X.Exosomal PD-L1 Retains Immunosuppressive Activity and is Associated with Gastric Cancer Prognosis.
2019;26:3745-3755 [PMID:31087180 DOI:10.1245/s10434-019-07431-7]
81 Conforti F,Pala L,Bagnardi V,De Pas T,Martinetti M,Viale G,Gelber RD,Goldhirsch A.Cancer immunotherapy efficacy and patients' sex:a systematic review and meta-analysis.
2018;19:737-746 [PMID:29778737 DOI:10.1016/S1470-2045(18)30261-4]
82 Schreiber RD,Old LJ,Smyth MJ.Cancer immunoediting:integrating immunity's roles in cancer suppression and promotion.
2011;331:1565-1570 [PMID:21436444 DOI:10.1126/science.1203486]
83 Fulop T,Larbi A,Kotb R,de Angelis F,Pawelec G.Aging,immunity,and cancer.
2011;11:537-550 [PMID:21712020]
84 Nishijima TF,Muss HB,Shachar SS,Moschos SJ.Comparison of efficacy of immune checkpoint inhibitors (ICIs) between younger and older patients:A systematic review and meta-analysis.
2016;45:30-37 [PMID:26946217 DOI:10.1016/j.ctrv.2016.02.006]
85 Gopalakrishnan V,Spencer CN,Nezi L,Reuben A,Andrews MC,Karpinets TV,Prieto PA,Vicente D,Hoffman K,Wei SC,Cogdill AP,Zhao L,Hudgens CW,Hutchinson DS,Manzo T,Petaccia de Macedo M,Cotechini T,Kumar T,Chen WS,Reddy SM,Szczepaniak Sloane R,Galloway-Pena J,Jiang H,Chen PL,Shpall EJ,Rezvani K,Alousi AM,Chemaly RF,Shelburne S,Vence LM,Okhuysen PC,Jensen VB,Swennes AG,McAllister F,Marcelo Riquelme Sanchez E,Zhang Y,Le Chatelier E,Zitvogel L,Pons N,Austin-Breneman JL,Haydu LE,Burton EM,Gardner JM,Sirmans E,Hu J,Lazar AJ,Tsujikawa T,Diab A,Tawbi H,Glitza IC,Hwu WJ,Patel SP,Woodman SE,Amaria RN,Davies MA,Gershenwald JE,Hwu P,Lee JE,Zhang J,Coussens LM,Cooper ZA,Futreal PA,Daniel CR,Ajami NJ,Petrosino JF,Tetzlaff MT,Sharma P,Allison JP,Jenq RR,Wargo JA.Gut microbiome modulates response to anti-PD-1 immunotherapy in melanoma patients.
2018;359:97-103 [PMID:29097493 DOI:10.1126/science.aan4236]
86 Tanaka Y,Shimizu S,Shirotani M,Yorozu K,Kitamura K,Oehorumu M,Kawai Y,Fukuzawa Y.Nutrition and Cancer Risk from the Viewpoint of the Intestinal Microbiome.
2021;13[PMID:34684330 DOI:10.3390/nu13103326]
87 Routy B,Le Chatelier E,Derosa L,Duong CPM,Alou MT,Daillère R,Fluckiger A,Messaoudene M,Rauber C,Roberti MP,Fidelle M,Flament C,Poirier-Colame V,Opolon P,Klein C,Iribarren K,Mondragón L,Jacquelot N,Qu B,Ferrere G,Clémenson C,Mezquita L,Masip JR,Naltet C,Brosseau S,Kaderbhai C,Richard C,Rizvi H,Levenez F,Galleron N,Quinquis B,Pons N,Ryffel B,Minard-Colin V,Gonin P,Soria JC,Deutsch E,Loriot Y,Ghiringhelli F,Zalcman G,Goldwasser F,Escudier B,Hellmann MD,Eggermont A,Raoult D,Albiges L,Kroemer G,Zitvogel L.Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors.
2018;359:91-97 [PMID:29097494 DOI:10.1126/science.aan3706]
88 Bourdais R,Rousseau B,Pujals A,Boussion H,Joly C,Guillemin A,Baumgaertner I,Neuzillet C,Tournigand C.Polymerase proofreading domain mutations:New opportunities for immunotherapy in hypermutated colorectal cancer beyond MMR deficiency.
2017;113:242-248 [PMID:28427513 DOI:10.1016/j.critrevonc.2017.03.027]
89 Nebot-Bral L,Brandao D,Verlingue L,Rouleau E,Caron O,Despras E,El-Dakdouki Y,Champiat S,Aoufouchi S,Leary A,Marabelle A,Malka D,Chaput N,Kannouche PL.Hypermutated tumours in the era of immunotherapy:The paradigm of personalised medicine.
2017;84:290-303 [PMID:28846956 DOI:10.1016/j.ejca.2017.07.026]
90 Domingo E,Freeman-Mills L,Rayner E,Glaire M,Briggs S,Vermeulen L,Fessler E,Medema JP,Boot A,Morreau H,van Wezel T,Liefers GJ,Lothe RA,Danielsen SA,Sveen A,Nesbakken A,Zlobec I,Lugli A,Koelzer VH,Berger MD,Castellví-Bel S,Mu?oz J;Epicolon consortium,de Bruyn M,Nijman HW,Novelli M,Lawson K,Oukrif D,Frangou E,Dutton P,Tejpar S,Delorenzi M,Kerr R,Kerr D,Tomlinson I,Church DN.Somatic POLE proofreading domain mutation,immune response,and prognosis in colorectal cancer:a retrospective,pooled biomarker study.
2016;1:207-216 [PMID:28404093 DOI:10.1016/S2468-1253(16)30014-0]
91 Rayner E,van Gool IC,Palles C,Kearsey SE,Bosse T,Tomlinson I,Church DN.A panoply of errors:polymerase proofreading domain mutations in cancer.
2016;16:71-81[PMID:26822575 DOI:10.1038/nrc.2015.12]
92 Shlien A,Campbell BB,de Borja R,Alexandrov LB,Merico D,Wedge D,Van Loo P,Tarpey PS,Coupland P,Behjati S,Pollett A,Lipman T,Heidari A,Deshmukh S,Avitzur N,Meier B,Gerstung M,Hong Y,Merino DM,Ramakrishna M,Remke M,Arnold R,Panigrahi GB,Thakkar NP,Hodel KP,Henninger EE,G?ksenin AY,Bakry D,Charames GS,Druker H,Lerner-Ellis J,Mistry M,Dvir R,Grant R,Elhasid R,Farah R,Taylor GP,Nathan PC,Alexander S,Ben-Shachar S,Ling SC,Gallinger S,Constantini S,Dirks P,Huang A,Scherer SW,Grundy RG,Durno C,Aronson M,Gartner A,Meyn MS,Taylor MD,Pursell ZF,Pearson CE,Malkin D,Futreal PA,Stratton MR,Bouffet E,Hawkins C,Campbell PJ,Tabori U;Biallelic Mismatch Repair Deficiency Consortium.Combined hereditary and somatic mutations of replication error repair genes result in rapid onset of ultra-hypermutated cancers.
2015;47:257-262 [PMID:25642631 DOI:10.1038/ng.3202]
93 Howitt BE,Shukla SA,Sholl LM,Ritterhouse LL,Watkins JC,Rodig S,Stover E,Strickland KC,D'Andrea AD,Wu CJ,Matulonis UA,Konstantinopoulos PA.Association of Polymerase e-Mutated and Microsatellite-Instable Endometrial Cancers With Neoantigen Load,Number of Tumor-Infiltrating Lymphocytes,and Expression of PD-1 and PD-L1.
2015;1:1319-1323[PMID:26181000 DOI:10.1001/jamaoncol.2015.2151]
94 McGranahan N,Furness AJ,Rosenthal R,Ramskov S,Lyngaa R,Saini SK,Jamal-Hanjani M,Wilson GA,Birkbak NJ,Hiley CT,Watkins TB,Shafi S,Murugaesu N,Mitter R,Akarca AU,Linares J,Marafioti T,Henry JY,Van Allen EM,Miao D,Schilling B,Schadendorf D,Garraway LA,Makarov V,Rizvi NA,Snyder A,Hellmann MD,Merghoub T,Wolchok JD,Shukla SA,Wu CJ,Peggs KS,Chan TA,Hadrup SR,Quezada SA,Swanton C.Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade.
2016;351:1463-1469[PMID:26940869 DOI:10.1126/science.aaf1490]
95 Yi M,Dong B,Chu Q,Wu K.Immune pressures drive the promoter hypermethylation of neoantigen genes.
2019;8:32 [PMID:31799063 DOI:10.1186/s40164-019-0156-7]
96 Ma W,Pham B,Li T.Cancer neoantigens as potential targets for immunotherapy.
2021;1-10 [PMID:33950415 DOI:10.1007/s10585-021-10091-1]
97 Li L,Yu R,Cai T,Chen Z,Lan M,Zou T,Wang B,Wang Q,Zhao Y,Cai Y.Effects of immune cells and cytokines on inflammation and immunosuppression in the tumor microenvironment.
2020;88:106939 [PMID:33182039 DOI:10.1016/j.intimp.2020.106939]
98 Minami S,Ihara S,Ikuta S,Komuta K.Gustave Roussy Immune Score and Royal Marsden Hospital Prognostic Score Are Biomarkers of Immune-Checkpoint Inhibitor for Non-Small Cell Lung Cancer.
2019;10:90-100 [PMID:31068989 DOI:10.14740/wjon1193]
99 Diem S,Kasenda B,Spain L,Martin-Liberal J,Marconcini R,Gore M,Larkin J.Serum lactate dehydrogenase as an early marker for outcome in patients treated with anti-PD-1 therapy in metastatic melanoma.
2016;114:256-261 [PMID:26794281 DOI:10.1038/bjc.2015.467]
100 Ameratunga M,Chénard-Poirier M,Moreno Candilejo I,Pedregal M,Lui A,Dolling D,Aversa C,Ingles Garces A,Ang JE,Banerji U,Kaye S,Gan H,Doger B,Moreno V,de Bono J,Lopez J.Neutrophil-lymphocyte ratio kinetics in patients with advanced solid tumours on phase I trials of PD-1/PD-L1 inhibitors.
2018;89:56-63 [PMID:29227818 DOI:10.1016/j.ejca.2017.11.012]
101 Jiang T,Qiao M,Zhao C,Li X,Gao G,Su C,Ren S,Zhou C.Pretreatment neutrophil-tolymphocyte ratio is associated with outcome of advanced-stage cancer patients treated with immunotherapy:a meta-analysis.
2018;67:713-727 [PMID:29423649 DOI:10.1007/s00262-018-2126-z]
102 Arenas-Ramirez N,Sahin D,Boyman O.Epigenetic mechanisms of tumor resistance to immunotherapy.
2018;75:4163-4176 [PMID:30140960 DOI:10.1007/s00018-018-2908-7]
103 Qamra A,Xing M,Padmanabhan N,Kwok JJT,Zhang S,Xu C,Leong YS,Lee Lim AP,Tang Q,Ooi WF,Suling Lin J,Nandi T,Yao X,Ong X,Lee M,Tay ST,Keng ATL,Gondo Santoso E,Ng CCY,Ng A,Jusakul A,Smoot D,Ashktorab H,Rha SY,Yeoh KG,Peng Yong W,Chow PKH,Chan WH,Ong HS,Soo KC,Kim KM,Wong WK,Rozen SG,Teh BT,Kappei D,Lee J,Connolly J,Tan P.Epigenomic Promoter Alterations Amplify Gene Isoform and Immunogenic Diversity in Gastric Adenocarcinoma.
2017;7:630-651 [PMID:28320776 DOI:10.1158/2159-8290.CD-16-1022]
104 Herbst RS,Soria JC,Kowanetz M,Fine GD,Hamid O,Gordon MS,Sosman JA,McDermott DF,Powderly JD,Gettinger SN,Kohrt HE,Horn L,Lawrence DP,Rost S,Leabman M,Xiao Y,Mokatrin A,Koeppen H,Hegde PS,Mellman I,Chen DS,Hodi FS.Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients.
2014;515:563-567 [PMID:25428504 DOI:10.1038/nature14011]
105 Wu HX,Chen YX,Wang ZX,Zhao Q,He MM,Wang YN,Wang F,Xu RH.Alteration in TET1 as potential biomarker for immune checkpoint blockade in multiple cancers.
2019;7:264 [PMID:31623662 DOI:10.1186/s40425-019-0737-3]
106 Perrier A,Didelot A,Laurent-Puig P,Blons H,Garinet S.Epigenetic Mechanisms of Resistance to Immune Checkpoint Inhibitors.
2020;10 [PMID:32708698 DOI:10.3390/biom10071061]
107 Fan J,Yin Z,Xu J,Wu F,Huang Q,Yang L,Jin Y,Yang G.Circulating microRNAs predict the response to anti-PD-1 therapy in non-small cell lung cancer.
2020;112:2063-2071[PMID:31786291 DOI:10.1016/j.ygeno.2019.11.019]
108 González-Silva L,Quevedo L,Varela I.Tumor Functional Heterogeneity Unraveled by scRNA-seq Technologies.
2020;6:13-19 [PMID:31952776 DOI:10.1016/j.trecan.2019.11.010]
109 Durante MA,Rodriguez DA,Kurtenbach S,Kuznetsov JN,Sanchez MI,Decatur CL,Snyder H,Feun LG,Livingstone AS,Harbour JW.Single-cell analysis reveals new evolutionary complexity in uveal melanoma.
2020;11:496 [PMID:31980621 DOI:10.1038/s41467-019-14256-1]
110 Mao X,Yang X,Chen X,Yu S,Zhang B,Ji Y,Chen Y,Ouyang Y,Luo W.Single-cell transcriptome analysis revealed the heterogeneity and microenvironment of gastrointestinal stromal tumors.
2021;112:1262-1274 [PMID:33393143 DOI:10.1111/cas.14795]
111 Di J,Liu M,Fan Y,Gao P,Wang Z,Jiang B,Su X.Phenotype molding of T cells in colorectal cancer by single-cell analysis.
2020;146:2281-2295 [PMID:31901134 DOI:10.1002/ijc.32856]
112 Zhou Y,Bian S,Zhou X,Cui Y,Wang W,Wen L,Guo L,Fu W,Tang F.Single-Cell Multiomics Sequencing Reveals Prevalent Genomic Alterations in Tumor Stromal Cells of Human Colorectal Cancer.
2020;38:818-828.e5 [PMID:33096021 DOI:10.1016/j.ccell.2020.09.015]
113 Lu Z,Chen H,Jiao X,Zhou W,Han W,Li S,Liu C,Gong J,Li J,Zhang X,Wang X,Peng Z,Qi C,Wang Z,Li Y,Brock M,Zhang H,Shen L.Prediction of immune checkpoint inhibition with immune oncology-related gene expression in gastrointestinal cancer using a machine learning classifier.
2020;8 [PMID:32792359 DOI:10.1136/jitc-2020-000631]
114 Conforti F,Pala L,Pagan E,Corti C,Bagnardi V,Queirolo P,Catania C,De Pas T,Giaccone G.Sex-based differences in response to anti-PD-1 or PD-L1 treatment in patients with non-small-cell lung cancer expressing high PD-L1 Levels.A systematic review and meta-analysis of randomized clinical trials.
2021;6:100251 [PMID:34455288 DOI:10.1016/j.esmoop.2021.100251]
115 Elias R,Karantanos T,Sira E,Hartshorn KL.Immunotherapy comes of age:Immune aging &checkpoint inhibitors.
2017;8:229-235 [PMID:28223073 DOI:10.1016/j.jgo.2017.02.001]
116 Manji G.Perioperative Chemo and Pembrolizumab in Gastric Cancer.[cited 8 September 2021].Available from:https://clinicaltrials.gov/ct2/show/NCT02918162
117 Ying L.Camrelizumab Combined with Apatinib for Advanced Gastric or Esophagogastric Adenocarcinoma [cited 8 September 2021].Available from:https://clinicaltrials.gov/ct2/show/NCT04948125
118 Park RS.Phase II Study of Neoadjuvant Immune Checkpoint Inhibitor in Patients with resectable Gastrointestinal Cancers (NeoChance).[cited 8 September 2021].Available from:ClinicalTrials.gov
119 Fate Therapeutics.FT500 as Monotherapy and in Combination With Immune Checkpoint Inhibitors in Subjects With Advanced Solid Tumors.[cited 8 September 2021].Available from:https://clinicaltrials.gov/ct2/show/NCT03841110
120 Incyte Corporations.Arginase Inhibitor INCB001158 as a Single Agent and in Combination with Immune Checkpoint Therapy in Patients With Advanced/Metastatic Solid Tumors.[cited 8 September 2021].Available from:https://clinicaltrials.gov/ct2/show/NCT02903914
121 Teclison Ltd.Combination of TATE and PD-1 Inhibitor in Liver Cancer (TATE-PD1) [cited 8 September 2021].Available from:https://clinicaltrials.gov/ct2/show/NCT03259867
122 Guangdong Provincial People's Hospital.A Real-World Study of Immune Checkpoint Inhibitors and Chemotherapy for Advanced Esophageal Cancer.[cited 8 September 2021].Available from:https://clinicaltrials.gov/ct2/show/NCT04822103
 World Journal of Gastrointestinal Oncology2022年1期
World Journal of Gastrointestinal Oncology2022年1期
- World Journal of Gastrointestinal Oncology的其它文章
- Comment on “Outcomes of curative liver resection for hepatocellular carcinoma in patients with cirrhosis”
- Liquid biopsy:Precise diagnosis and therapy for cholangiocarcinoma
- Increased risk of colorectal neoplasia in inflammatory bowel disease patients with post-inflammatory polyps:A systematic review and meta-analysis
- Exosomes as potential diagnosis and treatment for liver cancer
- Effects of cognitive behavior therapy combined with Baduanjin in patients with colorectal cancer
- Intertwined leukocyte balances in tumours and peripheral blood as robust predictors of right and left colorectal cancer survival