
Endoluminal closure of an unrecognized penetrating stab wound of the duodenum with endoscopic band ligation:A case report
2019-04-18 07:23DaeHoonKimHanlimChoiKiBaeKimHyoYungYunJoungHoHan
World Journal of Clinical Cases 2019年20期
Dae Hoon Kim,Hanlim Choi,Ki Bae Kim,Hyo Yung Yun,Joung-Ho Han
Dae Hoon Kim,Hanlim Choi,Hyo Yung Yun,Department of Surgery,Chungbuk National University Hospital,Chungbuk National University College of Medicine,Cheongju-si 28644,South Korea
Ki Bae Kim,Joung-Ho Han,Department of Internal Medicine,Chungbuk National University Hospital,Chungbuk National University College of Medicine,Cheongju-si 28644,South Korea
Abstract
Key words:Penetrating abdominal injury;Endoluminal treatment;Unrecognized duodenal injury;Case report
INTRODUCTION
Hollow viscus perforations cause considerable mortality and usually require emergency surgery.Rapid diagnosis and treatment of these conditions are essential to reduce the high morbidity and mortality associated with a late-stage presentation[1].The majority of missed hollow viscus injuries result from blunt abdominal trauma,with those resulting from stab-penetrating abdominal trauma less prevalent[2].However,because the duodenum is a retroperitoneal organ,a penetrating duodenal injury can be overlooked.Injuries to the duodenum are associated with high mortality,often associated with a delayed diagnosis[3].A penetrating intestinal injury is an obvious indication for a laparotomy,but endoscopic treatment is extremely rare[4,5].Endoscopic treatment for a penetrating intestinal injury is rare because the endoscopic approach is difficult,peritonitis may be exacerbated during the procedure,and peritonitis cannot be resolved by endoscopic treatment[6].There has been one report of endoscopic treatment for a penetrating gastric injury[7].However,there have been no reports of endoscopic treatment for a penetrating duodenal injury.Herein,we present the first report of a case of a penetrating duodenal injury treated with endoscopy.
CASE PRESENTATION
Chief complaints
A 27-year-old male requested transfer for a self-inflicted abdominal stab wound.
History of the present illness
The patient had stabbed himself in his upper abdomen with a kitchen knife three times,in front of his family.He then visited the emergency room at another hospital,from which he was transferred to our emergency room.According to his family,he was uncontrollable when angry.
History of past illness
The patient denied a history of hypertension,diabetes mellitus,viral hepatitis,or tuberculosis.He had no known drug or food allergies.He also denied a history of operation,trauma,or blood transfusion.
Physical examination
The patient’s vital signs upon arrival were as follows:Blood pressure 100/60 mmHg,heart rate 88 beats/min,respiratory rate 12 times/min,body temperature 37 °C,and oxygen saturation 98% on room air.He was awake,alert,and oriented.However,he complained of tenderness throughout the entire abdomen.We found three stab wounds in the upper-abdominal area.Two stab wounds had not penetrated the peritoneum,but the third had penetrated the peritoneum.There was a 3-cm longitudinal wound in the upper midline abdominal area,and the small bowel and transverse colon were eviscerated.
Laboratory examinations
A complete blood count was obtained showing a white blood cell count of 13.3 ×106/L,hemoglobin 15.3 g/dL,and a platelet count of 229 × 109/L.Electrolyte,coagulation,and blood biochemical tests were all normal.
Image examination
The three wounds in the middle of the upper abdomen were inspected.An exploratory laparotomy detected two perforations in the ileum and mid-transverse colon,which were repaired primarily(Figure 1A).One day after the surgery,the patient became hemodynamically unstable with massive hematochezia,although there was no evidence of bleeding in the Levin tube or Jackson-Pratt(JP)drain.Eight pints of packed red blood cells were transfused,but his hemoglobin value decreased from 10 to 8 mg/dL.Systolic blood pressure was < 80 mg and the patient’s consciousness became unclear.The patient was intubated and transferred to the intensive care unit.An abdominopelvic computed tomography(CT)scan revealed extravasation of contrast medium in the third duodenal portion(Figure 1B).An endoluminal approach for the endoscopic examination was performed in the intensive care unit to identify the bleeding lesions during preparation for the second operation.It showed a large blood clot on the third duodenum;a perforation 0.3 cm in diameter with active bleeding medially into the third duodenal portion was detected(Figure 2).
FINAL DIAGNOSIS
An unrecognized penetrating stab wound in the third portion of the duodenum.
TREATMENT
Several attempts to seal the perforation and stop the bleeding with endoclips failed due to the tangential angle.Next,an endoscopic band ligation(EBL)technique was used to obtain hemostasis and closure of the lesion using a pneumo-active singleband ligator(MD-48709;Akita Sumitomo Bakelite,Tokyo,Japan)(Figure 3A).After EBL,the patient’s hemodynamics stabilized,and no adverse events occurred.Endoscopy 9 d later showed a healing ulcer at the perforation site closed by EBL(Figure 3B).
OUTCOME AND FOLLOW-UP
After EBL,the patient was hemodynamically stable,and there was no evidence of peritonitis or bleeding.He resumed a normal diet 5 d after EBL and was discharged 9 d after surgery.
DISCUSSION
Duodenal injuries are relatively infrequent compared to injuries to other intraabdominal organs,and most duodenal injuries are penetrating injuries.However,a duodenal injury is often diagnosed late because part of the duodenum is retroperitoneal.In addition,a duodenal injury can be missed,resulting in delayed treatment and increased mortality and morbidity[3,8].In the present case,the small bowel and transverse colon were eviscerated at the time the patient arrived at the emergency department.Penetrating injuries to the terminal ileum and transverse colon were detected,and there was no active bleeding into the abdominal cavity.However,the patient became hemodynamically unstable on the day after surgery.The Levin tube and JP drain were clear,but he defecated massive hematochezia.We performed an upper gastrointestinal endoscopy and discovered a missed duodenal injury with active bleeding in the third portion of the duodenum.After endoscopic treatment,we reviewed the initial abdominal pelvic CT scan and detected intraluminal bleeding in the third portion of the duodenum.We missed the duodenal injury because there was no bile contamination or bleeding into the abdominal cavity during the operation.A hollow viscus injury manifesting with intra-luminal bleeding but no peritonitis or hemoperitoneum is an extremely rare condition.Retroperitoneal organ injuries resulting from a penetrating abdominal injury tend to be overlooked,as occurred in our case.This is why in the event of penetrating abdominal injuries it is important to perform a very careful abdominal exploration,including the Kocher maneuver.

Figure 1 Abdominal computed tomogrpahy.
Endoscopic closure of acute iatrogenic perforations using endoclips or a band ligator has been suggested[4,5].Per our previous report,EBL for an iatrogenic colon injury is a feasible and safe methodin vivo,and endoscopic EBL is an acceptable method to manage variceal bleeding[9].Endoscopic clipping for a hollow viscus perforation can be limited in cases with a large perforation or in those with tangential angles[4].In our case,the missed duodenal injury was accompanied by bleeding,and we closed the missed duodenal injury using EBL.
If a missed duodenal injury has already caused peritonitis,a surgical approach is required because a penetrating abdominal injury that accompanies a hollow viscus injury is an obvious surgical indication[10].In this case,a Levin tube was inserted to drain gastric and bile juice and to detect internal bleeding,and two JP drains were inserted in the paracolic gutter and pelvic cavity during the first operation to detect leakage or intra-abdominal bleeding.There was no evidence of internal or intraabdominal bleeding or leakageviathe Levin tube or JP drain,and there was no evidence of peritonitis.Thus,we attempted an endoscopic approach to diagnose the bleeding detected on the abdominal CT scan.
There has only been one previous report of endoscopic treatment of a penetrating abdominal injury,and that case was a penetrating gastric injury[7].There have been no reports on the endoscopic treatment of a traumatic duodenal perforation.Although our case is very rare and limited,it is the first successful endoscopic treatment for a missed duodenal injury found more than 24 h after surgery.
CONCLUSION
A penetrating hollow viscus injury is an indication for surgical treatment[11].Generally,endoscopic treatment is not indicated for hollow viscus injuries because of peritonitis,leakage,bleeding,and the length of endoscopy.In our experience,an endoscopic approach may be helpful in the event of a suspected duodenal injury.A very careful abdominal exploration,including the Kocher maneuver,is very important for an upper abdominal penetrating injury.
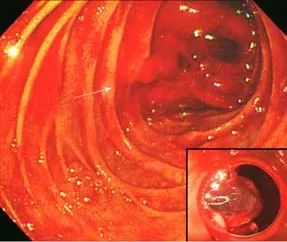
Figure 2 Endoscopy showed active bleeding with a perforation in the third portion of the duodenum.
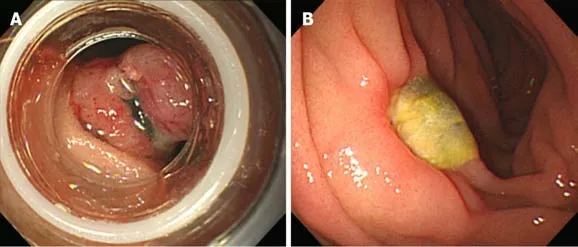
Figure 3 Endoscopy results.
 World Journal of Clinical Cases2019年20期
World Journal of Clinical Cases2019年20期
- World Journal of Clinical Cases的其它文章
- Clinical use of low-dose aspirin for elders and sensitive subjects
- Distribution and drug resistance of pathogenic bacteria in emergency patients
- Comparative analysis of robotic vs laparoscopic radical hysterectomy for cervical cancer
- Feasibility of laparoscopic isolated caudate lobe resection for rare hepatic mesenchymal neoplasms
- Soft tissue release combined with joint-sparing osteotomy for treatment of cavovarus foot deformity in older children:Analysis of 21 cases
- Clinical characteristics of sentinel polyps and their correlation with proximal colon cancer:A retrospective observational study