
Applications of dynamic visual acuity test in clinical ophthalmology
2021-11-30 04:48:00TingYiWuYueXinWangXueMinLi
Ting-Yi Wu, Yue-Xin Wang, Xue-Min Li
1Department of Ophthalmology, Peking University Third Hospital, Beijing 100191, China
2Beijing Key Laboratory of Restoration of Damaged Ocular Nerve, Peking University Third Hospital, Beijing 100191, China
Abstract
KEYWORDS: dynamic visual acuity test; cataract;dizziness; optic neuritis; glaucoma
INTRODUCTION
Dynamic visual acuity (DVA) is defined as the ability to identify the details of visual targets when there are relative movements between the subjects and objects[1]. In our daily lives, we need to observe different kinds of objects among which moving ones make up the majority. Therefore,DVA has a close relationship with our lives. Besides, there are differences between factors influencing dynamic visual signals and static ones, as well as their neural conduction pathways.According to the two-streams hypothesis, the static visual system is traditionally segregated into two main processing streams, one the dorsal ‘where’ pathway which is responsible for processing spatial location information and finally reaches the posterior parietal lobe, the other the ventral ‘what’pathway which is responsible for processing objects’ quality information and terminates in the inferior temporal lobe[2-5].Visual motion information flows parallelly from primary visual cortical (V1) direction-selective neurons, pulvinar neurons that receive afferent signals from the superior colliculus, and lateral geniculate nucleus (LGN) neurons into middle-temporal MT/V5 area[6-9]. MT/V5 is a motion-sensitive region which has an essential role in visuomotor transformations[10]. In terms of the diverse function of different brain regions, the ascending motion signals processed by MT/V5 are transferred directly orviathe MST complex, which is adjacent to MT/V5, to various functional areas[11-12]. For example, information related to biological motion (i.e., the perception of moving organisms) is projected to posterior superior temporal sulcus (pSTS) and ventral premotor cortex (vPMC)[13-15], and information associated with radial motion, eye movements generation and allocation of spatial attention towards the contralateral visual hemifield is projected to frontal eye fields (FEF)[16-18], while optic flow to V6 area[19-20], so that we can perceive multiple kinds of moving objects. Due to the separate conduction pathway, the significance of the DVA test (DVAT) and static visual acuity test (SVAT) in evaluating ocular disorders will also be different. Therefore, it is crucial to evaluate DVA in the clinical settings and we are confined to assess patients’ static visual acuity (SVA) at present. This review mainly introduces the DVATs commonly used and their applications in clinical ophthalmology.
DYNAMIC VISUAL ACUITY TESTS
Commonly used DVATs can be classified into DVATs with static optotypes, DVATs with moving optotypes and motion perception behavior tests. DVATs with static optotypes generally include subjects moving their heads volitionally and passively, which are mainly used to evaluate vestibulo-ocular reflex (VOR). DVATs with moving optotypes demonstrate optotypes mechanically or with a computer monitor, and are mainly used to evaluate dynamic visual function. Motion perception behavior tests can be divided into the object from motion (OFM) protocol and random dot kinematograms(RDKs) applied to assess the brain’s perceptual ability on moving visual targets.
Dynamic Visual Acuity Tests with Static Optotypes Volitionally head moving
1) Speed unsupervisedParticipants are instructed to oscillate their heads volitionally in the horizontal plane without speed supervision and identify the standard Snellen chart ahead at the same time[21]. DVA is determined by the smallest letter that can be recognized. The oscillatory frequency used should be at least 2 Hz to preclude the influential eye movements such as the smooth pursuit[22-24]. Although speed unsupervised test is convenient, the velocity and frequency of oscillation depend on the participants themselves, which makes it impossible to maintain the stable oscillation. Moreover, participants may be able to use non-VOR methods such as saccade to recognize optotypes at the instant of changing oscillate direction[23-24].
2) Speed supervisedParticipants are instructed to oscillate their heads volitionally in the horizontal plane with rotation sensors installed to their heads, taking VSR? SPORT for an example (Figure 1)[23-25]. The sensor will detect the velocity of the head movement. A Snellen E optotype will be demonstrated (less than 85 ms) on the computer screen as the velocity of head-rotation reaches the pre-set threshold. This method stipulates and monitors the moving speed making the results more accurate and the test repeatable, but the velocity and frequency of oscillation are still under participants’control[23-24].
Passive head movingParticipants sit on an electric rotary chair, which can turn at a particular speed and frequency,and identify the optotypes on the screen in the front at the same time with their heads fixed to the chair. The rotary chair can control the movement precisely which is in favor of clinical trials. However, it is not commonly used due to the requirement of specific apparatuses and large space[23,26-27].
Dynamic Visual Acuity Tests with Moving Optotypes
Mechanical moving optotypes demonstrationThe application of mechanical moving optotypes demonstration is closer to the real world compared with digital demonstration,and the test is not affected by the refresh rate and response time of the monitor. However, specific types of equipment are required to perform the mechanical demonstration.
The test system with a moving loading device places the standard optotypes, made according to the logMAR chart,on a mobile model cart (Figure 2). The cart carries multiple optotypes representing different visual acuity at the same time in descending order from left to right. The cart could move towards a certain direction at a particular speed. Participants are instructed to identify optotypes from left to right with their heads static and the result is defined as the smallest optotype identified correctly[28].
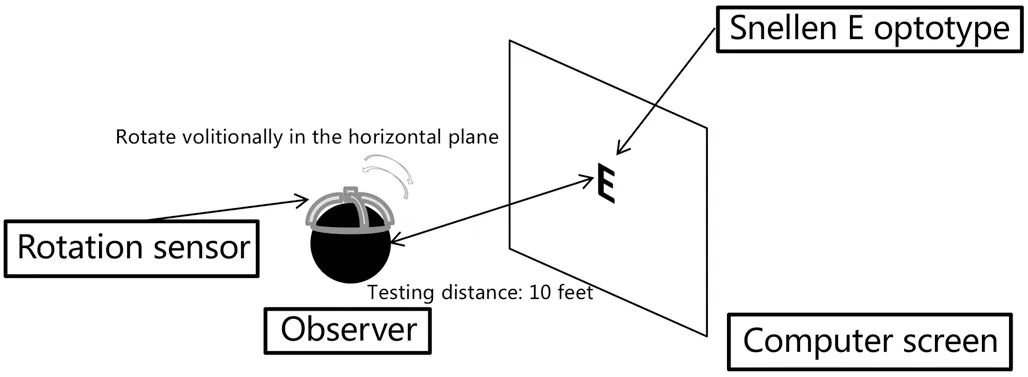
Figure 1 Speed supervised static optotypes DVAT Participants rotate their heads volitionally in the horizontal plane and identify the Snellen E optotype shown on the screen at the same time. A rotation sensor is installed on their heads for speed supervision. The testing distance is set at 10 feet.
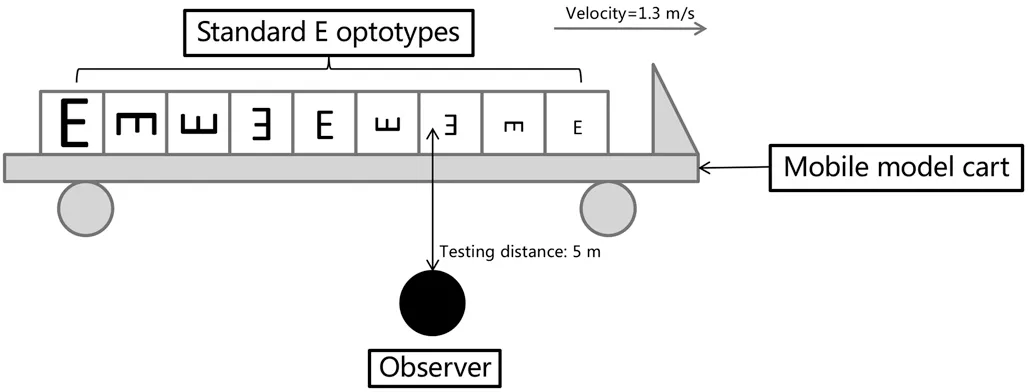
Figure 2 Direct mechanical moving optotypes demonstration DVAT A mobile cart carries standard E optotypes with the size arranged in descending order from left to right. The velocity of the cart is set at 1.3 m/s and the testing distance is set at 5 m.
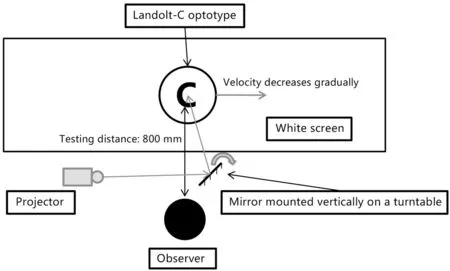
Figure 3 KOWA HI-10 system A projector projects a Landolt C optotype onto a mirror which is subsequently reflected onto a white screen. The mirror is mounted on a turntable motor. The optotype moves from left to right horizontally with certain velocity achieved through the spinning of the motor. The testing distance is set at 800 mm.
The test system with indirect mechanical moving optotypes demonstration such as KOWA HI-10 (Kowa Company, Ltd.,Japan) system (Figure 3) is also applied. The system applies a mirror mounted vertically on a turntable controlled by a speed motor. A Landolt-C optotype is projected onto the mirror by a projector and then reflected from the mirror onto a screen.The optotype moves from left to right horizontally at variable velocities, which is achieved through the spinning of the turntable. Optotype velocity is set to decrease gradually and the DVA is verified as the maximum speed at the first correctly recognition of the gap on the optotype[29-31].
Digital moving optotypes demonstrationA computer program is established to generate dynamic optotypes in different sizes, speeds, and movement patterns, which are directly demonstrated on a screen in front of the participants by a projector or data cable. Record the smallest optotype that can be identified at a particular speed,e.g., COI-SV software(Centro de Optometría Internacional, Spain), XP.14-TD-J905 DVA tester (Shanghai hump automatization technology co.,Ltd., China), and moV& software (University of Waterloo School of Optometry, Canada) or the maximum speed identifying optotypes at a specific size,e.g., moV& software(University of Waterloo School of Optometry, Canada)[32-37].Our team has developed a novel standardized DVA evaluation system with a testing program and procedures. The program is designed to display logMAR optotypes at a particular speed and size on the screen according to the parameter we enter.We also normalize the procedure of DVAT according to the standard SVAT. The procedure of the testing is similar to SVAT which is convenient and rapid that could be widely applied in clinical settings[32-33].
Motion Perception Behavior Tests
Object from motion protocolA computer program is used to generate a series of dots which contains a camouflaged pattern,e.g., star, umbrella, and wine glass (Figure 4). The dots within and outside the pattern are programmed to move towards opposite directions. The faster these dots move, the easier for participants to identify the pattern. The score is calculated according to the velocity requires to recognize the pattern[38-40].
Random dot kinematogramsRDKs (Figure 5), which include translational motion stimulus test, radial flow stimulus test and biological motion stimulus test, are composed of a series of white dots with a diameter of 0.1° on a black background. These dots contain signal dots and noise dots. A program is designed to move these dots in different patterns to detect various motion perception impairment[4,41-42]. The two-alternative-forced-choice-paradigms are used to discover the differences between contra- and ipsi-lesional visual hemifields. Participants are instructed to focus on the fixation dot at the center of the screen with their heads stabilized. They are required to choose the side containing signal dots or the focus of expansion (FOE). Signal intensity is defined as the percentage of signal dots relative to the total number of dots.The results are recorded according to the minimum signal intensity required to identify the circle containing signal dots or the FOE. Currently, we haven’t fully understood how human brains deal with various types of dynamic visual signals. Thus,the motion perception impairment identified by RDKs may not be able to correspond to a specific kind of lesion in the brain accurately[41].
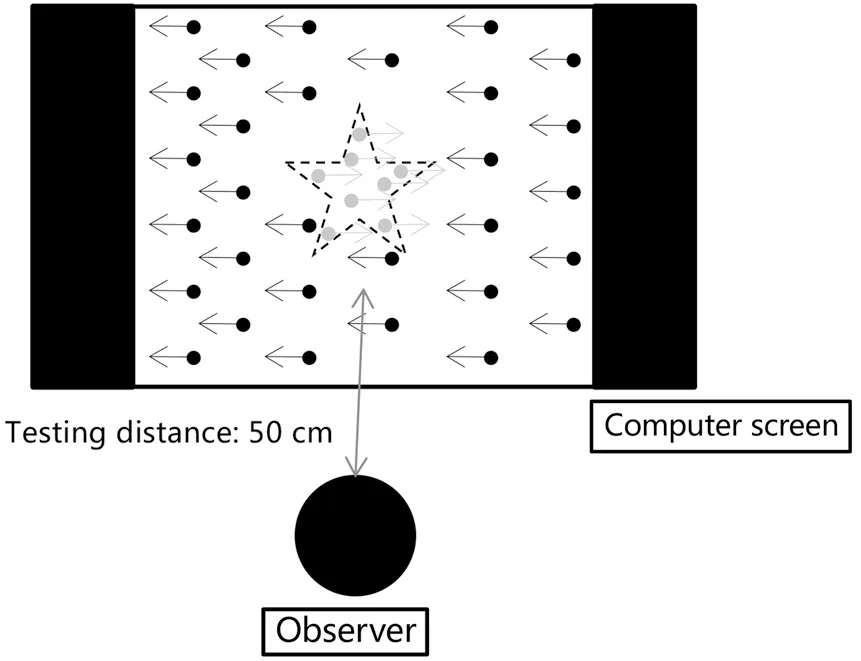
Figure 4 OFM protocol A series of dots contains a camouflaged pattern are demonstrated. The dots within and outside the pattern are programmed to move towards opposite directions. All dots are black in actual protocol and the grey dots were shown for clarification in the figure. Arrows are indications of moving direction.
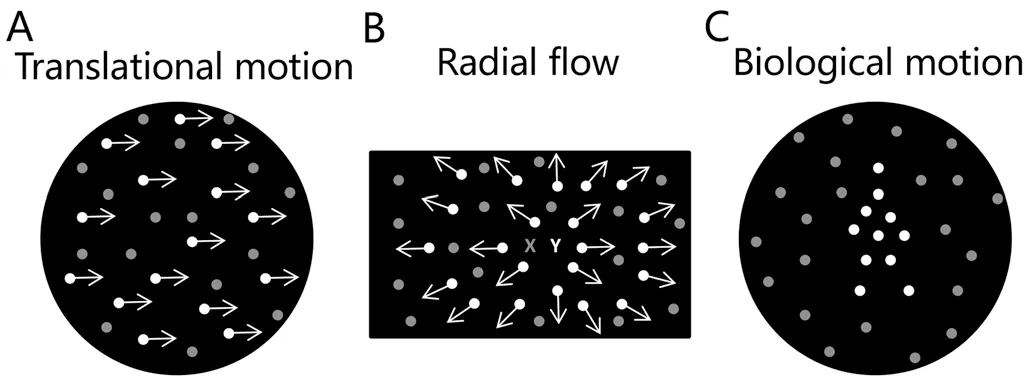
Figure 5 RDKs All dots are white in the actual test and the grey dots were shown for clarification in the figure. A: Translational motion stimulus test. Signal dots present in a coherent motion towards the same horizontal direction against the background of noise dots moving randomly. Arrows indicate the motion direction of the signal dots. B: Radial flow stimulus test. Signal dots expand coherently from the FOE (Y) while the noise dots move in random directions. X represents the fixation dot. Arrows indicate the motion direction of the signal dots. C: Biological motion stimulus test. Signal dots constitute the shape of a walker moving at a certain pace while the noise dots move in random directions.
1) Translational motion stimulus testThe stimulus is presented in a circular black background with a diameter of 9.4° containing 60 dots. Signal dots move towards the same horizontal direction at a speed of 6.6°/s, resulting in coherent motion. Noise dots move towards random directions.Participants are ordered to observe the two optotypes (black background circles with dots inside) appearing simultaneously right and left of the fixation dot, and identify the circle with signal dots[41].
2) Radial flow stimulus testThe stimulus is presented in a rectangular black background (37.5°×28.5°) containing 100 dots. Signal dots expand coherently from the FOE while the noise dots move in random directions. The velocity of expansion increases linearly from the FOE to the maximum of 18.6°/s in the periphery. Participants are instructed to identify whether the location of FOE is on the left or right of the central fixation point[41].
3) Biological motion stimulus testThe stimulus is presented in a circular black background with a diameter of 9.4°containing 11 signal dots which constitute the shape of a walker. The walker subtends a visual angle of 5.3° in height and 2.0° in width. The walking cycle is set to 1s. Noise dots move towards random directions. Participants are required to observe the two circles appearing simultaneously right and left of the fixation dot. One circle contains the walker. In the other one, these 11 dots move with the same mode but their spatial position is randomized within the circle so that the figure of a walker is lost[41].
APPLICATIONS OF DVAT IN CLINICAL OPHTHALMOLOGY
CataractCataract is a prevalent ocular disorder leading to vision loss. Phacoemulsification combined with intraocular lens (IOL) implantation surgery is a standard method to treat cataract[33]. As surgical techniques and IOL designs have improved a lot, cataract surgery mainly focuses on improving patients’ quality of life now[43-44]. Traditional SVAT and contrast sensitivity are commonly used to assess the visual function after cataract surgery at present, which only reflect static visual function. Since dynamic objects compose the majority of visual signals in our lives and there is an increasing number of patients who expect to drive or exercise after surgery, DVAT should be included in the cataract evaluation system[28,33,45].
Currently, DVATs with moving optotypes are used to assess patients with cataract[28,32-33,45]. Zhanget al[28]and Wanget al[45]used mechanical and digital optotypes demonstration respectively to evaluate DVA. Zhanget al[28]applied standard logarithmic E optotypes, and the velocity of the loading model cart was set at 1.3 m/s. Participants were instructed to identify the optotypes on the mobile loading cart at a distance of 5 m.Wanget al[45]projected the dynamic logarithmic E optotypes onto the screen at the horizontal moving speed of 15, 30, 60 and 90 degrees per second (dps), and tested at a distance of 4 m. These two studies revealed that the DVA of cataract patients significantly improved after the surgery with IOL implantation.Wanget al[45]also compared the DVA after surgery with the normal population, and the result showed no statistically significant difference. Our team applied a self-developed DVAT system and tested 30 elderly volunteers without cataract and 26 age-related cataract patients[32]. The result indicated that postoperative DVA of 15, 30, 60 and 90 dps significantly improved and there was no significant difference when compared to the control group[32]. Furthermore, we compared the DVA following implantation of trifocal with monofocal IOL. The result demonstrated that patients who implanted trifocal IOL obtained significantly better postoperative DVA as compared with monofocal IOL at the velocity of 15, 30,60, and 90 dps. Meanwhile, DVA was significantly correlated with distance, intermediate and near SVA postoperatively, and the multiple linear regression revealed that intermediate visual acuity made an increasing contribution to DVA as the velocity increased, which indicated that a continuous range of vision was paramount to DVA[46].
It has been identified that moving of the visual targets will produce artifact at the margin of their images on the retina which is termed as a retinal smear. The extent of retinal smear increases with the velocity increasing[47]. The opaque lens in cataract patients will scatter the light resulting in a blurry image on the retina, and moving of the visual targets will make the image more blurry under the influence of marginal artifacts[32,45,47].
All of the studies above show that dynamic visual signals significantly impact on age-related cataract patients. After phacoemulsification combined with IOL implantation surgery,DVA can improve remarkably. DVAT has feasibility and validity in assessing visual function after cataract surgery, and it has a greater advantage than traditional SVAT on evaluating the visual experience during driving and exercising[28,32,45,48].
Differentiation Diagnosis of DizzinessPatients with complaints of asthenopia are often complicated with dizziness,which might be caused by vestibular disorders or ocular disorders such as convergence insufficiency[49]. As patients are not able to express symptoms including vertigo, disequilibrium,syncope, lightheadedness, and asthenopia accurately, the differential diagnosis of dizziness is of significance for these patients and DVAT could facilitate the distinguishment of the causes[50-51].
VOR is an important physiological reflex to stabilize the retinal image during head moving[52]. Eyes are rotated automatically and precisely towards the opposite direction to compensate for the movements of heads, which fixes the image of visual targets onto the fovea continuously[52]. Patients with vestibular dysfunction often complain of oscillopsia and dizziness with decreased DVA due to an increased slip of image on the retina during head movements[26].
Shippmanet al[51]enrolled 10 participants complaining dizziness without vertigo, and they developed oscillopsia and dizziness after near work for a long time due to their convergence insufficiency. The participants were examined with static-optotype DVAT without head-rotation speed supervision. The result showed that none of these participants had a decrease in DVA, which was defined as three or more lines inferior to SVA. A retrospective cross-sectional research,including 323 cases, was conducted by Wanget al[53]with speed unsupervised static-optotype DVAT. The 113 of the cases showed impaired DVA, among which 109 cases were confirmed as having compromised VOR. Schubertet al[54]investigated 5 patients who had vestibular hypofunction. Their static-optotype DVA significantly improved after vestibular rehabilitation training. All of these trials reveal that DVAT can be used to differentiate dizziness in clinical settings. The patients with significantly impaired static-optotype DVA might indicate vestibular disorders that should be referred to otolaryngologists for further tests[51].
Optic NeuritisMultiple sclerosis (MS) is a chronic, acquired,immune-mediated inflammatory disorder involving optic nerves[55], and optic neuritis (ON) is one of the most common clinical features in MS that results in acute visual acuity decrease[56].
Currently, visual evoked potentials (VEPs), which could identify the demyelination of optic nerves, are often performed for the diagnosis of ON[39,57]. The VEP of typical ON in MS characteristically demonstrates latency of P100[58], and this prolongation may persist for years even after the recovery of visual function[39,59]. In addition to VEP, the demyelination of optic nerves causing reduced projection rate along the visual pathways might also be detected by DVAT[39].
Razet al[39]tested the DVA of 16 unilateral ON patients using OFM protocol. During the test, participants are required to recognize 20 stimuli successively. Each of these was first presented at the lowest velocity of 4 pixels/s, and the velocity gradually increased if the participant was not able to identify.The final score was a sum of 20 patterns according to the velocity participant required to identify them. The result indicated that the affected eyes of ON patients obtained significantly lower OFM scores when compared to normal eyes and patients’ fellow eyes. Impaired scores were also found 12mo following the attack. VEP was applied to each participant simultaneously and the OFM scores were found to be positively correlated with VEP (P100) latency values.
As compared with SVAT, DVAT may be more appropriate to quantify projection latencies caused by demyelination,because the generation of DVA requires sufficient amount and velocity of visual input projection, while SVA only depends on the amount[39,60]. In comparison with VEPs, the application of OFM favors the cost-effectiveness due to the lower cost. It does not require a trained technician as well and can be used by all clinical doctors. Therefore, OFM protocol can facilitate the diagnosis of ON patients, and evaluate not only the latency extent of neural projection rate but also the rehabilitation of optic nerves[39].
GlaucomaGlaucoma is one of the leading causes of irreversible blindness, characterized by progressive degeneration and death of retinal ganglion cells. Due to the effect of transsynaptic degenerations, glaucoma causes damages to the optic nerves as well as the post-retinal intracranial visual systems such as LGN neurons[61]. Thus, it’s critical to detect glaucomatous optic nerve damage in early stages[62-64].
The human LGN receives direct visual signals input from the retina and then project them to the visual center in occipital lobe[65]. The LGN is mainly made up of six layers including magnocellular layers (M layers) and parvocellular layers (P layers). M neurons are primarily related to the perception of moving visual signals, such as the alteration of velocity and position, and other sudden visual changes occurring at large spatial scales. P neurons mainly involve the analysis of objects’ appearance information[66-67]. During the progression of glaucoma, different neurons of the LGN might be differentially involved. Previous studies on the primate model of experimental glaucoma and the human autopsy revealed that M layers were more vulnerable to glaucomatous damage, comparing to P layers[68-69]. Zhanget al[65]compared signal differences of LGN neurons between early-stage openangle glaucoma patients and normal subjects with functional magnetic resonance imaging (fMRI). The result indicated that signals from M layers were selectively loss in early glaucoma patients and the loss was significantly correlated with the degree of functional deficits to the glaucomatous eye.Currently, isolated-check visual evoked potential (ic-VEP) is applied to evaluate early-stage glaucoma. Using low contrast stimulus, ic-VEP can detect M pathway relatively specifically.Fanet al[70]reported that the signal-to-noise ratio (SNR)significantly reduced (≤1) in early glaucoma patients with 15% contrast optotypes using ic-VEP. All of these researches implied that M neurons are more seriously injured in earlystage glaucoma. Previous research demonstrated that M pathway mainly transferred visual signals which were made up of low spatial frequencies and high temporal frequencies.As temporal frequencies increased, the percentage contribution to signal conduction from M cells increased[71]. Therefore, M pathway is primarily responsible for the conduction of visual signals in motion which provides a theoretical basis for using DVAT to assess early-stage glaucoma. Wenet al[62]investigated the function of contrast sensitivity in preperimetric glaucoma patients by using interference fringe optotypes which were in high temporal frequency. The result showed that there was a loss of contrast sensitivity in the peripheral visual field in preperimetric glaucoma patients, and this also corresponds to the selective damage in M pathway, as M neurons mainly function under high temporal frequency. Therefore, the moving-optotypes DVAT using high temporal frequency optotypes has potential clinical value in the earlier detection of functional defects in glaucoma. However, there are no reports of using dynamic optotypes to evaluate early-stage glaucoma at present, and this requires further research.
CONCLUSION
At present, DVAT is still mainly applied to investigate vestibular function in otolaryngology and the visual functions of elite athletes as well as drivers’ driving safety[72-73]. The clinical trials mentioned in this review demonstrate that DVAT has its unique clinical significance in understanding various ocular diseases and the influence of surgery to visual function in real lives comprehensively, differentiating ocular disorders and vestibular dysfunction, and offering an earlier diagnosis of some ophthalmic diseases. DVAT can provide a good supplement for the tests traditionally used in clinical ophthalmology, such as SVAT, contrast sensitivity and visual field. Problems, including the lack of criteria and application indication, still exist currently. Moreover, the exact relationship between DVA and other visual functions remains unclear.Further research still needs to uncover the significance of DVAT and explore its application in clinical ophthalmology.
ACKNOWLEDGEMENTS
Foundations:Supported by Chinese Capital’s Funds for Health Improvement and Research (No.CFH2018-2-4093); National Science and Technology Major Project(No.2018ZX10101-004).
Conflicts of Interest: Wu TY,None;Wang YX,None;Li XM,None.
 International Journal of Ophthalmology2021年11期
International Journal of Ophthalmology2021年11期
- International Journal of Ophthalmology的其它文章
- Toric implantable collamer lens for the management of pseudophakic anisometropia and astigmatism
- Angle-closure glaucoma with attenuated mucopolysaccharidosis type l in a Chinese family
- Novel biallelic compound heterozygous mutations in FDXR cause optic atrophy in a young female patient: a case report
- A novel temporary keratoprosthesis technique for vitreoretinal surgery
- Human umbilical cord-derived mesenchymal stem cells treatment for refractory uveitis: a case series
- lntroduction of longstanding complicated sulcus intraocular lens into the intact capsular bag