
Fish bone-induced myocardial injury leading to a misdiagnosis of acute myocardial infarction:A case report
2019-04-18 07:23QianQianWangYiHuLiangFengZhuWenJunZhuPengShen
World Journal of Clinical Cases 2019年20期
Qian-Qian Wang,Yi Hu,Liang-Feng Zhu,Wen-Jun Zhu,Peng Shen
Qian-Qian Wang,Peng Shen,Department of Intensive Care Unit,The First Hospital of Jiaxing,Jiaxing 314001,Zhejiang Province,China
Yi Hu,Department of Cardiac Surgery,The First Hospital of Jiaxing,Jiaxing 314001,Zhejiang Province,China
Liang-Feng Zhu,Department of Cardiology,The First Hospital of Jiaxing,Jiaxing 314001,Zhejiang Province,China
Wen-Jun Zhu,Department of Ultrasound,The First Hospital of Jiaxing,Jiaxing 314001,Zhejiang Province,China
Abstract
Key words:Chest pain;Acute myocardial infarction;Pericardial effusion;Fish bone;Case report
INTRODUCTION
Chest pain is the early symptom of numerous life-threatening disease processes.The most common causes of acute chest pain(ACP)are acute coronary events(acute myocardial infarction or angina),aortic dissection,and pulmonary embolism.ACP caused by esophageal foreign body is relatively rare[1].Most patients with ACP are accurately diagnosed and promptly treated based on the individual histories,blood biochemical tests,or imaging examination.Herein,we report the case of a patient with ACP as the chief complaint that was ultimately diagnosed as fish bone-induced myocardial injury.
CASE PRESENTATION
Chief complaints
A 56-year-old man suffering from chest pain presented at the Emergency Department of our hospital on October 25,2015.The patient’s symptoms lasted for nine hours with persistent episodes of chest pain,which have especially worsened over the last 2 h.
History of past illness
The patient had no previous medical history.
Personal and family history
None.
Physical examination
The patient’s temperature was 36.6 °C,heart rate was 120 bpm,respiratory rate was 23 breaths per minute,blood pressure was 97/70 mmHg,and the oxygen saturation in room air was 98%.Heart sounds were very faint and rales were heard in both lungs.All other signs were negative.
Laboratory examinations
The patient’s blood tests showed elevations in cardiac troponin-I(CTN-I)(0.34 ng/mL;normal:< 0.05 ng/mL).Electrocardiograph(ECG)revealed ST segment elevation in the precordial leads II,aVF,and V4-V6.No abnormalities were observed on chest computed tomography(CT).Acute anterior myocardial infarction was thusinitially considered.
Imaging examinations
The patient received dual antiplatelet agents comprising clopidogrel and aspirin at load dosages and underwent emergency percutaneous coronary angiography under the application of nitrates.The operation showed no stenosis in the left main coronary artery or right coronary artery,and about 50% stenosis in the ostial left anterior descending segment and left circumflex artery.
Further diagnostic work-up
Considering that the lowest blood pressure was 74/40 mmHg and it was not possible to maintain normal blood pressure with the help of dopamine,the patient was transferred to intensive care unit(ICU)for further analysis.Subsequently,he required high doses of norepinephrine to maintain blood pressure.Follow-up bedside cardiac ultrasound showed pericardial effusion(Figure 1A).Pericardial tamponade was considered.The patients then underwent pericardium puncture drainage with some 220 mL pericardial effusion;consequently,the blood pressure increased to 110/75 mmHg,while the CTN-I increased to 2.29 ng/mL.At 18:24(see Table 1),the symptom of chest pain worsened and the blood pressure was decreasing.Bedside cardiac ultrasound revealed a large number of pericardial blood clots prompting cardiac tamponade(Figure 1B).Our medical team including cardiology,ICU,and thoracic surgery,taking into consideration the unexplained hemopericardium,decided to preform emergency thoracotomy and pericardium exploratory surgery with the prior consent from patients’ relatives at 19:57.During the operation,the sharp foreign body,a long fish bone measuring about 3.7 cm(Figure 2),was found at the surface of the pericardium and penetrating the left ventricular myocardium to some blood vessels.
FINAL DIAGNOSIS
Finally,the patient was diagnosed with fish bone-induced myocardial injury.
TREATMENT
After removing the fish bone and mending the damaged blood vessels,the patient returned to ICU at 20:55.Reviewing the initial chest CT at local hospital(Figure 3),a strip-shaped high-density shadow at the bottom of the esophagus was found.After being repeatedly inquired of the medical history,the patient admitted to eating fish at dinner,but could not recall swallowing a fish bone.
OUTCOME AND FELLOW UP
The postoperative course was uneventful and CTN-I fell to 0.25 ng/mL.The patient was successfully extubated on day 3,transferred to thoracic surgery department next day,and discharged in good clinical condition after half a month.
DISCUSSION
Acute myocardial infarction or angina is the most common cause of ACP,which is mainly diagnosed by using ECG and blood biochemical test[2].In our case,the patient was misdiagnosed with acute myocardial infarction.His emergency percutaneous coronary angiography was negative.Bedside cardiac ultrasound showed pericardial effusion and pericardium puncture drainage improved the circulation.Nevertheless,persistent pericardial bleeding,unclear bleeding causes,and clot formation led to poor drainage,eventually resulting in worsening of cardiac tamponade symptoms.Considering the possibility of coronary artery injury and lack of the capability of emergency coronary artery bypass at our hospital,our medical team was highly concerned that thoracotomy hemostasis would significantly increase the risk for the patient,while he was reaching the condition when it was no longer safe for him to be transferred to another hospital.We conferred with the patient’s family and obtained their consent for emergency exploratory thoracotomy.Finally,a diagnosis of fish bone leading to pericardial bleeding was confirmed.
Our patient was extremely lucky to survive this penetrating heart injury.Actually,in retrospect to the whole treatment,there are still many aspects worth reflecting on:First,the primary clinician failed to adequately and carefully examine the patient’s history.The existing literature shows that ACP caused by ingested fish bone resulting in esophageal or cardiac injury is not relatively uncommon[3-8].Foreign body ingestion is an important diagnostic clue.Thus,the diagnostic challenge we faced with this patient was that he could not recall swallowing a fish bone,which partly contributed to the initial misdiagnosis.Second,chest CT examination is the preferred technique for suspected esophageal foreign body[9].In this case,the patient underwent CT examination at a local hospital;however,the clinicians failed to observe a highdensity shadow in the lower esophagus.Moreover,the primary clinician at our hospital did not personally read the chest CT,which further contributed to the misdiagnosis.Finally,we failed to timely recheck chest CT,cardiac ultrasound and so on after negative results of emergency coronary angiography,which led to further deterioration of the patient’s condition.
Table 1 Timeline
Therefore,for patients with chest pain,it is necessary to consider the possibility of foreign body in the esophagus or even in the heart.Careful history taking and the corresponding inspection can help to avoid unnecessary damage and safeguard patients from unnecessary pain.
CONCLUSION
Foreign body is a very rare cause of chest pain.Careful history taking and the corresponding inspection can help to avoid unnecessary damage and safeguard patients from unnecessary pain.
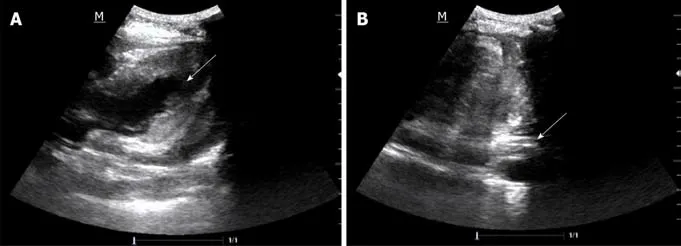
Figure 1 Bedside cardiac ultrasound images.

Figure 2 The fish bone 3.7 cm in size.
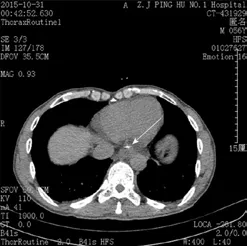
Figure 3 Chest computed tomography image.
 World Journal of Clinical Cases2019年20期
World Journal of Clinical Cases2019年20期
- World Journal of Clinical Cases的其它文章
- Clinical use of low-dose aspirin for elders and sensitive subjects
- Distribution and drug resistance of pathogenic bacteria in emergency patients
- Comparative analysis of robotic vs laparoscopic radical hysterectomy for cervical cancer
- Feasibility of laparoscopic isolated caudate lobe resection for rare hepatic mesenchymal neoplasms
- Soft tissue release combined with joint-sparing osteotomy for treatment of cavovarus foot deformity in older children:Analysis of 21 cases
- Clinical characteristics of sentinel polyps and their correlation with proximal colon cancer:A retrospective observational study