
Diabetes empowerment scores among type 2 diabetes mellitus patients and its correlated factors: A crosssectional study in a primary care setting in Malaysia
2019-07-23 11:52ThewHuiZhuChingSiewMooiNurainulHanaShamsuddinChingSiewMooi
World Journal of Diabetes 2019年7期
Thew Hui Zhu,Ching Siew Mooi,Nurainul Hana Shamsuddin,Ching Siew Mooi
Abstract
Key words: Diabetes;Empowerment;Scores;Diabetes Empowerment Scale;Type 2 diabetes;Primary care;Malaysia
INTRODUCTION
Diabetes has become a global epidemic of the 21stcentury.Over 70% of known cases of diabetes occur in developing countries.Four hundred and fifteen million adults were estimated to have diabetes globally in 2015,or 1 in 11 adults.This is estimated to rise to 642 million by 2040[1].The Southeast Asian region has seen a recent dramatic increase in diabetes.An estimated 96 million people have diabetes in the region,90%of whom have type 2,which is preventable[2].In Malaysia,the incidence rate has also significantly increased from 8.3% in 1996 to 17.5% (3.5million) in 2015[3].The Federal Territory of Putrajaya was noted to have the highest increment in the prevalence of diabetes in adults,from 2011 to 2015,that is 8.8% to 19.2%[4].Primary care was identified as the backbone in managing diabetes.A majority sought treatment at government health clinics (59.3%) and private clinics (15.1%)[3].Therefore,the population attending government health clinics would provide a better picture of overall diabetes management.
Evidence shows that self-empowerment is important in managing chronic diseases,especially diabetes[5,6].Self-empowerment is an approach that can improve the ability of the patients with diabetes to understand the disease process better,involve themsel-ves actively in self-care,and practise healthy lifestyles for better disease control[6,7].The process of empowerment improves diabetes control by helping patients in making decisions in regards to diabetes care and self-realization of their responsi-bilities in managing type 2 DM[8].Tolet al[9]and Liuet al[10]showed that selfefficacy and self-esteem have a strong relationship with empowerment.However,there are few studies on diabetes empowerment among type 2 diabetes patients in Malaysia.Therefore,this study was conducted to examine diabetes empowerment and its correlated factors among patients with type 2 diabetes in a primary care setting in Malaysia.
MATERIALS AND METHODS
Setting
This is a cross-sectional study of patients registered with a primary health care clinic located in Putrajaya,a Federal Territory and the administrative capital of Malaysia.It has a total population of 91900[11].The study was conducted over a 3-month period from January 2019 to March 2019.
Inclusion criteria
The inclusion criterion for this research included patients aged 18 years and above diagnosed with type 2 diabetes mellitus (DM) and following up for at least 6 months in the primary care clinic.The exclusion criteria included intellectual disability or dependence for activities of daily living,being bed ridden,requiring nursing care to carry out daily activities or being clinically unstable during the study period.The sample size was calculated using the Lemeshow formula based on the prevalence of high DES scores of 36.9% for married and 3.8% for unmarried .The calculated sample size was 322 after taking account of non-respondent rate of 30%,80% power and significance level of 0.05.
Data collection
Face-to-face interviews were conducted using an adapted structured questionnaire.After obtaining ethical approval,we approached the participants and explained the nature of the study before obtaining written consent to participate in the study.Systematic sampling was used to recruit respondents.The estimated number of diabetic patients attending follow up in the primary care clinic is about 15 patients per day,and 900 patients over the three-month duration of data collection.The estimated sample size for this study was 322;therefore,a sampling interval of 3 was used as the constant during study recruitment.The starting number of 1 was selected randomly from the health clinic registration counter using a dice.
Data collection instrument
The questionnaire was initially prepared in English by the author.Then,forward and backward translations into Malay and English languages were performed by two certified translators.The questionnaire was a self-administered type divided into two sections.The first section includes the patients' sociodemographic information.The second section explores the clinical profiles,clinical outcome and total diabetes empowerment scores.
Diabetes Empowerment Scale
The Diabetes Empowerment Scale (DES-28) was developed by the University of Michigan Diabetes Research and Training Center.The questionnaires consist of 28 items with 3 subscales,with each item rated along a 5-point Likert scale (1=strongly disagree,2=disagree,3=neutral,4=agree,5=strongly agree).The range of score was divided in three subgroups as low (28-65 scores),middle (66-103) and high (104-140).Cronbach's alpha coefficient is a measure of internal consistency and can be interpreted as the mean of all possible split-half coefficients[12].By convention,if Cronbach's alpha is greater than or equal to 0.7 to 0.8,there is acceptable agreement[13].
This DES-28 is a reliable tool with good internal consistency (Cronbach's alpha=0.96)[14].The Cronbach's alpha of each subscale was 0.93 for “managing the psychosocial aspects of diabetes”;0.81 for “assessing dissatisfaction and readiness to change”;and 0.91 for ”setting and achieving diabetes goals”.Each coefficient for the overall DES and three subscales was good[14].
For the DES Malay version,the questionnaire was originally in English by the author from the University of Michigan Diabetes Research and Training Center,then forward and backward translated into Malay and English languages by two certified translators.The questionnaire was a self-administered questionnaire,which was pretested through a pilot study prior to the actual data collection.The Cronbach's alpha coefficient for the Malay version total DES was 0.92.
The pilot study included 30 patients,10% of the actual sample size of 322.Recruitment was performed via the systematic sampling method,with every one in two patients registered at the health clinic counter for follow-up selected for the pilot study.About five to eight respondents were collected a day for five days.Question 5 had a spelling error,“realitik” which was corrected to “realistis”.Two other questions were rephrased for easier understanding,namely questions 1 and 2 “apa bahagian”(What part) to “bahagian apa”.The findings from this pilot study were not included in the data analysis of the actual study.
Operational definitions
Ethnicity was defined as Malay,Chinese,Indian or others.Education level was according to the respondents' self-reported highest attained level of education: No formal education,primary school,secondary school or tertiary (diploma/university).Smoking status was defined as whether the patient is a smoker,non-smoker or exsmoker who had quit smoking at least 6 months from the quit date[13].BMI was calculated as the weight in kg divided by the square of height in meter,and classified according to the Asian population[14].Diabetes duration was defined as the duration of diabetes in years.Compliance to treatment was defined as the patients' self-reported compliance to treatment.The clinical outcomes [systolic and diastolic blood pressure,low-density lipoprotein (LDL) level,high-density lipoprotein (HDL) level,triglycerides (TG) level,glycated hemoglobin (HbA1c) %] in this study were defined in terms of the latest levels measured.
Data analysis
Statistical Package for Social Sciences (SPSS) version 25.0 was used to analyze the data collected from the study.Descriptive analysis was used to describe the characteristics of the respondents in terms of frequencies,percentages,median,and interquartile range (IQR).In this study,we used Chi-square test for the categorical data,Spearson's test,Mann-WhitneyUtest and Kruskal Wallis test for the continuous data to identify the associations between the total diabetes empowerment scores with sociodemographic factors,clinical profiles and clinical outcomes.Multiple linear regressions were used to identify the predictors of total diabetes empowerment score.All variables with aPvalue<0.25 in the univariate analysis,as well as clinically significant variables,were entered into the multiple linear regression.The dependent variable was total diabetes empowerment score among type 2 diabetes patients.The independent variables are sociodemographic factors (age,gender,ethnicity,level of education,marital status,smoking status) and clinical profiles (DM durations,DM education exposure,compliances to treatment,BMI,hypertension status,dyslipidemia status,ischemic heart disease status,asthma status systolic and diastolic blood pressure,HbA1c,HDL level,LDL level and TG level).
Ethical approval
Ethical approval was obtained from the Medical Research and Ethics Committee(MREC),Ministry of Health Malaysia (NMRR-17-3085-38099).
RESULTS
A total of 322 participants were recruited into this study,for a response rate of 93.7%.There were no missing data in our study.Table 1 demonstrates the sociodemographic and clinical characteristics of the study population.Median age was 55 years old with IQR of 18.More than half of the participants were male (58.7%,n=189).The majority of the study population were Malay (92.2%),married (92.2%) and had an education above the secondary school level (88.8%).Two-thirds of the participants were nonsmokers (66.5%).With regards to the clinical profiles (Table 2),the median diabetic duration for the participants was 4 years (IQR=7).The mean systolic and diastolic blood pressures are 133.2 ± 15.5 mmHg and 83.7 ± 10.0 mmHg respectively.More than half of respondents were obese (62.7%),had hypertension (64.3%) and dyslipidemia(76.4%).The median for HbA1c was 7.4% with IQR 2.6.The mean for LDL was 3.0 ±1.0 mmol/L.The median for HDL was 1.1 mmol/L with IQR 0.3,and the median for TG was 1.4 mmol/L with IQR 0.9.
Most of the participants had received diabetes education (82%,n=264).The total diabetes empowerment median score was 110 (IQR=10) and classified as high.The median scores of the three subscales were 40 (IQR=4) for “Managing the psychosocial aspect of diabetes”;36 (IQR=3) for “Assessing dissatisfaction and readiness to change”;and 34 (IQR=5) for “Setting and achieving diabetes goal”.Spearman Correlation coefficient showed a statistically significant relationship between HbA1c level (r=-0.132,Pvalue 0.018) with the total empowerment score as shown in Table 3.Mann WhitneyUtest showed that those with diabetes education exposure (P=0.004),received above secondary school level (P<0.001),and those without ischemic heart disease (P=0.004) were statistically significant correlated with total diabetes empowerment score as shown in Tables 4 and 5.
There is no significant correlation between total diabetes empowerment score with other variables like age,diabetes duration,systolic and diastolic blood pressure,gender,ethnicity,marital status,smoking status,hypertension status,dyslipidemia status,asthma status,compliance to treatment,LDL level,HDL level and TG level.According to multiple linear regressions,factors that had significant correlation with higher empowerment scores among type 2 diabetes patients included above secondary education level (P<0.001),diabetes education exposure (P=0.003),lack of ischemic heart disease (P=0.017) and lower HbA1c (P<0.001) as shown in Table 6.
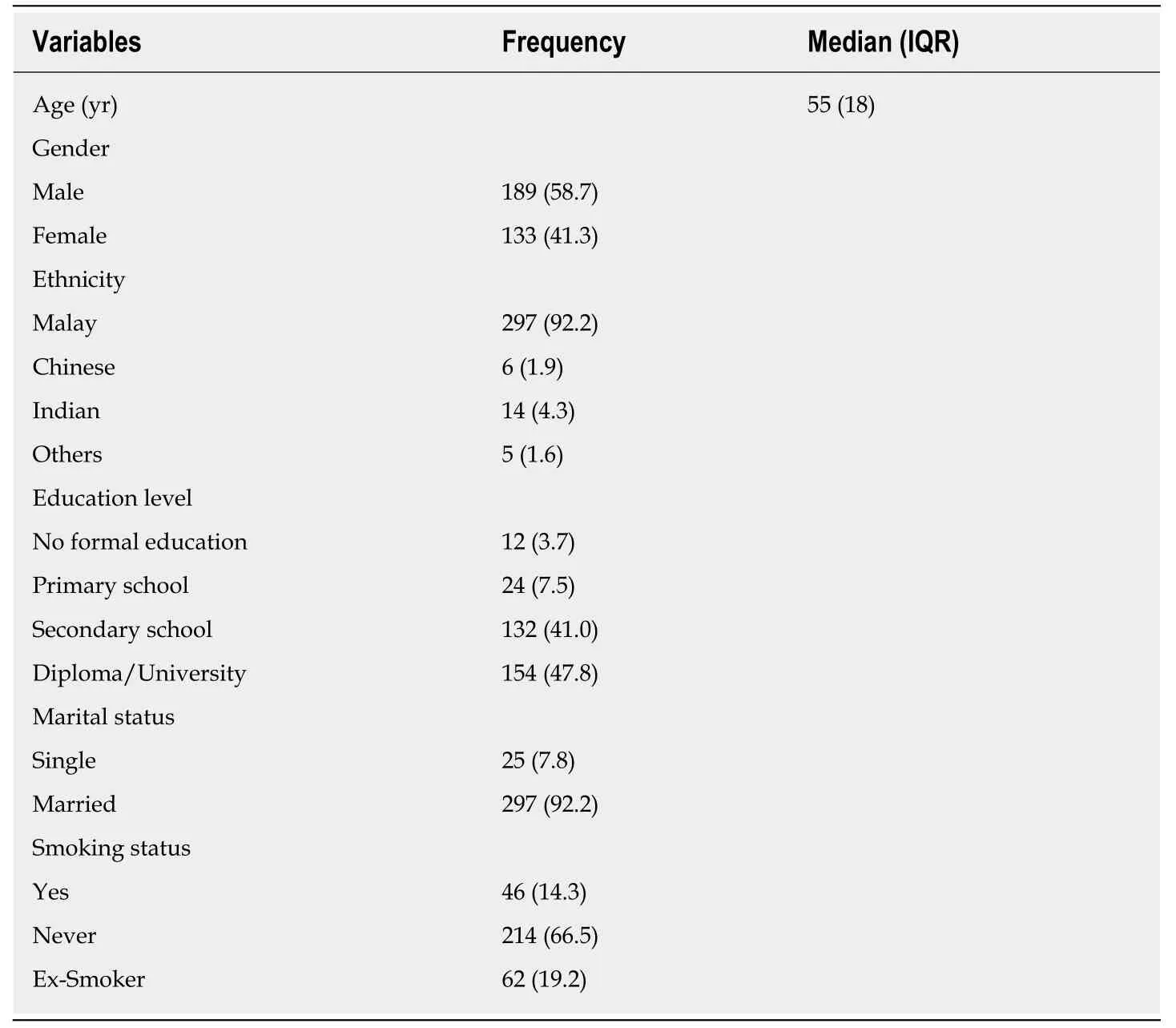
Table 1 Sociodemographic profiles of the study participants in primary health care clinic in Putrajaya (n=322),n (%)
DISCUSSION
In our study,the median score of the total diabetes empowerment was 110.We thus conclude that the empowerment of this study population is high based on the range for high empowerment score range in DES being 104 to 140.The total mean score found by Tolet al[9]was 88.13 ± 30.3,which indicated a middle score according to DES score range,lower than that of our study.This is probably due the difference of the education level between the two study populations,as less than half of their study population had a diploma or higher education,and the study was conducted in a diabetes research centre.A majority of our study population had an education above the secondary school level,the study was conducted in an urban primary care clinic setting.This may be due to socio-culture restrictions as well.For example,in Iran,quality diabetes care is not widely available,with a significant knowledge gap in handling diabetes.Diabetes diagnosis,prevention and management are suboptimal[14].
The study findings showed that the subscale of “Setting and achieving diabetes goal” has highest median score among the three subscales.This finding is similar with two previous studies[15,16].The literature has shown that structured goal setting is the best way to aid diabetes patients to set behavior goals to practice healthy lifestyle and improve HbA1c level[17,18].
This study shows that a higher than secondary school education level is significantly correlated with diabetes empowerment score.This result is similar with other studies.Tolet al[18]showed that an education level of diploma or higher had higher empowerment score.Similarly,D'Souzaet al[19]showed that those with high school and diploma education level had higher diabetes empowerment scores[15,16].This indicates that patients with a higher education level possibly understand the disease process better and have more awareness towards self-care of diabetes management[19].
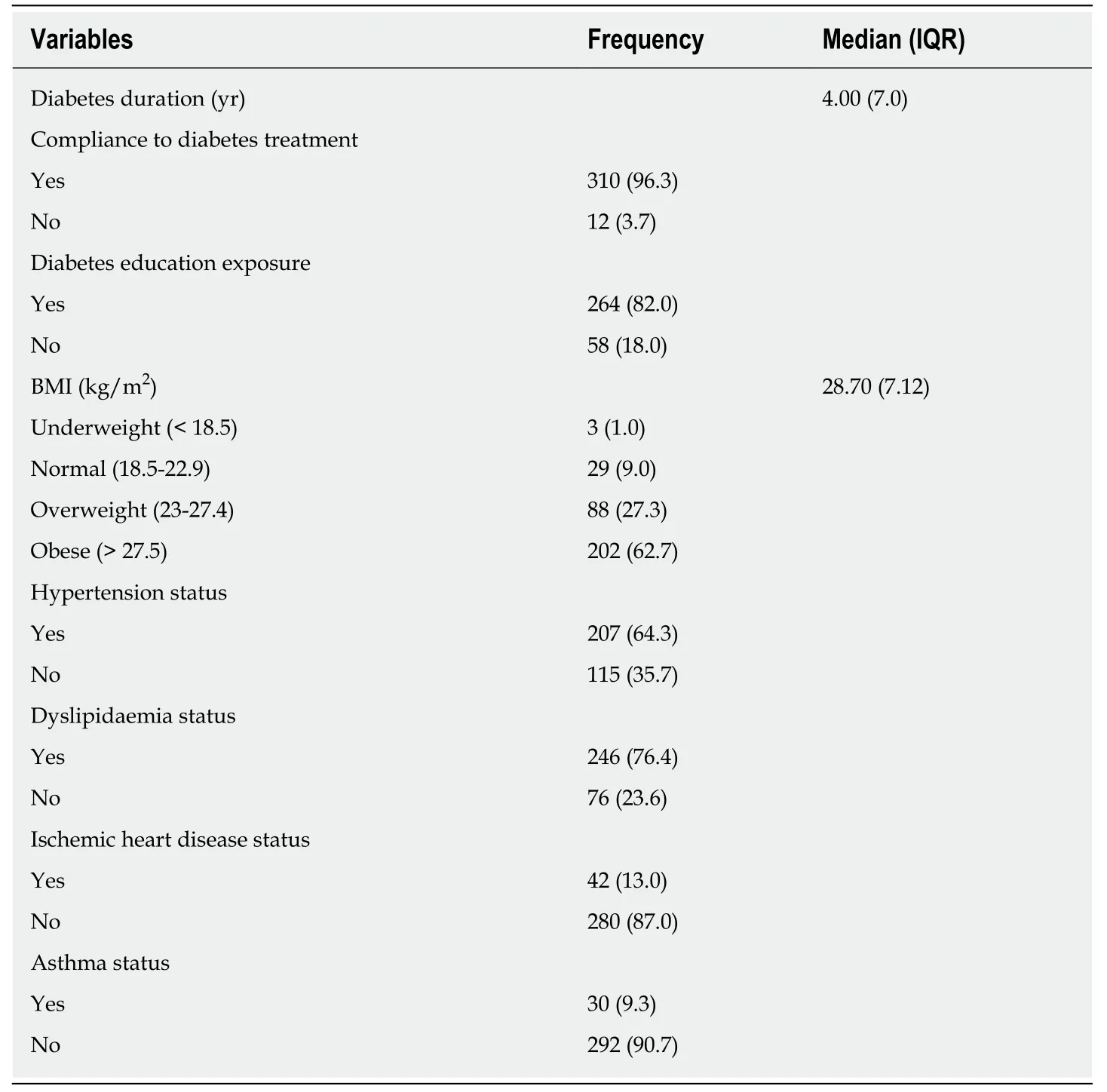
Table 2 Clinical profiles of the type 2 diabetes mellitus patients with total diabetes empowerment scores,n (%)
This study found that diabetes education exposure had a significant relationship with the total diabetes empowerment score.Those participants who had diabetes education exposure had better empowerment compared to those who had no diabetes education exposure.Diabetes education consists of structured programs,which cover basic information on diabetes,insulin therapy,blood glucose levels and targets,physical exercise,diet management and hypoglycemia[20].It incorporates practical skills especially using the home blood glucose monitoring and insulin therapy in diabetes management.The education program also emphasizes the importance of achieving targeted glycemic control to prevent complications and it includes foot care[21].Thus,those who received diabetes education exposure are better skilled in managing their disease,as reported in the literature.Enhancement of patient empowerment is achieved when patients are educated with adequate information on their health conditions[22].
Our study showed a significant correlation between those without ischemic heart disease with total diabetes empowerment score.The majority of the patients without ischemic heart disease had secondary education and above (89.6%),which correlates to higher diabetes empowerment score.
Our study found that HbA1c was 7.4% with an IQR of 2.6.It would be better to compare this to the mean HbA1c for type 2 DM population in Malaysia[23].According to National Diabetes Registry,the mean HbA1c for type 2 DM from 2009 to 2012 was 8.1.Our study showed that a lower HbA1c level was significantly correlated with higher diabetes empowerment scores.This finding is consistent with those of a previous study[16].Patients with higher empowerment score were better in self-care and practicing healthy lifestyle contributing to a better HbA1c level[8,24,25].Age had no significant correlation with diabetes empowerment score in our study.Our study participants were aged between 26 to 84 years old with a median age of 55 (IQR=18).This finding was not similar compared to the study done previously by D'Souzaet al[19]in a study in Oman,which reported that higher empowerment levels were seen among those 40-49 years old.
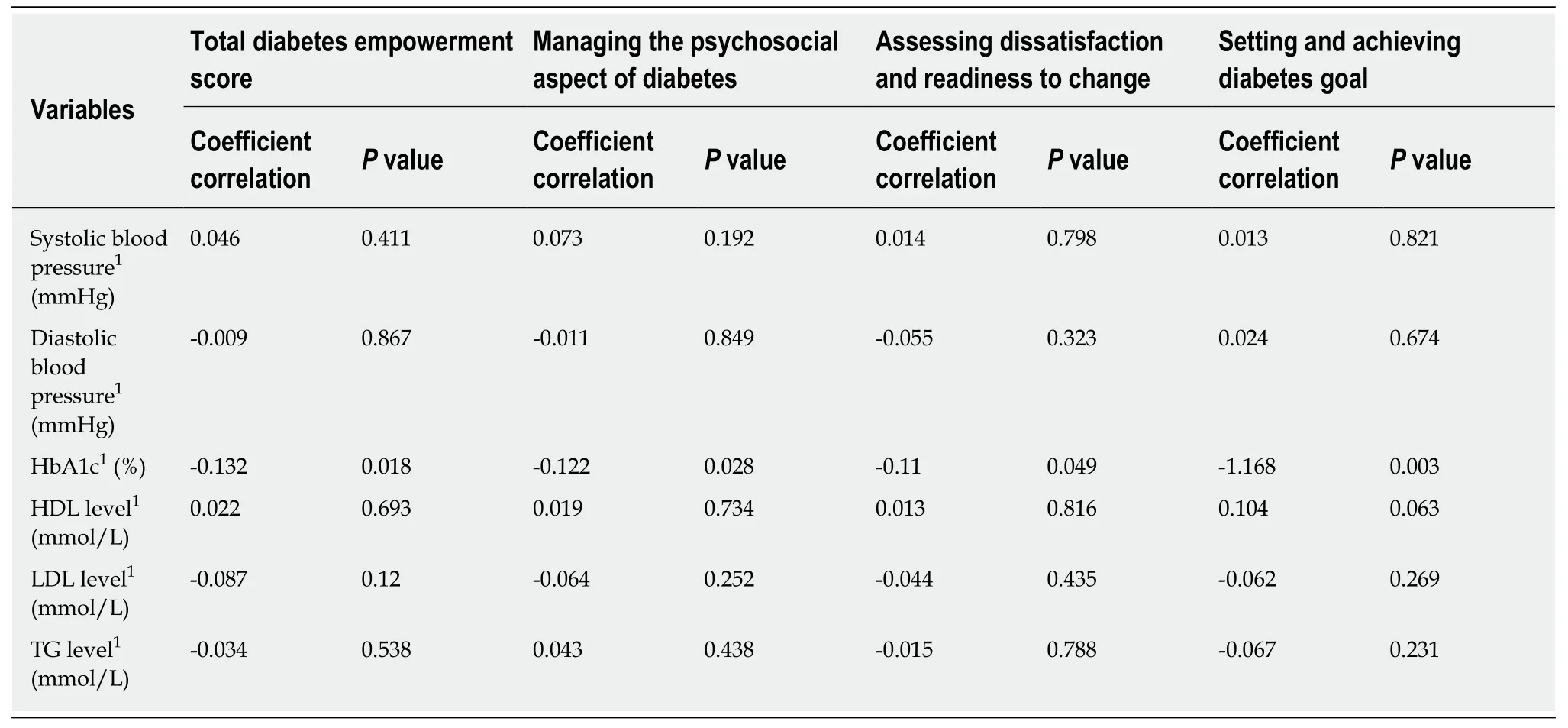
Table 3 The correlation between clinical outcome with total diabetes empowerment scores and subscales and among type 2 diabetes mellitus patients
There is no significant relationship between diabetes duration with total diabetes empowerment score in our study.This contradicts a study done in Oman in which the duration of diabetes was significantly correlated with total diabetes empowerment score[16].The median diabetes duration in our study was 4 years (with IQR=7),similar to a study in Iran[15].However,in the study in Oman,63% of participants had been diagnosed with diabetes for more than 10 years[16].Patients have better empowerment when they had diabetes for a longer duration,which translates into a longer duration of learning and adopting skills and knowledge through experience and exposure to diabetes education to make better decisions for self-care,set targets and achieve goals[10].
In our study,there was no significant correlation between gender and empowerment score.Tolet al[18]showed that females were more empowered than males,probably due to the distribution of their sample,in which more than half of their participants were female.The literature indicates that gender may influence lifestyle modification,as men are more proactive with their health,but women are more likely to change eating habits[26].
Strengths and limitations
To date,this is the first study conducted among type 2 diabetes patients in the primary care setting in Malaysia.Furthermore,the sample size of this study is relatively larger than others in the literature[15,16].In addition,this study has not only identified socio-demographic factors,but also correlates clinical profiles and outcomes with total diabetes empowerment scores,which has not been reported by any local studies,especially in the primary care setting.The limitations are mainly due to the recruitment of participants at a single clinic,which may not be representative of the country's population.This is due to the short duration of the study and limitation of human resources.Therefore,similar future studies should consider multiple centers.This is a cross sectional study,and only an associational and not causational relation can be inferred in this study.
Our study reported high empowerment scores among type 2 diabetes patients.Potential predictors for total diabetes empowerment scores in our study included higher than secondary education level,diabetes education exposure,lack of ischemic heart disease and lower HbA1c levels.
ACKNOWLEDGEMENTS
We would like to extend our gratitude to the Putrajaya district Health Office and Director of Health for their support of our study.The author would like to thank all the primary care doctors and staffs for providing support during the data collection.Last but not least,we would like to thank the Director General of Health Malaysia for his permission to publish this article.
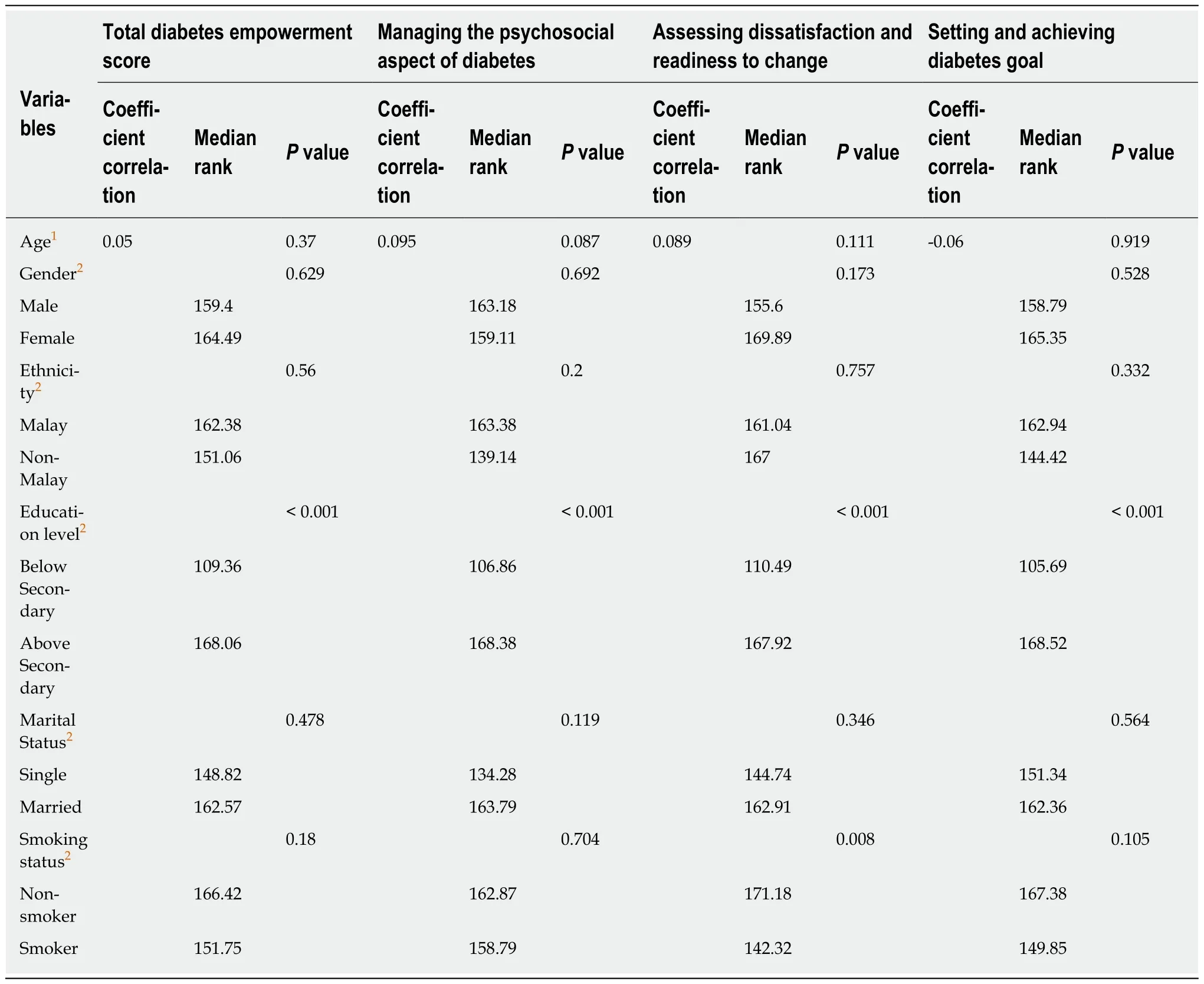
Table 4 The correlation between sociodemographic factors with total diabetes empowerment scores and subscales among type 2 diabetes mellitus patients
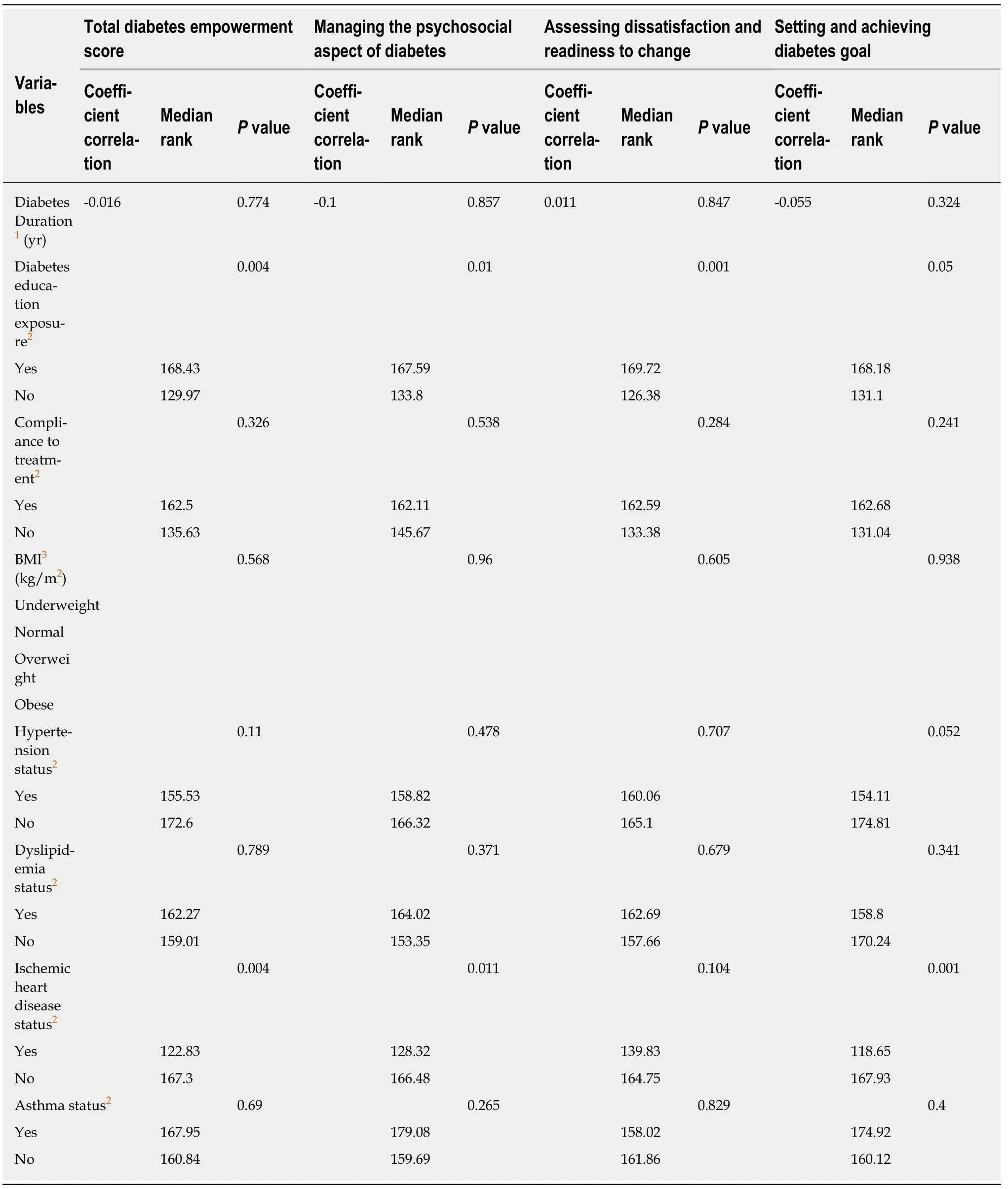
Table 5 The correlation between clinical profiles with total diabetes empowerment scores and subscales among type 2 diabetes mellitus patients
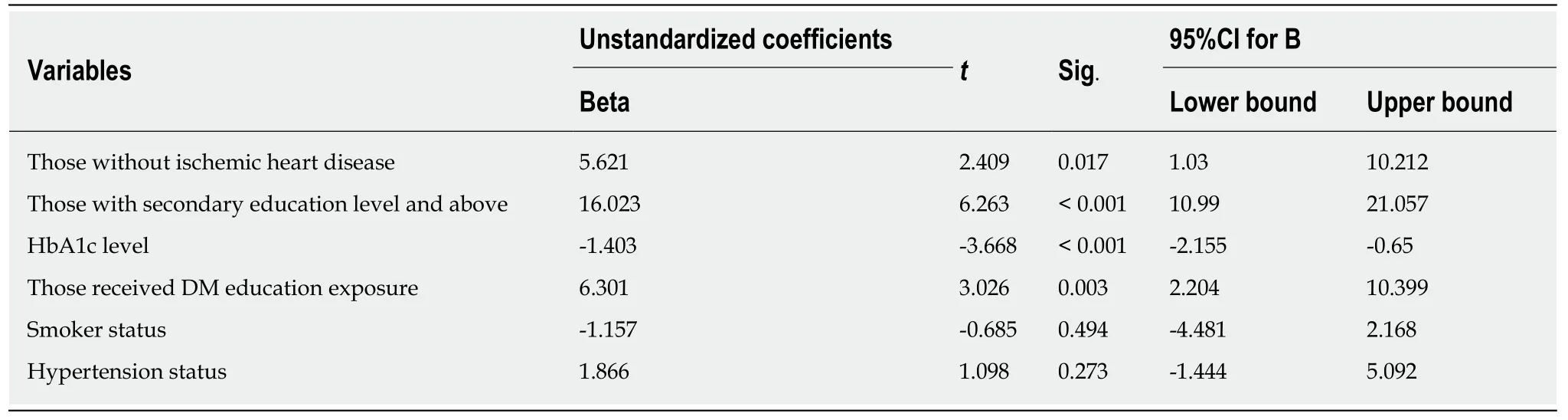
Table 6 Predictor of total empowerment scores among type 2 diabetes mellitus patients using multiple linear regressions
ARTICLE HIGHLIGHTS
Research background
There is a limited study on the diabetes empowerment among type 2 diabetes patients particularly in primary care settings.This study aims to assess the diabetes empowerment scores and its correlated factors among type 2 diabetes patients in a primary care clinic in Malaysia.
Research motivation
Diabetes is becoming a global epidemic of the 21st century and over 70% of known cases of diabetes occur in the developing countries.Evidence shows that self-empowerment is important in managing chronic diseases,especially diabetes.Self-empowerment is an approach that can improve the ability of the patients with diabetes to understand the disease process better,involve actively in self-care and practice healthy lifestyles for better disease control.Therefore,it is very crucial to identify the predictors for diabetes empowerment score among type 2 diabetes patients.
Research objectives
Our objective was to access the diabetes empowerment score among type 2 diabetes patients,also to identify correlated factors with diabetes empowerment scores among type 2 diabetes mellitus (DM) patients in primary care clinic.In addition,we aimed to identify the predictors for diabetes empowerment score among type 2 diabetes patients.
Research methods
This is a cross sectional study involving 322 adults with type 2 DM patients followed up in a primary clinic.Systematic sampling method was used for patients' recruitment.The Diabetes Empowerment Scale (DES) questionnaire was used to measure patients' empowerment.Data analysis was done using SPSS version 25 and multiple linear regressions was used to identify the predictors of total diabetes empowerment scores.
Research results
Median age of the study population was 55 years old,56% were male and mean duration of diabetes was 4 years.The total median score of the DES was 110 [interquartile range (IQR)=10].The median scores of the three subscales were 40 with (IQR=4) for “Managing the psychosocial aspect of diabetes”,36 with (IQR=3) for “Assessing dissatisfaction and readiness to change”and 34 with (IQR=5) for “Setting and achieving diabetes goal”.According to multiple linear regressions,factors that had significant correlation with higher empowerment scores among type 2 diabetes patients were those who had above secondary education level (P<0.001),those who had diabetes education exposure (P=0.003),those who had no ischemic heart disease (P=0.017)and those who had lower glycated he moglobin (HbA1c) level (P<0.001).
Research conclusions
Diabetes empowerment scores were high among type 2 diabetes patients in this study population.The predictors for high empowerment score were those who had above secondary education level,diabetes education exposure,no ischemic heart disease status and lower HbA1c.
Research perspectives
Given the high empowerment score were those who had above secondary education level,diabetes education exposure,no ischemic heart disease status and lower HbA1c,hence all the diabetes patients should be educate and empower on self-care for long-term diabetes management.
 World Journal of Diabetes2019年7期
World Journal of Diabetes2019年7期
- World Journal of Diabetes的其它文章
- Recent advances and perspectives in next generation sequencing application to the genetic research of type 2 diabetes
- Epidermal growth factor receptor rs17337023 polymorphism in hypertensive gestational diabetic women: A pilot study
- HNF1A mutation in a Thai patient with maturity-onset diabetes of the young: A case report