
The impact of inspiratory muscle training on exercise capacity and inspiratory muscle strength in heart failure patients: a meta-analysis
2019-12-11 01:58:54MengYaJingXiaoYiLiXueYunHaoGuoMinSong
TMR Non-Drug Therapy 2019年4期
Meng-Ya Jing,Xiao-Yi Li,Xue-Yun Hao,Guo-Min Song
1Graduate College,Tianjin University of Traditional Chinese Medicine,Tianjin,301617,P.R.China.
2Department of Nursing,Tianjin Hospital,Tianjin,300211,P.R.China
Abstract
Keywords: Inspiratory muscle training,Exercise capacity,Inspiratory muscle strength,Heart failure,Meta-analysis
Introduction
Heart failure is a complex clinical syndrome caused by various cardiac structural or functional abnormalities that impair ventricular filling and ejection capacity[1]and has become an increasingly important health worldwide problem [2-3].The peripheral and respiratory muscles in heart failure patients are impaired,resulting in reduced inspiratory and expiratory function.Thirty to fifty percent of patients with chronic heart failure have declined inspiratory function,exercise intolerance and muscle weakness/deconditioning,which lead to the decline of their life quality and a poor prognosis [4].Studies have shown that inspiratory muscle training (IMT) can improve cardiopulmonary function and improve exercise endurance and quality of life in patients with heart failure[5-7].However,not all studies have reached the same conclusion [8].Therefore,this study conducted a meta-analysis method to comprehensively evaluate the effects of IMT on heart failure patients,in order to provide a basis for clinical practice.The meta-analysis was planned and conducted in accordance with Cochrane Collaboration recommendations and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Materials and methods
Inclusion criteria
Types of studies: RCTs,whether adopting blind methods or allocation concealment,with the language of Chinese and English.
Types of participants: age ≥ 18 years old; all the involved participants meet the New York Heart Association cardiac function classification class II-IV.
Types of interventions: patients in the experimental group accepted the IMT with/without additional treatment.IMT included inspiratory muscle training with device,fast inhalation training,chest breathing training and abdominal breathing training.Additional treatment including basic medication,dietetic regulation,education,routine care,and aerobic exercise; the control group did not take any intervention or only received the same additional treatment as the experimental group.
Outcomes: (1) 6-minute walking distance (6-WMD)test (according to the “6-minute walking distance test guide” [9]); (2) peak oxygen uptake (Peak VO2); (3)maximum inspiratory pressure (MIP); (4) first second forced expiratory volume (FEV1); (5) forced vital capacity(FVC).
Exclusion criteria
(1) Non-Chinese and English literature; (2) repeated publications; (3) key data missing,unable to get contact with author;(4)patients with severe other organ diseases;(5) patients with physical disabilities; (6) patients with mental disorders or cognitive impairment.
Searching strategies
Computer retrieval of PubMed,EMbase,the Cochrane Library,Web of Science,CBM,Wanfang Data,VIP and CNKI databases were conducted to collect RCTs on the efficacy of IMT on the cardiopulmonary functions in patients with heart failure.The search time was from the built time to March 31st,2018.The search used a combination of subject words and free words.English search terms include: “breathing exercises”,“respiratory muscle training”,“inspiratory muscle training”,“heart failure”,“cardiomyopathy,dilated”,“ventricular dysfunction”,“randomized controlled trial”; The study design group of keywords included the terms randomized controlled trials,clinical trials and controlled trials;At the same time,the original studied included in the references and subject-related systematic reviews included in the study was retrospectively supplemented to ensure the recall rate.The specific search strategies are as follows(Figure 1):
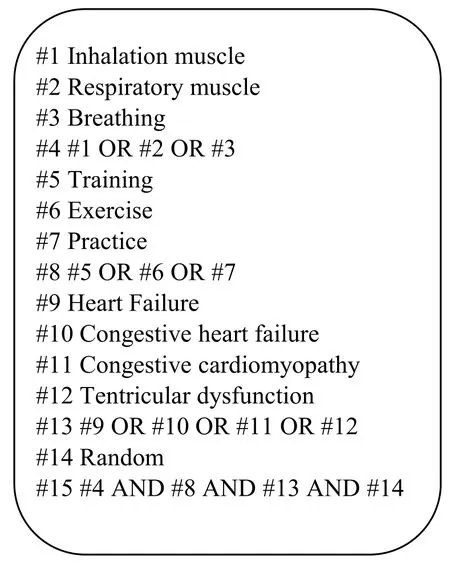
Figure 1 The specific search strategies of the meta-analyses
Literature selection and data extraction
Two researchers independently screened the articles,extracted the data and cross-checked.If there were any objections,the two sides will discuss or listen to the opinions of the third researcher.Use the self-made data extraction table to extract relevant information,including:(1)basic information included in the study:research topic,first author,publication time,etc.;(2)basic characteristics of the research subject: age,number of cases,etc.; (3)intervention measures; (4) treatment time limit; (5)outcome indicators of concern.
The assessment of methodological bias risk
Methodological quality evaluation was performed using the bias risk assessment tool for RCT recommended in the Cochrane Handbook 5.1.0 [10].The evaluation content included random sequence generation,allocation concealment,blind method for participants,integrity of result data,selective outcome report and source of bias.Each item was judged on three levels such as low risk of bias,high risk of bias and unclear risk of bias[11].
Statistical analysis
Meta-analysis was performed using RevMan 5.3 software.Continuous variables were expressed as mean difference(MD) or standard mean difference and 95% confidence interval (CI).Classified variables were expressed as risk ratio(RR)and its 95%CI.The heterogeneity between the included studies was analyzed by χ2 test (test level is α =0.1),and the size of heterogeneity was determined by quantitative analysis with I2.If there is no statistical heterogeneity between the results of each study,a fixed effect model is used for meta-analysis; if there is statistical heterogeneity between the results,further analysis of heterogeneity source,after excluding the effects of significant clinical heterogeneity,a random effects model was used for meta-analysis.For obvious clinical heterogeneity,subgroup analysis or sensitivity analysis was used for treatment or descriptive analysis only.The test level of the meta-analysis was set to α =0.05.
Results
Search results
A total of 759 articles were obtained through the initial inspection of the database.And at last,a total of 20 RCTs[12-31] meeting the inclusion criteria were included,of which 10 RCTs were reported in English and the other 10 RCTs were reported in Chinese.The literature screening process and results are shown in Figure 2.
Basic characteristics of the included studies and bias risk assessment results
The number of participants in the analyzed studies ranged from 16 to 300,resulting in a total of 1,415 subjects.The samples of the selected studies largely consisted of middle-aged and elderly individuals with mean age ranged from 53.3 to 75.0 years.All studies included individuals of both genders.The basic characteristics of the included studies are shown in Table 1.The table contains the source,age,number of cases,intervention methods,intervention time and outcome indicators.And results of the bias risk assessment are shown in Figure 3.
Effects on outcome indicators
6-MWD.A total of 14 literatures reported the effects of 6-MWD,while the Palau 2014 [16] research using a different form data reporting method was not included.The overall results are shown in Figure 4.The meta-analysis comparing the IMT group with a control group showed a pooled standardized mean effect on exercise capacity of 59.41 (95% CI (51.02-67.80),P<0.001).However,there was a large statistical heterogeneity (P< 0.001,I2= 92%) between the combined results,so sensitivity analysis was used to explore heterogeneous sources by removing the selected RCTs one by one to recalculate the overall correlation results and I2.After analysis,the source of heterogeneity may be related to the intervention time.The heterogeneity was eliminated after removing the three studies [13,28,30] (P= 0.14,I2= 35%),and there was a statistically significant between the control group and the experimental group (MD = 45.10,95% CI (39.08-51.13) ,P<0.001).Subgroup analysis under different training time was further conducted,the results showed that taking IMT less than 10 months,could improve the 6-MWD score by 39.07 (95% CI (33.31-44.84),P<0.001,fixed effect model (P= 0.75,I2= 0%)),while taking more than 10 months,6-MWD score could increase by 68.00(95%CI(45.15-90.85),P<0.001);the 6-MWD scores of patients who received the IMT from the admission to discharge increased by 46.76 (95% CI(44.83-48.69),P<0.001,fixed effect model(P=0.89,I2=0%)).
Peak VO2.A total of 6 articles reporting peak VO2were included.There was a large statistical heterogeneity between the combined results (P<0.001,I2= 96%).Therefore,sensitivity analysis was carried out,and a study was excluded in turn,and heterogeneity did not change significantly.Therefore,the random analysis model was used for meta-analysis.The results showed that there was no difference in the change of peak VO2in the experimental group (MD = 1.37,95% CI (-0.57-3.30),P=0.17)(Figure 5).
MIP.A total of 8 RCTs reporting the MIP results were included.There was a slight statistical heterogeneity between the pooled results (P= 0.37,I2= 8%),and a meta-analysis using a fixed-effects model showed that the experimental group was able to increase MIP compared with the control group.(MD = 15.59,95% CI (12.96-18.21),P<0.001) (Figure 6).Subgroup analysis showed that the MIP scores of 1-2 months of intervention were not significantly different from those of the control group(MD = 12.10,95% CI (-0.15-24.35),P= 0.050).There was no heterogeneity (P=0.56,I2=0%),the fixed effect model was used; The MIP score of the intervention for 3 months was statistically significant compared with the control group (MD = 15.76,95%CI (13.07-18.45),P<0.001).The combined results showed that there was no heterogeneity between the studies (P= 0.19,I2= 35%),the fixed effect model was used.
FEV1.A total of 3 articles assessing FEV1 were included.Meta-analysis showed no difference in FEV1 changes in the experimental group (MD = -5.79,95% CI (-12.23-0.65),P=0.08)(Figure 7).
FVC.A total of 3 articles reporting FVC were included.There was no statistical heterogeneity between the combined results (P= 0.17,I2= 44%),and the fixed analysis model was used for meta-analysis.The results showed that there was no difference in FVC between the experimental groups (MD =-0.45,95%CI(-6.39-5.49),P=0.88)(Figure 8).
Discussion
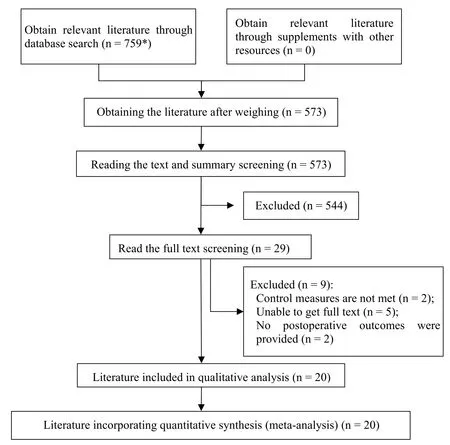
Figure 2 Eligibility and data-synthesis PRISMA flow diagram.
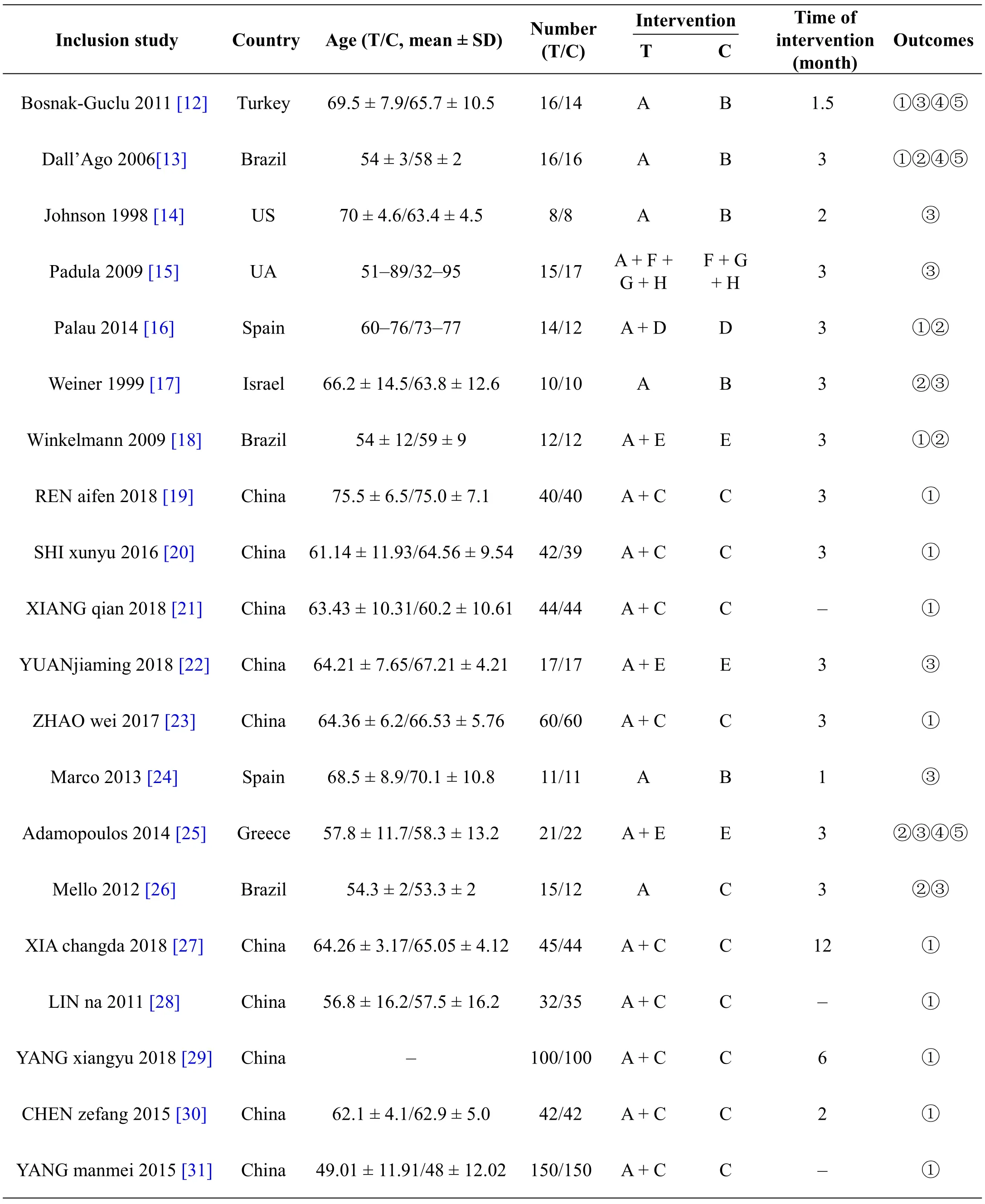
Table 1 Basic characteristics of the included studies
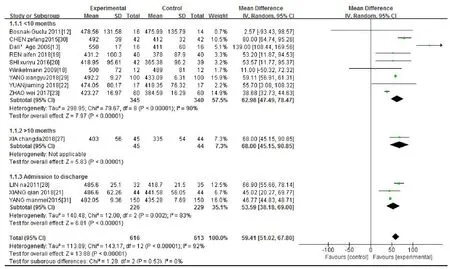
Figure 4 The effects of IMT on 6-MWD in patients with heart failure.
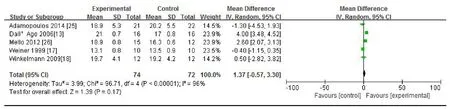
Figure 5 The effects of IMT on peak VO2 in patients with heart failure.
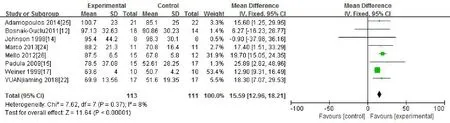
Figure 6 The effects of IMT on MIP in patients with heart failure.

Figure 7 The effects of IMT on FEV1 in patients with heart failure.

Figure 8 The effects of IMT on FVC in patients with heart failure.
IMT is used to exercise the muscles with inspiratory function based on diaphragm,to enhance their muscle strength and endurance,improve heart and lung function,and promote the recovery of exercise capacity [20].According to our results,IMT was associated with improved exercise capacity and inspiratory muscle strength strength to some extent.This study showed that IMT can increase the 6-MWD of patients with heart failure,and subgroup analysis of different training duration was basically consistent with the above results.Therefore,it was recommended to use this training.However,the data indicated that training period and intensity played important roles in improving respiratory muscle strength,which supported the implementation of resistance exercise training programs both for healthy individuals and patients with chronic diseases.Through a certain degree of continuous training,exercise endurance can be improved and cardiopulmonary function can be enhanced [20].To achieve such clinical effects,oral encourages,persuades,interprets,repeats,etc.,should be provided to enhance the patient's self-efficacy of IMT[32]and improve patient compliance.
Studies of patients with heart failure had provided evidence supporting the role of MIP as a strong prognostic factor of mortality.MIP is also a useful indicator of the optimal timing for cardiac transplantation in heart failure patients.This study showed that inhaled muscle training can increase the MIP of patients with heart failure,and subgroup analysis of different training duration were basically consistent with the above results.Regarding the training period and intensity,in each study,the time and intensity of the inhalation muscle training performed by the researchers were different and were not clearly defined.
This study showed that inhalation muscle training did not improve Peak VO2,FEV1,and FVC in patients with heart failure.The study by Laoutaris [33] showed that FVC and FEV1 were significantly improved.Considering factors such as baseline lung function,medication,inspiratory muscle exercise,intensity,sensitivity of different populations to training,etc.,may influence the results stability and accuracy.Further research is needed.The present systematic review called attention to the need for randomized studies to assess the factors affecting the potential benefits of IMT.
Finally,readers should interpret our results in light of low quality of included studies,although this ultimately reflects the body of evidence about IMT and relevant outcomes for heart failure patients.New large-scale randomized controlled trials are needed to confirm the findings of this systematic review.
Conclusion
IMT seemed to be a useful strategy for improving exercise capacity and inspiratory muscle strength in heart failure patients,which could improve 6-MWD and MIP,but not the PVO2,FEV1,and FVC.
- TMR Non-Drug Therapy的其它文章
- Hidden in the hands-the special inner Bagua acupoints for pediatric massage
- Non-drug therapies for acute gouty arthritis treatment
- Quality evaluation and content analysis of non-drug guidelines on risk factors of secondary prevention of myocardial infarction
- Mirror therapy:a potential rehabilitation treatment
- Mirror therapy,an important but underappreciated rehabilitation treatment