
Challenges confronting rural hospitals accentuated during COVID-19
2021-01-13 07:12:12AnthonySlonimHelenSeeSheilaSlonim
Anthony D. Slonim, Helen See, Sheila Slonim
1Renown Health, Reno, NV 89503, USA;2Medicine and Pediatrics, University of Nevada, Reno School of Medicine, Reno, NV 89557, USA;3Hospital Operations, Carilion Clinic, Roanoke, VA 24017, USA.
Abstract The Balanced Budget Act of 1997 created a designation for critical access hospitals (CAHs) to sustain care for people living in rural communities who lacked access to care due to hospital closures over the preceding decade.Twenty-five years later, 1350 CAHs serve approximately 18% of the US population and a systematic policy evaluation has yet to be performed. This policy analysis serves to define challenges faced by CAHs through a literature review addressing the four major categories of payment, quality, access to capital, and workforce.Additionally, this analysis describes how current challenges to maintain sustainability of CAHs over time are accentuated by gaps in public health infrastructure and variability in individual health care plans exhibited during the COVID-19 pandemic.
Keywords: rural hospitals, critical access hospitals, COVID-19, coronavirus
Introduction
The United States (US) population is broadly distributed throughout the nation. Healthcare delivery for people who live in rural environments has been challenged for many years. Despite numerous legislative efforts to improve this care over decades,rural healthcare providers continue to face unique and important challenges that in many ways jeopardize the service offerings to those populations from access,cost and quality perspectives.
SARS-CoV-2, the novel coronavirus that has caused the coronavirus disease 2019 (COVID-19)pandemic presents challenges facing providers in rural America and can have devastating and permanent effects on the healthcare received by people who live there. This analysis will seek to improve our understanding of the important role of a significant component of rural healthcare, namely the critical access hospitals (CAHs), to determine the challenges to ongoing care facing these hospitals, and to identify potential solutions that can help them continue to be viable as they wrestle with the COVID-19 pandemic.
COVID-19 pandemic
The COVID-19 pandemic is a global infectious disease crisis that began in Wuhan, China in late 2019.The clinical syndrome, caused by a novel coronavirus,is characterized by a variety of clinical symptoms,which initially seemed to have a predisposition for the elderly and those with underlying chronic conditions.As the pandemic evolved, additional subgroups were affected including children who displayed a generalized inflammatory condition. The syndrome is characterized by high infectivity, abnormalities in organ function and clotting, and significant mortality.Of importance, the virus is transmitted through asymptomatic carriers who can infect others without their knowledge. To date, there is no vaccine or widely available treatment. The best, currently available defenses include broad based public health prevention strategies like masking, social distancing and hand washing. Other public health interventions like population based screening using testing and contact tracing have failed because of a lack of resources.
What does it mean to be "rural"?
Using clear and objective parameters in defining rurality is important for informing analyses.Unfortunately, confusion on this topic has existed for some time with definitions that remain unclear and are based broadly on two prevailing definitions, one from the Census Bureau, which tends to overestimate the population and land in the rural environment, and one from the Office of Management and Budget, which tends to underestimate the rural population and land area. Using these two baseline definitions, the Federal Office of Rural Health Policy (FORHP) has adapted their own approach for defining rural counties for the purpose of healthcare services based on the Goldsmith modification[1](Fig. 1). FORHP has coordinated activities related to rural health care within the U.S.Department of Health and Human Services (HHS) for the past 30 years.
The FORHP considers all non-metropolitan counties as rural and goes further by using codes known as the Rural-Urban Commuting Area (RUCA)codes. These codes are based on census data and classify each census tract with a code. There are>70 000 census tracts in the US and any census tracts classified as 4 to 10 using this method qualifies as rural. This approach also provides for the classification of rural tracts within metropolitan areas since some of these are very large tracts of land with very small populations. With this approach,approximately 57 million people are within rural tracts accounting for 18% of the population and 84% of the land area (Fig. 1).
Serving the healthcare needs of people who live in rural environments
Given the substantial proportion of the US population that live in the rural environment and the special and unique circumstances for serving the healthcare needs of these people, several important programs have evolved, and designations have emerged[3](Table 1). While each of these has a place in the rural environment, the emphasis for this analysis will be on the first designation known as the CAH and their enduring presence nearly 25 years after their initiation (Fig. 1).
The CAHs were created by the Balanced Budget Act of 1997 as one approach to deal with the increased number of rural hospital closings in the preceding decade. Today, there are approximately 1350 CAHs providing rural care in the US (Fig. 1). The designation of CAH comes from meeting several important criteria for size, distance from other facilities and mechanisms of payment (Table 1).Despite these important designations, which aim to preserve the role of the CAH as a safety net provider of services for those in the rural environment, there were ongoing challenges that affected these hospitals long before the COVID-19 pandemic and raise important questions about their viability in the current healthcare landscape.
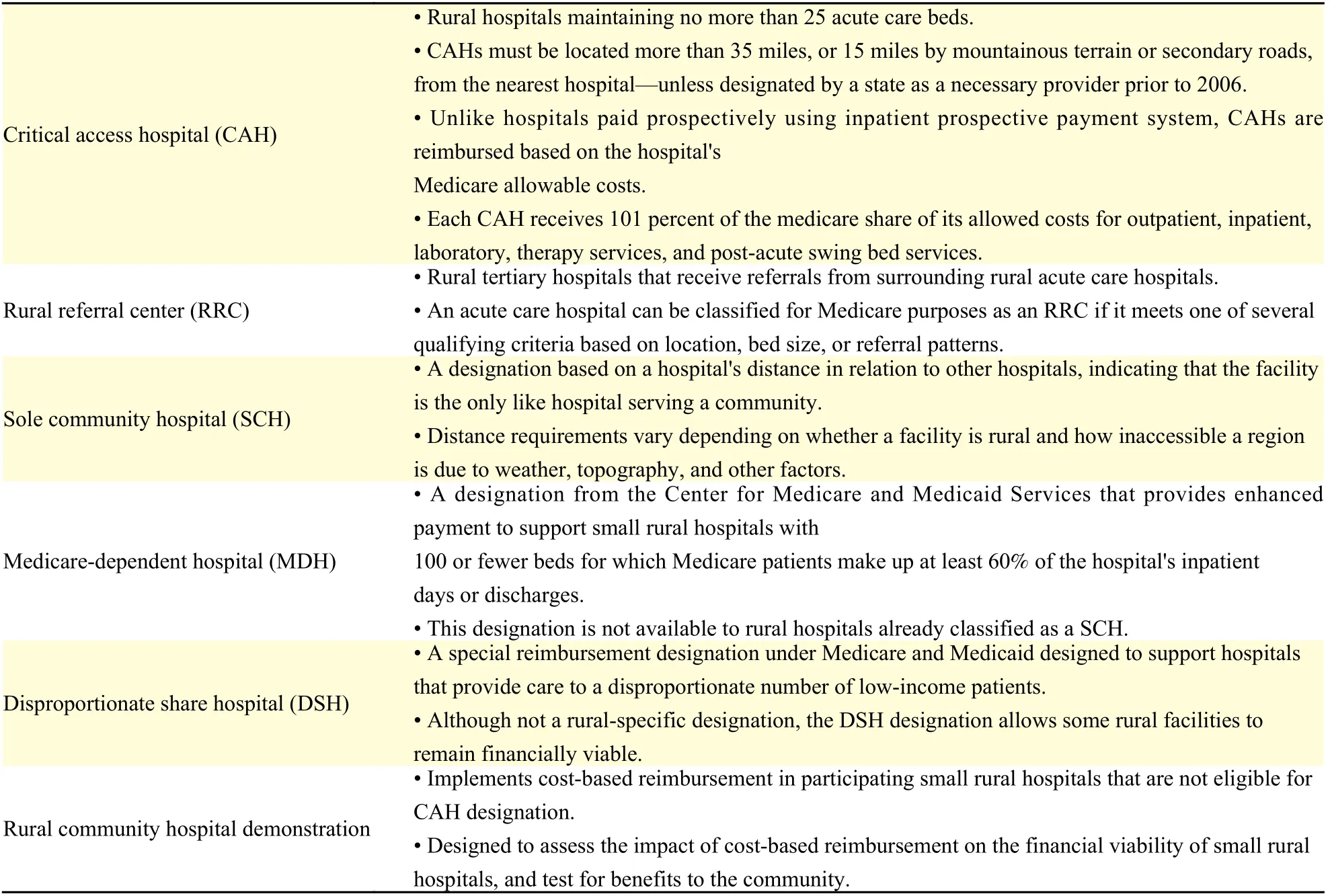
Table 1 Rural hospital designations and provider types
Four challenges faced by CAHs
The American Hospital Association (AHA) drew attention to some of the more recent threats to rural healthcare viability, which are layered on the consistent challenges plaguing providers in the rural environment[4]. These issues are particularly relevant for CAHs and become accentuated for those CAHs challenged by COVID-19 because they affect the ability of these hospitals to respond effectively to the pandemic[4](Fig. 2). While some of the traditional challenges for CAHs include managing the opioid epidemic, access to capital and broadband, and mechanisms to combat cyber threats[4]there are several threats that continue to plague CAHs on a more consistent basis and have been around for many years (Fig. 2). These include the following categories of payment challenges, workforce challenges,challenges to quality, and access to capital. These four challenges help to define a state of impending chaos for rural providers and some would argue jeopardize the long-term viability of these organizations and their ability to provide access to important healthcare services at CAHs in the rural environment even before the pandemic started.
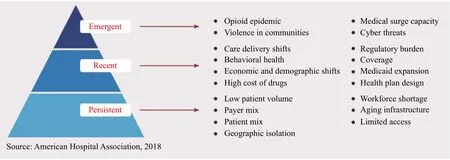
Fig. 2 Persistent, recent, and emergent challenges facing rural communities[4].
Methodologic approach to synthesizing the literature
Using PubMed, the literature was reviewed for how CAHs were operative across the four major challenge areas of payment, workforce, quality and access to capital. While CAHs are an important component of rural hospitals and healthcare, only results that included CAHs specifically were included. Sequential searches were performed that investigated the following combinations of key words: "critical access hospitals" and "payment"; "critical access hospitals"and "workforce"; "critical access hospitals" and"quality"; "critical access hospitals" and "capital".From the results obtained in these searches, a manual review that looked at all articles published from January 2009 to June 2020 were investigated.
The search was inclusive of peer-reviewed articles,discussion articles, and commentaries published in the United States. Articles that met the appropriate inclusion criteria were selected and the full text of the article was downloaded for further review. For the most part, while single state or institution articles were included in a first level review, they were not included as a part of the final literature review if their findings were not applicable to a broader context beyond that state.
Literature synthesis for non-COVID challenges to CAHs
Payment challenges prior to COVID-19
Among the many challenges facing CAHs, one of the most important is payment and financial performance. The CAHs are paid on a cost-based reimbursement and not on the prospective payment system (PPS). As detailed above, there are specific criteria to obtain a CAH designation, not the least of which is distance from another acute care facility, but the same criteria that assist in designating a CAH may in turn affect its financial performance because of its rural location.
There is considerable variability and sometimes contradictory data in the literature related to payments to CAHs and how well they are performing. For example, while some believe that the CAH designation and distancing requirements are essential for the survival of the CAHs[5]others believe that the distances and special treatment provided to preserve CAHs have led to less efficient and costlier care overall in these CAHs[6–8]. Reiter and colleagues found that Medicare reimbursement of swing beds in CAHs was approximately $300 higher than swing bed costs in non-CAHs, but rationalized that this was still a less expensive alternative than the $1300 per diem rate that would have alternatively been charged. Holmes and colleagues in a study using the Healthcare Cost and Reporting Information System over a period of six years evaluated a variety of financial performance measures describing profitability, liquidity, capital structure, and financial strength found that CAHs performed better on all of these measures after controlling for hospital, market and reimbursement characteristics[8]. These authors also performed a number of simulations to determine if CAHs would maintain financial viability under a PPS and found that universally financial performance in CAHs would be worse under PPS[8].
In addition, there is a fair amount of controversy for those CAHs that are a part of a large health system that disproportionately receive cost allocation from the system to the CAH may inappropriately be affecting the financial performance of the CAH by cost shifting and preserving the performance of the system overall[9–10].
Workforce challenges prior to COVID-19
The CAHs are by definition working in a context that is constrained. The literature around workforce constraints in CAHs is limited and more often composed of case studies and examples from individual hospitals, groups of hospitals or local regions that highlight both the problems of workforce in this setting and some potential local solutions that have been tested and appear to work.
The literature is clear that limitations in workforce are not isolated to a specific discipline. Clinical providers of all disciplines, including nurses,pharmacists, physicians, and mid-level providers, like physician assistants and nurse practitioners, are difficult to recruit and retain[11–16]. Among the reasons listed as challenging for recruitment, include the need to feel connected to colleagues in more urban settings so that skills can be maintained[11,13,14]. In addition,there was a clear need to assure that recruits had ample support financially, with adequate time off, and supported in a network of other providers[12,13,17].
When CAHs identified shortfalls in workforce,there were a number of creative mechanisms designed to augment that discipline. For example, the offering of medical students of a rural health rotation was designed to augment the physician workforce at one CAH[11]. In an effort to maintain the quality of surgical efforts by one CAH surgeon, he performed all the pre and post-operative care himself rather than sending patients back to a primary care group with little surgical experience[18]. Using mid-level providers has become an important mechanism for addressing the health and healthcare needs in CAHs and in the rural setting more broadly[13,15,18]. In addition to the traditional extenders like nurse practitioners and physician assistants, pharmacy extenders have become an important group that can expand the reach of some primary care and specialty physicians[12,16].
A consistent theme for CAHs was not only finding workforce, but also finding a skilled workforce that could maintain their skills in a low volume setting over time. In this respect, the literature was varied.There were case examples of some excellent care like the CAH whose nurses committed to obtaining Magnet designation[19]. In addition, a group of pharmacists covering seven CAHs significantly and in concert reduced their hospitals' formularies to both streamline the medications reducing the inventory and aligning so that borrowing medications from each other in times of shortage would be easier[16].
Despite these examples of excellent care, there are concerns that the workforce in CAHs may not be as skilled as you would expect. This will be discussed further under the next section on quality. However,Undurraga and colleagues highlight that a traditional surgical residency may not provide sufficient case mix for the procedures that need to be performed in the rural environment[20]. Similar issues with continuing education were identified in many disciplines and highlight the need for partnership and ongoing rotations with larger volume centers[17–18]. In addition,a skilled workforce needs the tools and equipment to effectively perform their work. DesRoches and colleagues highlight how CAHs have fallen behind on their implementation of electronic medical records(EMRs) and their display of meaningful use[21]. This is important because evidence based guidance, in the form of protocols, pathways, and alerts built into these EMRs assist providers who must address certain conditions rarely[21].
In aggregate, the literature on workforce challenges and opportunities in CAHs lacks systemization, and is focused on published anecdotal experiences and case reports. While these studies provide a lens into the workforce issues experienced in a CAH, they lack the scientific and evidence based rigor associated with large scale, data driven studies in order to make informed decisions.
Quality challenges prior to COVID-19
The literature related to the quality of care in CAHs is quite heterogeneous and can be organized in the categorical groups of structure, process and outcome described by Donabedian in the 1970s. The structure includes the regulatory environment, the organization of the delivery mechanisms and the financing programs available at CAHs. The processes are the interactions that occur to carry on the business. These may be clinical, business or regulatory processes occurring in CAHs. The outcomes are the final determinants of the work effort expended on the customers of the CAHs. This approach will hopefully bring some clarity around the literature related to the quality challenges at CAHs.
From a structural perspective, the Center for Medicare and Medicaid Services (CMS) in their revised rule highlighted the quality requirements that needed to be in place to assure participation in the CMS programs[22]. While the CAHs receive considerable latitude in a variety of quality improvement efforts, this rule specifies the minimum expected performance criteria that need to be achieved even in a resource constrained CAH[22]. Beyond the CMS rule, there are also several other programs that guide the structural quality improvements in the rural environment. These other programs range from hospital outpatient performance reporting for specific functions like imaging[23]to CMS outpatient performance measures more globally and a concern that they may be irrelevant in many communities served by CAHs[5]. An alternative perspective by Schmaltz and colleagues highlighted that while CAHs are not required to be accredited by the Joint Commission, over time Joint Commission accredited hospitals performed better even among CAHs[24].
An additional series of structural measures that attempt to improve care include investments made in technology. While CAHs are resource and capital constrained, programs aimed at improving technology adoption are important to assure quality improvement efforts even in rural environments. For example, the EMR is widely accepted as a mechanism to improve the quality of care associated with medication delivery, improve the coordination of providers and assure that on line decision support improves provider decision making at the point of delivery. Despite the broad scale adoption of EMRs across the nation and specific programs instituted in 2009 as part of the Health Information Technology for Economic and Clinical Health (HITECH), CAHs have been slow to adopt these important structural tools to improve patient care[25–27]. In addition, CAHs are even slower in reaching meaningful use after implementation of the EMRs, which implies that the full value of the tool is not yet attained[21]. There are several reasons for this including the difficulty of convincing providers that the implementation of these tools is necessary, will improve their work, and make their roles more efficient[25,27].
On the process side of quality in CAHs, the literature is robust with examples across different practice settings and disciplines that help to demonstrate the quality of care in CAHs is adequate or can be improved. These examples range from the outpatient arena, to the emergency department[28], to inpatient care with hospitalists[29]to the operating room[30–31]to advance directives[32]and end of life care[33]. When taken together, there are a series of cases and anecdotes that help to highlight the improvements in care in different settings of the CAH.Most of these reports, however, fail to use methods that are reproducible or stringent in their approach.
From an outcomes perspective, there are some welldesigned approaches for evaluating the performance of CAHs using Medicare datasets[34–35]. The first study used national Medicare data and determined that the performance of CAHs was inferior on a number of important process of care indicators and significant outcomes like infections and mortality[34]. The authors refined their work in a second paper that specifically looked at the care provided to Medicare beneficiaries at CAHs and found similar results in inferior outcomes at CAHs for these patients for important outcomes like mortality. While there are important criticisms that can be addressed in the methods of these works[36], these two papers represent some of the more robust and systematic analyses related to outcomes at CAHs.
Access to capital prior to COVID-19
The literature related to capital access for CAHs is nonexistent despite the importance and the need for continued investment in these settings. There are reasons why the search may have failed to demonstrate any results. These include search terms that were too narrow, a time- frame that was too short,or perhaps the use of PubMed was the incorrect search engine to identify the literature based on CAH's access to capital. To address these issues, the period for sources was expanded from 10-20 years. This did little to identify literature that was relevant to the current plight of CAHs and their capital needs. Next,additional search terms were attempted: Critical Access Hospitals AND Finance; Access Hospitals AND Bonds; Critical Access Hospitals AND Investments; Critical Access Hospitals AND Funding.None of these provided a literature that was relevant to the problem facing CAHs. Finally, since a search of the evidence based literature using PubMed did not lead to effective source documents, a review of the gray literature using Google was attempted.
Using the search terms Critical Access Hospitals AND Capital Access, a range of documents were obtained. Notable among them is the Rural Health Information website, which is a comprehensive website for rural health generally and CAHs specifically[37]. This website had a range of important information related to the problem of capital access and the opportunities for funding capital, but is written from the perspective of representing the CAHs and may be biased in the provided information.Nonetheless, they are included so that an assessment regarding a CAHs access to capital can be performed.
The capital needs of a CAH are numerous and range from infrastructure items like fire suppression equipment, physical plant modification or replacement, and technology enhancements for the delivery of care. Many CAHs struggle with an aging infrastructure and are barely able to reach a positive bottom line for operations. This makes the need to access capital imperative if the CAH wishes to sustain its operation over time[37].
There are both traditional and nontraditional approaches to accessing capital. Traditional approaches include loans, bond issuance, or letters of credit. In addition, nontraditional approaches, like federal subsidies and block grants may assist with investments in program expansion or for clinical tools like the EMR. Some specific federal programs are available for infrastructure and equipment from the USDA, the Economic Development Authority and the Administration for Children and Families[37]. In order to reduce the burden of debt, some CAHs are turning to long-term leases for everything from clinical buildings to equipment. This approach has the added advantage of being able to retain investments and cash in a liquid form[37]. In addition, some are using an opportunity to improve access via local or regional philanthropy (Erwin, 2015).
In addition, a study by Gregg at the University of Minnesota was particularly helpful in understanding the problem, although the study was published in 2005[38]. In this work, which used a survey design of over 700 CAHs, the investigator found that CAHs self-reported that they were significantly undercapitalized by $700 million to $1 billion[38]. In 2020 dollars, there is a 31.3% increase thus this represents an under-capitalization of approximately $920 million to $1.3 billion. Of importance, additional loans were being accessed in larger and larger amounts and the success of obtaining those loans continued to exceed 80%[38]. The major efforts for the use of these loans was plant improvements, expansions, and the acquisition of technology and equipment. Gregg identified a major problem with this approach in the ongoing needs for enhanced operational performance by these CAHs to cover the debt service of the loans and to continue to invest in their facilities without the necessary cash flow from operations[38].
Overall, the peer-reviewed literature had few relevant citations for access to capital for CAHs. The gray literature had several very robust references that while dated, seem to continue to be relevant in the current context of CAHs.
Summary of the challenges facing CAHs prior to COVID-19
There were numerous challenges facing CAHs in the healthcare context prior to COVID-19. Among them were challenges with payment, quality, access to capital and workforce. A literature review and synthesis for each of these major challenges highlighted that, in fact, the challenges are real and substantial. However, there is also clarity that eliminating the CAH designation or changing the criteria including distance may disproportionately affect these 1350 facilities and the infrastructure that has helped to sustain healthcare in the rural environment prior to COVID-19.
How COVID-19 worsens the plight of CAHs
The COVID-19 pandemic exacerbates the challenges facing the sustainability of CAHs and the access to healthcare for people living in the rural environment. Further, COVID-19 demonstrates the particular vulnerability of CAHs not only around the traditional challenges, but also adds a range of new concerns that jeopardize the health and well-being of people who live in the rural environment throughout the United States.
Public health infrastructure and response
The public health model
Public Health is defined as the "infrastructure and systems necessary to allow communities, urban settings, and nation-states to provide physical and societal protections to their populations"[39]Successes of public health have been referred to as "silent triumphs" and present alongside advances in societal development which guarantee clean water, food,sanitation, and shelter[39–40]. In contrast to the medical model, the public health model operates out of a commitment to the population's health, striving to achieve "the greatest good for the greatest number"and focusing on an approach that allocates healthcare resources effectively (utility) and fairly (distributive justice)[41–43]. Physicians play an important role in public health, such as mandatory reporting of infectious diseases, implementing screening practices,and promoting prevention through primary care. The tools used in the public health model are informed by physician practice such as gathering patient data or observation of clinical trials. A major difference is that the science behind the work of public health is primarily interested in prevention and evaluation strategies rather than focusing on the cure of disease.Table 2compares key differences between the medical and public health model.
To avoid a duplication of efforts, the public health and medical models work separately, but together towards overall improved health. While there are consistent challenges in access to care in the medical model, there is a continued investment in infrastructure for public health that is derived from a tax base. However, addressing population health in rural communities can have challenges due to a lack of funding for infrastructure causing many rural and frontier regions to be without local health departments. Public health funding is set up hierarchically in a way that flows from the federal to the state and local level, unlike the medical model,where payment for services through reimbursements occur from multi-payer systems.Table 2contrasts the public health and medical models.
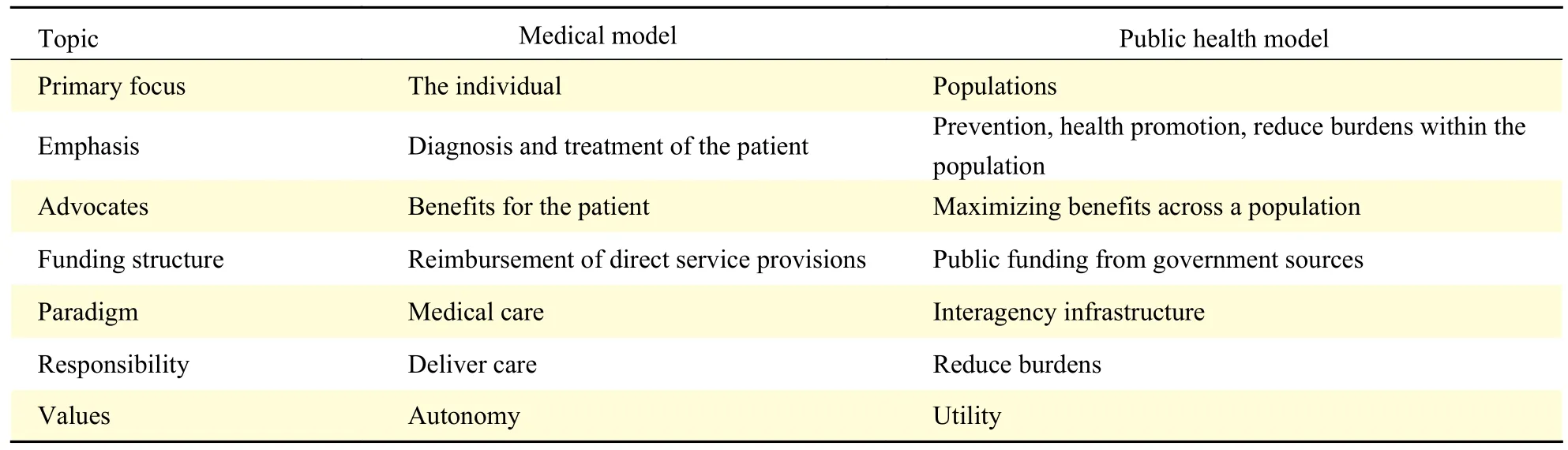
Table 2 A comparison of the medical and public health models
Pandemics and the crisis of scarcity
Pandemics are large-scale outbreaks of infectious disease that can greatly increase morbidity and mortality over a wide geographic area and cause significant economic, social, and political disruption[44]. In the context of the COVID-19 pandemic, we face a public health emergency stemming from a scarcity of resources including N95 masks, ventilators, test kits, hospital beds and staff due to a surge in hospitalizations[39]. The Institute of Medicine states that the emphasis in a public health emergency must be on improving and maximizing the population's health while tending to the needs of patients within the constraints of resource limitations[45]. Public health emergencies justify temporarily adjusting practice standards and shifting the balance of ethical concerns to emphasize the needs of the community rather than the needs of the individual (Table 3). Substantial changes in the usual and traditional health care operations are justified in certain circumstances and formally declared by state government, resulting in crisis operations for a sustained period[45]. Rural communities and CAHs are at a higher risk of suffering from resource scarcity and limited response capabilities such as fewer hospital beds and a smaller supply of ventilators and facemasks.
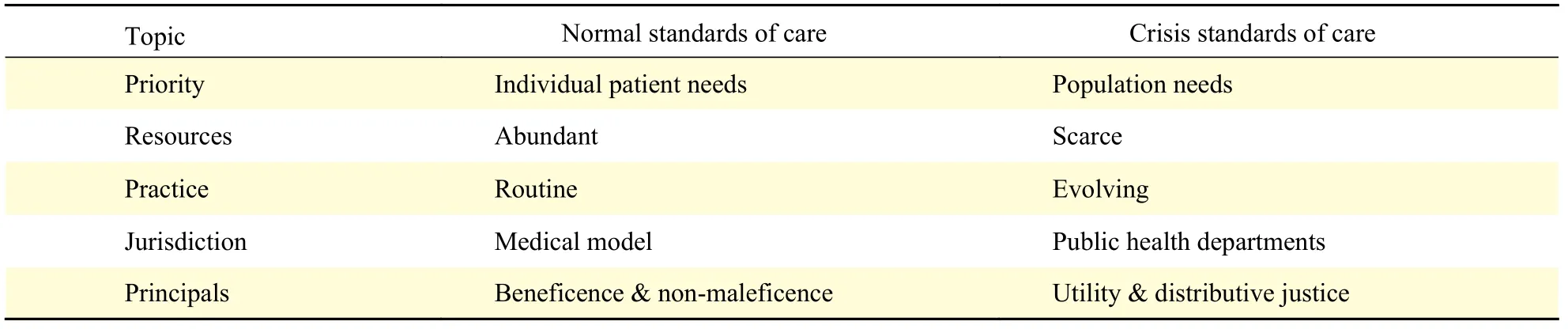
Table 3 A comparison of the normal and crisis standards of care
Public health departments have jurisdiction when state and national emergencies are declared, resulting in the medical model becoming subordinate to the hierarchical demands of incident command. What this means, is that during times of a national or state emergency public health decisions prevail. This is important for a number of reasons. First, the needs of the larger community take precedent over the needs any individual patient. Second, at times when the medical model and public health model run inconsistent with one another, the public health model prevails. Third, this is particularly important during times of resource constraints, which CAHs may be vulnerable to during a pandemic considering one of the designations of being a CAH is to have no more than 25 inpatient hospital beds[46]. During these situations, the public health guidelines that determine implementation protocols for conservative resources prevail over the decisions of any individual provider.Table 3provides a comparison of the shift in priorities, resources, practices, jurisdiction and principles under normal standards of care versus crisis standard of care.
While providers have been educated within the medical model, the transition to a public health model is often challenging and difficult because it is perceived as reducing the autonomy of the medical provider. The benefits of this approach however include the fact that any individual provider is not responsible for the kind of life and death allocation decisions where resources are constrained, but rather the opportunity comes from protocols and guidelines implemented with the community's best interest at hand.
The implementation of crisis standards of care can result in a shift in priorities that may be difficult, but necessary during disaster response. It is understandable that this shift in priorities may cause ethical tension between patient-centered and population-centered considerations. An awareness of the stressful nature of this tension is likely found in the clinical context of pandemic emergencies where it is acknowledged that crisis protocols shift outcome priorities from the individual to the population,creating ethical tension for health professionals who are educated to care for individuals rather than populations[43].
Why does public health matter?
The need to shift standards of care during a pandemic from the medical model to the public health model can be exemplified in role-fidelity as it applies to the use of ventilators. Some providers may find it unconscionable to make decisions about the allocation of scarce resources in the context of a pandemic,which is why the public health response takes precedent in these circumstances (Table 3). We ought not to place the responsibility of allocating resources on the shoulders of individual providers, forcing them to decrease their advocacy for patient care. To alleviate this burden, the literature encourages a system that shifts from apatient-physician dyadto apatient-physician-population triad[43].This way, the decision-making focus for the allocation of scarce resources is done through appropriate protocols and guidelines established by crisis standards of care through the public health model (Table 3).
Traditional challenges facing CAHs in the context of COVID-19
Early reports suggest that the rural environment may be relatively spared from a surge of COVID-19 patients given their remote location and distance from major urban settings where the prevalence and infectivity rates are staggering. The extent to which these rural communities can use public health interventions and remain 'cloistered' and free from disease remains questionable. It is likely that as the pandemic continues to spread even the rural environments will begin to see patients as migratory trends suggest that the virus will ultimately reach across both urban and rural environments. The four traditional challenges facing CAHs, payment, quality,access to capital and workforce, are worsened by the presence of COVID-19 and depending upon the duration of crisis may be detrimental to the ability of CAHs to survive over time without intervention long term and sustainable payment reform.
Payment
The care of patients with COVID-19 is expensive,depending on the severity of disease. Patients treated for critical illness experience a substantial duration that is atypical in the current reimbursement paradigm.While a number of remedies have been advanced,including payment remediation and federal funding through the Coronavirus Aid, Relief, and Economic Security (CARES) Act to reimburse hospitals, the current estimates are that these mechanisms are insufficient should a CAH experience even a few patients with COVID-19 that need to be cared for[47].An analysis by the Kaiser Family Foundation found that the formula used to allocate funding in the CARES Act favored hospitals with the highest share of private insurance revenues and would provide disproportionately less funds to hospitals that see a relatively smaller number of patients with private insurance[48]. A Separate analysis done prior to COVID-19 on the financial viability of US rural hospitals showed that 354 hospitals across 40 states were at high risk of closing, representing more than 222 350 annual discharges, 51 800 employees and$8.3 billion in patient revenue[49]. Any downturn in the economy will likely worsen these crises for rural hospitals and CAHs. Historically, health care has been relatively unaffected by recessions, however,COVID-19 has had dramatic effects on the economy due to government mandated shutdowns that also directly applied to hospitals[50]. Most hospitals,including CAHs, were required to cancel elective surgeries and other revenue generating services for the intended outcome of reducing exposure. Additionally,the closure of non-essential businesses and subsequent loss of tax dollars and increased unemployment claims, has led to reduced budgets for government agencies with the potential of effecting future CAH payments.
Workforce
The workforce issues facing CAHs under normal circumstances include both a limited number of providers and a broad range of specialty experience.Under the pandemic, the risks to this limited workforce from fatigue, burnout, or illness are accentuated. The limitations that exist to experience diversity is also an important factor where specialists in clinical disciplines may be limited. When combined with the novelty of the clinical syndrome presented by COVID-19, the limited availability of specialty care,particularly intensive care unit care, and limited access to technologies that provide for specialty consultation,the workforce challenges become daunting and the provision of care may suffer as a result. These difficulties are not simply addressed by changes to the supply chain. For example, even if ventilators were to be made available to CAHs, they require an experienced, multidisciplinary team for their use to derive optimal benefit in outcomes and minimize complications from care. Without experienced providers across disciplines, the provision of equipment of this type does little to enhance care in the setting of a pandemic where ventilator use is necessary for large segments of the population if affected.
Quality
Structure
The lack of infrastructure and personnel have become the centerpiece to the challenges facing CAHs during the COVID-19 pandemic. An aging and potentially compromised infrastructure has proven to be ill equipped to address the needs of widespread COVID-19 in the rural environment. For example, one of the designations to become a CAH, having ≤ 25 inpatient beds, may be the reason the hospital is unable to respond adequately to an outbreak within a rural community. Many CAHs do not have sufficient isolation rooms, ventilators, or personnel to staff surges in patient volume. In addition, the challenges around the adoption of technology in CAHs highlighted above exacerbates structural challenges to care as substantial elements of care in the non-rural setting have transitioned to virtual platforms during the pandemic; thereby leaving health maintenance and routine care at risk in the rural space.
Process
Systematic and fundamental quality control mechanisms are limited under normal circumstances in CAHs. As described above, the literature is limited to published innovative improvements, but systematic analyses regarding the provision of quality combined with a lack of formal and universal accreditation processes, like the Joint Commission, can further compromise the provision of care in CAHs during the pandemic because fundamental processes may not have been 'hardwired' in the normal context of care prior to COVID-19.
Outcome
Outcome appraisals usually take time, particularly when done well, systematic assessments of outcome in the rural environment generally and CAHs specifically have been performed using large administrative datasets. However, the problems are that these comprehensive data sets depend on claims data that need to be processed; hence, there is an extraordinary lead time until outcome data become available for analysis. In addition, these datasets, while helpful to assess the macro-environment, may not have sufficient granularity to address changes that need to be made in the micro-environment of the CAH.
Access to capital
The limitations for accessing capital for infrastructure for CAHs have been highlighted. The ability to provide capital for infrastructure needs like buildings, equipment, and technology, although substantial to fortify the CAH infrastructure, is certainly possible with a variety of mechanisms of traditional and innovative support. The problem being the lead-time for implementation, even if funds were available, it would be too long and time consuming to be undertaken within the limitations and constraints of a pandemic. The opportunities for infrastructure remediation may have already passed or be so difficult to implement that capital does not appear to be the rate limiting step during the pandemic; rather, lead time,the availability of equipment, and workforce would make capital improvements difficult.
New challenges in the context of COVID-19
While the traditional challenges of payments,workforce, quality and access to capital are important within the context of COVID-19, there are also some new realities that need to be considered. First, the traditional backup mechanism for limitations in the rural setting is to transfer a patient to a level of care that suits their condition. Under the strained conditions of the pandemic, the settings that usually accept these patients will also be constrained for equipment, supplies, and personnel in caring for their primary service areas. The result is that the normal backup mechanisms may simply not be able to accommodate transfers from the rural environment in the same way as they did prior to the pandemic.Second, many of the responsibilities for addressing the COVID-19 pandemic fall under the public health model as described above. Unfortunately, the current public health infrastructure has been overwhelmed during this pandemic on federal, state, and local levels. Many rural jurisdictions simply lack a public health infrastructure and personnel so that there is insufficient bandwidth to address a crisis of this magnitude. As a result, fundamental public health services, such as staying abreast of the evolving literature for best practices, implementing prevention,screening and surveillance programs, and managing contact tracing, are dependent on a single individual,when in actuality; it requires an entire team of qualified personnel to run these response efforts.These responsibilities may then fall to the next closest county or to the state for management when these entities themselves are already overwhelmed. Finally,the result of a system that is already constrained under normal circumstances is an inadequate backup plan and detrimental gaps within the public health infrastructure. The reality is that citizens living in rural America are left to fend for themselves, hope they do not get sick, and if they do will have to piece together an approach that works individually for them and their family. Unfortunately, this is the antithesis of public health guidance and entrains significant variability in the process of care and diminished outcomes overall.
Conclusions
The Balanced Budget Act of 1997 created a designation for Critical Access Hospitals because of an increase in hospital closures in the rural environment over the preceding decade. This effort was intended to sustain care for people living in the rural environment over time. Now, 25 years later,1350 CAHs serve approximately 18% of the US and a systematic policy evaluation has yet to be performed.Further, the challenges presented over the last eight months related to COVID-19 has created an unprecedented series of consequences to both the public health infrastructure and healthcare delivery system.
Despite the large number of CAHs, these hospitals continue to struggle with major challenges that compromise their sustainability over time. Of the challenges analyzed in this literature synthesis,payment mechanisms, quality, access to capital, and a skilled workforce were among the most important. In addition, there are new challenges related to COVID-19 including challenges to the redundant plans for these communities, a lack of public health infrastructure, and the inherent variability derived from citizens creating individual plans for their care.Efforts to sustain CAHs over the next decade will require additional policy interventions that account for overcoming or moderating the challenges in each of these areas.
There are a number of goals that need to be achieved to assure that CAHs are going to meet the intent and purpose of the Balanced Budget Act of 1997. First, there must be a goal that assures rural communities continue to have access to health and hospital care in a way that demonstrates excellence and can address the ongoing and evolving challenges of COVID-19. Second, there must be a means of assuring that CAHs get access to capital to improve their physical plants, technology, and access to a skilled workforce in order to provide the level of excellence that is expected. Finally, to the extent possible, these hospitals should not cost more to run when analyzed at the level of the US health system.Said differently, a goal that establishes a net neutral cost structure is necessary for any new policy revisions or recommendations. With these goals in mind, it becomes clear that policy changes are needed if access, cost, and quality are to be assured for those living in rural America considering the status quo was simply not sustainable prior to COVID-19 and may be insurmountable after COVID-19.
 THE JOURNAL OF BIOMEDICAL RESEARCH2020年6期
THE JOURNAL OF BIOMEDICAL RESEARCH2020年6期
- THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- An unusual COVID-19 case with over four months of viral shedding in the presence of low neutralizing antibodies: a case report
- Identification of therapeutic drugs against COVID-19 through computational investigation on drug repurposing and structural modification
- Subgroup comparison of COVID-19 case and mortality with associated factors in Mississippi: findings from analysis of the first four months of public data
- Identification of county-level health factors associated with COVID-19 mortality in the United States
- Characteristics of viral specimens collected from asymptomatic and fatal cases of COVID-19
- Modeling the transmission dynamics of COVID-19 epidemic: a systematic review