
Peroral endoscopic myotomy for management of gastrointestinal motility disorder
2020-06-17 05:53ZheFengZiMingLiuXiangLeiYuanLianSongYeChunChengWuQingHuaTanBingHu
World Journal of Clinical Cases 2020年11期
Zhe Feng, Zi-Ming Liu, Xiang-Lei Yuan, Lian-Song Ye, Chun-Cheng Wu, Qing-Hua Tan, Bing Hu
Zhe Feng, Zi-Ming Liu, Xiang-Lei Yuan, Lian-Song Ye, Chun-Cheng Wu, Qing-Hua Tan, Bing Hu,Department of Gastroenterology, West China Hospital, Sichuan University, Chengdu 610041,Sichuan Province, China
Abstract
Key words: Endoscopy; Achalasia; Peroral endoscopic myotomy; Esophageal diverticula;Gastroparesis; Pyloric stenosis
INTRODUCTION
Over the last decade, peroral endoscopic myotomy (POEM) has been introduced as an alternative treatment option for patients with achalasia. POEM is an operation that is conducted to establish a tunnel between the esophageal mucosa and the muscularis propria through an endoscope. This operation is based on endoscopic submucosal dissection and natural orifice transluminal endoscopic surgery, and tunnel establishment and muscle incision are regarded as two essential elements. Compared with traditional treatments including medication, Botox injections, pneumatic dilation, and laparoscopic Heller myotomy (LHM), POEM has significant advantages of minimal invasiveness and a low rate of adverse events (AEs) when performed by experienced operators[1]. POEM should be strongly recommended as the first-line and standard treatment option for patients with achalasia[2,3]. Besides, POEM is a feasible and effective treatment for other gastroesophageal diseases such as gastroparesis (GPOEM) and esophageal diverticulum (D-POEM). Recent studies have showed promising results of POEM for these diseases. Till now, it has been the preferred treatment option in most of the centers, with excellent and similar long-term results as the conventional strategies.
CLASSICAL POEM
POEM is an alternative technique for patients with achalasia, and this was first introduced in 2010 for conducting myotomy under the guidance of an endoscope[4,5].Over the last decade, POEM has been considered an initial treatment option for patients with achalasia[3]. The detailed procedure is as follows[1]:
Establishment of mucosal entry
First, the site for anterior mucosal incision should be selected by correlating with high-resolution manometry (HRM) parameters. It is generally existing in the middle of the esophagus,i.e., about 13 cm above the esophagogastric junction (EGJ). For type III achalasia, it is necessary to establish the entrance above all the stenotic loops that are caused by abnormal contraction (the stenotic loops can be seen under the endoscope, and the abnormal contraction sites can also be measured by HRM). All the stenotic loops should be cut open. The key point in this step is to judge the "EGJ"accurately to avoid a long tunnel, and the indigo carmine is injected into the submucosal layer.
Establishment of submucosal tunnel
A 1.5 cm to 2cm longitudinal or horizontal mucosal incision was made in the mid esophagus. Next, a blunt dissection was created followed by carbon dioxide insufflation, and the submucosal tunnel was extended towards the EGJ for about 2 cm to 3 cm onto the gastric cardia. The length of the tunnel, which is usually 5 cm to 15 cm[6-9], depends on the choice of each surgeon according to the patients’ conditions.Also, the basic principle is that the length of the tunnel allows enough space for a full muscularis incision.
Myotomy
This part of operation is highly controversial. Classically, the circular fibers, lower esophageal sphincter (LES), and stomach are divided, leaving the longitudinal layer intact. The length of myotomy is generally 8-10 cm, with at least 2 cm below the EGJ.The myotomy length of achalasia type III is determined according to the stenotic loops.
Closure of mucosectomy
Finally, after an adequate myotomy, the tunnel was checked for any blood exudation or electric injury on large vessels and washed several times. The mucosectomy site was then closed by using hemostatic clips or endoscopic sutures.
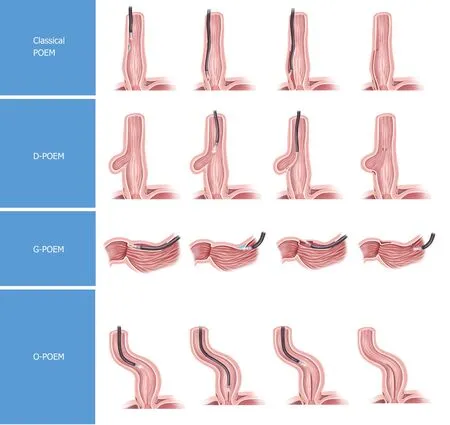
Figure 1 Schematic representation of peroral endoscopic myotomies. The procedures of classical peroral endoscopic myotomy (POEM), esophageal diverticulum POEM, gastroparesis POEM, and open POEM are shown in this figure. The blue part in the procedure represents the injection. POEM: Peroral endoscopic myotomy; D-POEM: Diverticulum peroral endoscopic myotomy; G-POEM: Gastroparesis peroral endoscopic myotomy; O-POEM: Open peroral endoscopic myotomy.
After LHM and pneumatic dilation (PD) as first-line treatments for achalasia,POEM has been the widespread and recognized technique. A systematic review and meta-analysis conducted by Schlottmannet al[10]showed that POEM is more effective than LHM in improving the symptoms like dysphagia, but is associated with a higher incidence of gastroesophageal reflux according to short-term results. An analysis of more than 1300 patients by Shiwakuet al[2]also confirmed that POEM is a safe and effective option, supporting it as a first-line and standard treatment for achalasia. A randomized clinical trial by Pondset al[3]have further demonstrated that for treatment-naive patients with achalasia, POEM resulted in a higher treatment success rate at 2 years when compared to PD. In addition, for patients aged below 18 years[11,12]or with gastric bypass[13], POEM treatment was proved to be clinically effective and safe.
All these findings above suggest that POEM might be an initial and standard treatment option for achalasia.
OPEN POEM
Liuet al[14]have described open POEM (O-POEM) without a submucosal tunnel for treating achalasia. Considering the most common potential complications of high technical requirements for tunnel construction and mucosal injury associated with OPOEM, the endoscopic myotomy by this technique is considered to be much safer and more feasible and effective under direct visualization and by leaving the postresection mucosal defect open[15,16]. The O-POEM procedures are as follows[16]: (1) Sterile saline solution was injected into the submucosa to perform mucosectomy (6-10 cm above the gastroesophageal junction at the 5–6 o’clock position) with at least 2 cm below the EGJ into the proximal stomach; (2) After mucosectomy, the submucosal fibers were extended from the proximal end to the distal end; (3) Next, selective myotomy of the circular muscle for at least 4–6 cm proximal to the EGJ and 2 cm distal to the EGJ was performed. Much attention should be paid while conducting the procedure to avoid cutting the longitudinal muscle layer. However, the longitudinal muscle is so thin that it might play by itself; (4) After completing the incision, a smooth passage exists with minimal resistance through the EGJ; and (5) After that, a nasogastric tube was inserted into the gastric lumen under endoscopic guidance for gastric decompression,because acid secretion might affect the healing of injury. And the mucosal defect will close by itself.
According to a case series of 82 cases[16], O-POEM seems to be an exceptionally effective treatment over others for achalasia due to a short-term success rate of more than 95%, significant improvement of symptoms and manometry outcomes, and decreased Eckardt score. In that study, the follow-up gastroscopy showed a wider cardia and the radiography displayed an easy passage of barium into the stomach.Moreover, this was comparable to classical POEM[17], and the total clinical reflux complication rate of O-POEM was 15.9%. However, compared with classical POEM,the rates of minor and severe AEs are slightly higher after undergoing O-POEM[18].Nonetheless, most of the O-POEM-related AEs are usually self-limiting and do not require retreatment. Compared with classical POEM treatment, another major advantage of O-POEM is its simplicity and expeditiousness. In that case series, the average O-POEM treatment time was 20.0 min, which was remarkably lower than that of classical POEM treatment[19]. Furthermore, the O-POEM treatment decreases the volume of gas to a certain extent within the working field, possibly lowering the risk of insufflation-related AEs. Considering the difficulty to define a clear separation of circular and longitudinal muscular layers, treatment with O-POEM might lead to potential infection-related AEs. Therefore, prophylactic antibiotics and postoperative gastrointestinal decompression should be routinely applied to prevent possible infection. Based on the indications of O-POEM, the preliminary results demonstrated that it could be a treatment option mainly for patients with severe submucosal fibrosis(such as sigmoid achalasia or patients after Heller myotomy), in which the submucosal tunnel would be technically demanding.
According to other short-term outcomes for achalasia with sigmoid-shaped esophagus or failed Heller myotomy, O-POEM could be a potential first-line treatment[20-22].
DOUBLE O-POEM
An alternative O-POEM was recently described by Yuanet al[23]in a patient with negative predictors of myotomy, namely, severe preoperative dysphagia and esophageal dilatation, and named double O-POEM (D-O-POEM).
The indigo carmine was injected into the submucosal layer, and the mucosal and submucosal layers were incised directly at 9 o'clock position.
After mucosectomy, the circular muscle was cut to 2 cm below the cardia and a fullthickness myotomy was performed at the LES level. During the single procedure, a second myotomy was performed in the same way at 3 o'clock position. The double mucosectomy and myotomy conducted should be of 10 cm and 9 cm in length,respectively.
Finally, instead of using endoscopic clips, the mucosal defects were left open.
According to some short-term outcomes in patients with achalasia in that study, the D-O-POEM might be regarded as a simple and quick treatment for patients with achalasia and negative predictors of myotomy, probably achieving absolute myotomy and averting retreatment.
PERORAL ENDOSCOPIC DUAL MYOTOMY
Yuanet al[24]have described a peroral endoscopic dual myotomy (dual POEM)technique. To avoid repeated intervention for achalasia patients with negative predictors, dual myotomies were performed during a single procedure.
First, the mixture of saline and methylene blue was injected into the submucosa of the posterior esophageal wall.
Next, a hybrid knife was used to make a mucosal entry of about 7 cm above the EGJ, creating an at least half-esophageal-lumen wide submucosal tunnel. Usually,dual POEM is performed separately at 3 o’clock and 8 o’clock positions, and myotomy was extended to 2 cm below the cardia.
The mucosal entry is finally closed using the endoscopic clips.
SHORT TUNNEL POEM
Different from the standard tunnel in classical POEM, Liet al[25]have decreased the length of the tunnel, which might reduce the surgical duration and the rates of post-POEM complications according to the short-term outcomes. The innovative short tunnel POEM procedure is as follows: (1) A 0.8 cm to 1.0 cm wide transverse incision was made at the proximal end of the EGJ, followed by making a 0.8 cm to 1.0 cm longitudinal incision from the middle of transversal incision to the anal side; (2) After that, a short submucosal tunnel was established. The length of the short tunnel was only 6 cm to 8 cm, while that of a standard tunnel was 10 cm to 14 cm; (3) For myotomy, only a part of the circular muscle at the starting point was cut, and the depth of the myotomy increased from the beginning to the cardia area where the fullthickness myotomy was operated; and (4) The entry was closed. Both the transversal and longitudinal incisions lengthwise were closed with titanium clips.
LIU POEM
Liuet al[26]have put forwarded a modified endoscopic myotomy (Liu-POEM) in which the submucosal tunnel is replaced by a submucosal water column. This improvement makes POEM more simplified and less time-consuming. The specific steps are as follows[26]: (1) The patient was placed on the left decubitus position with normal preparation; (2) Longitudinally, a submucosal water column was formed by injecting the saline into the submucosa from the bottom to the middle part of the esophagus; (3)The mucosal layer was cut open and then separated into the submucosal layer under the guidance of an endoscope to form a submucosal space about 2 cm deep; (4) The muscle layer was cut from the proximal esophagus to the bottom of the stomach through the cardia; and (5) The “water tunnel” was closed.
Compared with classical POEM, Liu-POEM demonstrated similar postoperative effects, hospitalization days, and post-POEM complications, such as fever, abnormal routine blood parameters, pleural effusion, and reflux esophagitis[26]. However, after replacement of traditional submucosal tunnel, the duration of operation was significantly reduced, and the laborious steps were simplified. Moreover, the rate of gas-related complications associated with Liu-POEM was lower than that of classical POEM treatment. Furthermore, as the mucosa and muscularis are separated by a submucosal water column, the probability of subcutaneous emphysema and pneumomediastinum is also lower than that of classical POEM.
POEM FOR ESOPHAGEAL DIVERTICULA
In addition to the above modifications, POEM could also be used for treating more diseases, and esophageal diverticula might be one of the indications.
Yanget al[27]have found the possibility of POEM treatment for esophageal diverticula, which was named D-POEM. This unique technique, as a consequence of creating a submucosal tunnel, assists in making septotomy under endoscopic view more methodically and completely. The procedure technique is as follows:
A mixture of 1% indigo carmine, diluted epinephrine, and 0.9% sterile saline was injected into the submucosa 1-2 cm from the diverticular septum to form a mucosal vesicle. A 1 cm incision was then created using a triangular tip knife as an entrance to the tunnel. The submucosal fibers were dissected by spray coagulation, followed by the entry of an endoscope into the submucosal space through the transparent cap. The spray coagulation was then used and indigo carmine solution was injected to form a submucosal tunnel until the diverticular septum was identified. The tunnel should be extended on both sides of the septum till the bottom of the diverticulum.
The septotomy was performed with an insulated tip knife. Under direct endoscopic view, the muscle fibers of the septum were completely dissected till the bottom of the diverticulum. To ensure a complete septotomy, myotomy should be extended to about 1 cm of the proximal esophagus.
Finally, after examination of the esophageal mucosa, the incision was closed with endoscopic clips.
According to a multicenter study[27]and several case reports[28-32], the D-POEM treatment is considered to be feasible, safe, and effective for esophageal diverticula,especially in elderly patients with coexisting diseases which make them unable to tolerate anesthesia, or those with failed previous laparotomy. D-POEM was considered to have a definitive advantage of complete septostomy. Larger multicenter studies are still warranted to confirm this.
G-POEM FOR GASTROPARESIS AND PYLORIC STENOSIS
G-POEM was first reported by Khashabet al[33]in 2013, and could be another alternative treatment for gastroparesis and pyloric stenosis. This is a slightly invasive novel approach for gastroparesis and pyloric stenosis. The process of G-POEM was similar to that of classical POEM that is traditionally performed for achalasia.
Before G-POEM treatment, conventional preparation for endoscopic operation and a high-resolution endoscope with a transparent cap are necessary. Besides, carbon dioxide should be continuously pumped in throughout the whole procedure to keep the vision bright and clear. The particular procedures are shown as follows[33,34]:
A mixture of glycerin fructose and methylene blue was injected into the mucosa approximately 5 cm from the pylorus. Most frequently, a 1.5-2 cm longitudinal incision was made with a triangular-tip knife as an entry into the submucosa.
After the endoscope enters the incision, the submucosal fibers should be isolated and then a submucosal tunnel is established. During this procedure, when the submucosal anatomical plane becomes difficult to define, repeated injection of glycerin fructose and methylene blue mixture strengthens the boundary between the submucosal layer and the muscularis propria. As the submucosal tunnel extends into the pylorus, the operation then should be performed close to the muscular layer to avoid any damage to the mucosal layer during the incision. When a blue mucosa is observed near the pylorus, it can extend 0.5-1.0 cm to the distal end of the tunnel.
The proximal end is returned. The medialis oblique and circular muscle bundles of the pylorus are incised from the proximal end, which was about 2-3 cm away from the pylorus to the end point of the submucosal tunnel.
The incision of the mucosa is closed with titanium clamp.
According to the single institution study[34]and several case reports or case series[35-37], the G-POEM treatment is considered a feasible, safe, and effective method for gastroparesis and pyloric stenosis, especially for medical refractory gastroparesis,in short term. It was also described that G-POEM demonstrates successful improvement in a patient with gastric stenosis post-laparoscopic sleeve gastrectomy[38]. Long-term study for relief from gastroparesis and pyloric stenosis symptoms is still needed.
OTHER POEMS
Considering the time-consuming characteristics of POEM, there are still more improvements that need to be checked in the procedure of POEM. Philipset al[39]have modified the procedure, in which a proximal-to-distal circular myotomy is operated after creating about half of the classical submucosal tunnel (4-6 cm in length). The myotomy continues while the submucosal tunnel extends. This half-tunnel POEM might be more efficient than the classical POEM and the outcome might be equivalent to that of short-term outcome follow-up. On the other hand, Hernandez Mondragónet al[40]have used a new small-caliber endoscope in the POEM procedure in patients with achalasia, and named it thin-POEM. Other procedures are the same as those of classical POEM. With a short-term follow-up of 45 patients after thin-POEM, it might be considered a safe, effective, and feasible option for achalasia treatment. In Digestive Disease Week 2019 United States, Gutierrezet al[41]and Bellet al[42]have described a new POEM treatment combined with transoral incisionless fundoplication(TIF). During the POEM procedure, a flap valve was made after TIF over the cardiac entrance[43]. According to the short-term outcomes of nine patients, the TIF procedure might be a safe and effective solution in treating gastroesophageal reflux disease(GERD) after POEM treatment. As for the length of the incision, Wellingtonet al[44]have offered a possible solution for patients who need minimum myotomy length and showed improved symptoms best indeed. They studied five patients with spastic esophageal disorders and took the use of topography to figure out an optimal length of myotomy for each patient.
RELEVANT DATA
According to data analysis at eight facilities in Japan[2], a total of 1346 patients,including the straight type in 1105 (82%) patients and the sigmoid type in 241 (18%),received POEM during the study period. The operation time was 99.6 min on an average and the mean length of myotomy was 10.8 cm in the esophageal body,extending a mean of 2.8 cm into the stomach. The response rates (Eckardt score ≤ 3) at 3 mo and 12 mo were 95.1% and 94.7%, respectively. During this study, 50 (3.7%) AEs of Clavien-Dindo classification grade ≤ IIIa were recorded and all were resolved during the follow-up treatment. In addition, there were no Clavien-Dindo classification grade ≥ IIIb AEs. On the other hand, post-POEM gastroesophageal reflux was confirmed in 14.8% of patients, and responded well to treatment with a proton-pump inhibitor.
LIMITATIONS OF POEM
However, for some diseases, such as idiopathic achalasia, POEM showed no successful outcomes as before, with a significantly higher likelihood of postoperative gastroesophageal reflux than LHM. According to this research[45], POEM was noninferior to LHM plus Dor’s fundoplication in controlling the symptoms of idiopathic achalasia at 2 years. A total of 221 patients were randomly assigned to receive either POEM (112 patients) or LHM plus Dor’s fundoplication (109 patients).During the 2-year follow-up period, 83.0% of the patients in the POEM group and 81.7% in the LHM group achieved clinical success. The incidence of serious AEs was 2.7% in the POEM group and 7.3% in the LHM group. For the postoperative gastroesophageal reflux, 57% of patients in the POEM group and 20% in the LHM group had reflux at 3 mo as assessed by endoscopy, and the corresponding percentages at 2 years were 44% and 29%, respectively.
DISCUSSION
Since its first introduction in 2010, POEM has already been considered an initial and standard treatment instead of LHM and PD[2,3]. However, POEM has been especially challenging. For instance, submucosal fibrosis might be the most common cause of failed tunneling, and morphological changes in the esophagus such as curved esophageal lumen might cause out of direction. Only experienced endoscopists could perform this technique. Moreover, as for the problems of “time-consuming”, “high technique-demanding”, and “post-POEM complications”, more modified POEM introduced above were created to solve these problems.
Liuet al[14]have introduced the “open POEM”, in which myotomy was directly performed without a submucosal tunnel to treat complex achalasia such as submucosal fibrosis and sigmoid esophagus. Compared with conventional POEM procedures, the O-POEM does not require submucosal tunneling. The procedure reduces high technique-requirement relatively. Based on the O-POEM, the D-OPOEM[23]was created for patients with negative predictors of myotomy, despite the risk of perforation or leakage and similar potential infection-related AEs. On the other hand, another modified POEM (Liu-POEM)[26]replaced the tunnel by a water column,which greatly reduced the duration and complexity of treatment. Besides, POEM with a shorter tunnel (short tunnel POEM) was described due to its association with high safety and low rates of AEs.
For other disadvantages associated with POEM treatment[39-44], such as post-POEM gastroesophageal reflux, POEM with TIF showed unique superiority over other modifications. For the problem of “time-consuming”, thin POEM and half tunnel POEM might be possible solutions. As POEM was applied in many centers, several other indications including esophageal diverticula (D-POEM) and gastroparesis and pyloric stenosis (G-POEM) have been developed. Relevant short-term studies[27-38]confirmed improvements in symptoms with POEM treatment.
As for the potential complications, infection and perforation are main potential complications for O-POEM. Prophylactic antibiotics and postoperative gastrointestinal decompression could help with possible infection. The perforation is mainly related to the operator's technology. It is still recommended that doctors with rich traditional POEM surgery experience perform O-POEM operation. The main complication of Dual-POEM and double-O-POEM is the reflux problem. According to current experience, the reflux that occurs in these patients is relatively mild (the proportion of grade A esophagitis will be larger, and rarely grade C or above). And the incidence of esophagitis is equivalent to that of traditional POEM. PPI treatment can achieve good results, and no case requires additional fundoplication. Some scholars[46]proposed adding fundoplication to the classical POEM procedure to reduce gastroesophageal reflux.
CONCLUSION
In summary, although short-term outcomes of various modifications in POEMs have proved them to be safe and effective, multiple large sample studies and randomized clinical trials are still warranted to discuss the relief from symptoms, post-POEM events, and long-term consequences.
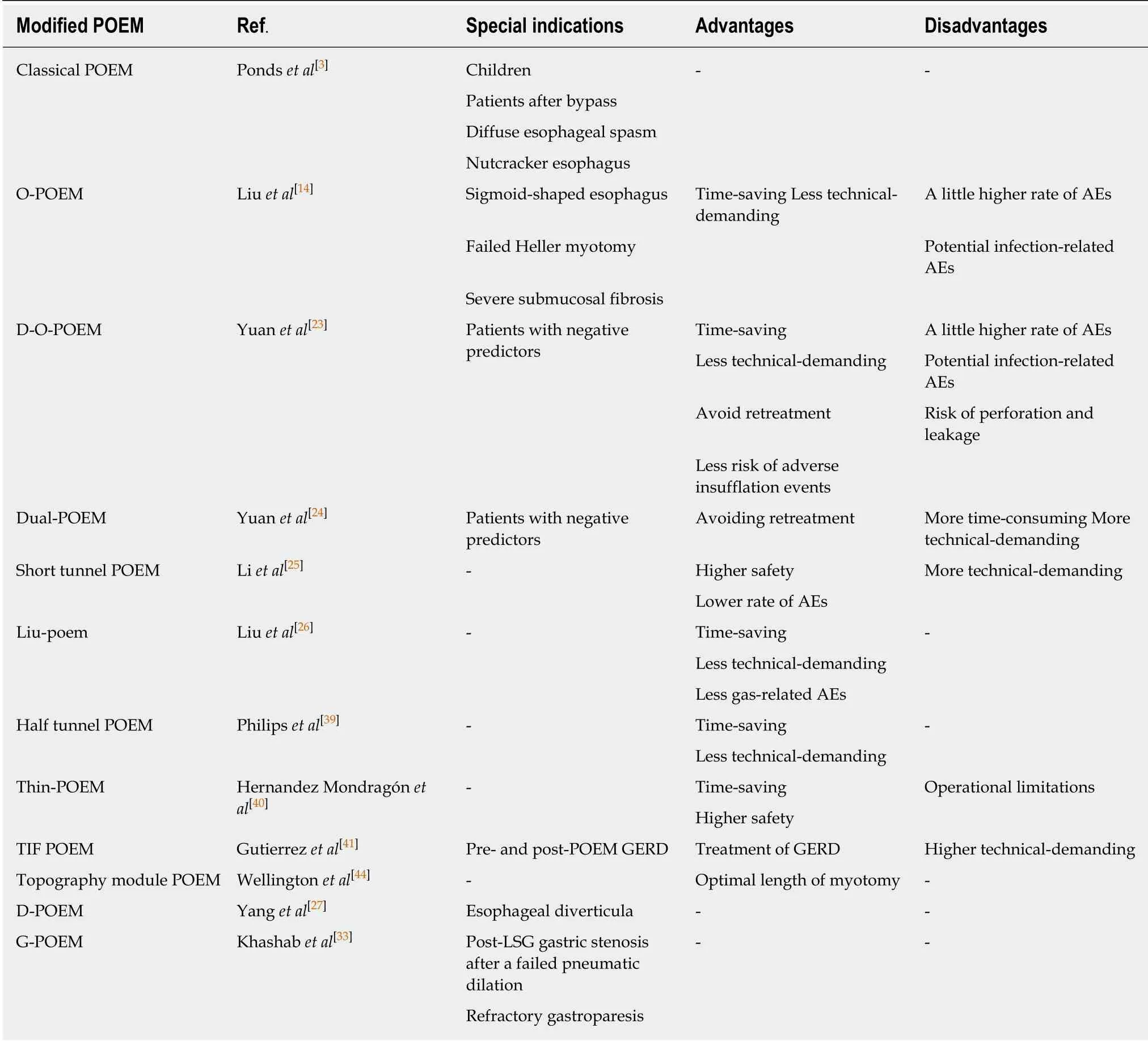
Table 1 Comparison of advantages and disadvantages of different peroral endoscopic myotomies and specific indications
 World Journal of Clinical Cases2020年11期
World Journal of Clinical Cases2020年11期
- World Journal of Clinical Cases的其它文章
- Tumor circulome in the liquid biopsies for digestive tract cancer diagnosis and prognosis
- Isoflavones and inflammatory bowel disease
- Cytapheresis for pyoderma gangrenosum associated with inflammatory bowel disease: A review of current status
- Altered physiology of mesenchymal stem cells in the pathogenesis of adolescent idiopathic scoliosis
- Association between liver targeted antiviral therapy in colorectal cancer and survival benefits: An appraisal
- Clinical prediction of complicated appendicitis: A case-control study utilizing logistic regression