
Blood glucose control in the intensive care unit: Where is the data?
2019-02-27 04:58SebastianCasillasEdgarJaureguiSalimSuraniJosephVaron
World Journal of Meta-Analysis 2019年8期
Sebastian Casillas,Edgar Jauregui,Salim Surani,Joseph Varon
Abstract
Key words: Blood glucose control; Critical illness; Intensive care unit; Insulin therapy;Critical care
INTRODUCTION
Critically ill patients present a special challenge when dealing with glycemic control,as they require correcting hyperglycemia while avoiding hypoglycemia and keeping blood glucose (BG) at optimal levels.This can have significant repercussions on the prognosis of these patients[1].In the last 2 decades there have been a series of studies and added recommendations for glycemic control in the intensive care unit (ICU)setting[2-5].For example,Van den Bergheet al[2,3]conducted a study among patients in the surgical ICU,who were managed with a rigorous glucose control protocol(maintenance of BG between 80-110 mg/dL) versus conventional treatment (infusion of insulin if BG > 215 mg/dL).They showed an increased survival rate and better prognosis,overall decrease in the mortality rate by 34%,as well as by sepsis (46%),polyneuropathy (44%) acute kidney injury (41%),and a significant decrease in blood transfusion requirements (50%)[2].That particular study elicited some controversies,and additional randomized controlled trials were conducted.In 2009,the Normoglycemia in Intensive Care Evaluation-Survival Using Glucose Algorithm Regulation study (known by its acronym,NICE-SUGAR) revealed an increased mortality rate in those patients that underwent the tight glucose control (TGC) of 81-108 mg/dL,while moderate glucose control target of 140-180 mg/dL was associated with a higher survival rate[6].This multicenter study emphasized the significant risk of hypoglycemic episodes with TGC due its proximity to the lower limit of the BG levels and other similar studies followed[6-8].
Independent of diabetes mellitus,there are many other clinical scenarios that may cause alterations in BG level among critically ill patients,although diabetics are most susceptible to these alterations[9-11].Indeed,critically ill patients are usually admitted to the ICU with stress-induced hyperglycemia (50%-85%)[5,12].For that reason,it is important to identify adequate BG monitoring methods.Continuous BG monitoring would be ideal but can be complex to interpret and treat.Current glucose monitoring devices are rudimentary,and laboratory results may take longer periods of time[13].In this review,we present some aspects regarding the diagnosis,monitoring and management of glycemia in the ICU and discuss some of the newer technological advances that are at the forefront of continuous care of BG.
Complications
Hyperglycemia has been an important issue when dealing with glucose control in critically ill patients.Krinsleyet al[9]conducted a retrospective study evaluating 1826 patients admitted to the ICU and reported a significant increase in mortality related to glycemic levels,reaching 42.5% in patients with higher mean glucose levels (> 300 mg/dL).These results are consistent with those from other studies,which also have shown that hyperglycemia is a marker of mortality in the ICU[1,14].
Hypoglycemia,on the other hand,is also an important contributing factor for mortality in critically ill patients.Many trials have tested the effectiveness of TGC and have shown it to be a risk factor for developing hypoglycemia (BG < 40 mg/dL) as well as a powerful marker for mortality; it was also found to be superior to hyperglycemia[6-8,15].For example,hypoglycemia in intensive insulin therapy (IIT) was found to be 6-fold more common in patients with more liberal glycemic control[2,16].
MATERIALS AND METHODS
The authors independently searched an electronic database (PubMed?) using MeSH identifiers with the terms “blood glucose” and “intensive care unit” to identify articles published up to December 2018 with relevancy to glycemic care in the ICU.This search yielded 309 articles.Of those articles,after independent manual review,160 potential articles were identified and reviewed.As the topic of this search was narrowed to the care of the critically ill patients,only 49 articles were included in this review.Abstract-only,posters,duplicate information,comments and conference papers were excluded.All data acquired were discussed later between the authors,and any disagreements were resolved (Figure 1).
GUIDELINE RECOMMENDATIONS ON GLUCOSE CONTROL
Several different guidelines recommend certain parameters for glycemic control,with slight differences between the reference values,but a common denominator is the minimization of TGC.In 2011,the American College of Physicians recommended the use of the moderate range of 140-200 mg/dL and did not recommended TGC of 80-110 mg/dL,in order to avoid hypoglycemia and glucose variability (similar to the conclusive results from NICE-SUGAR)[17].The following year,the American Diabetes Association recommended a very similar glycemic control,ranging from 140-180 mg/dL[18].These recommendations are consistent with current critical care guidelines that support the use of insulin infusions in values that exceed 150 mg/dL,with the aim of maintaining a glycemia of 180 mg/dL in an attempt to avoid hypoglycemic episodes[19,20].The Society of Critical Care Medicine guidelines recommended to keep a BG between 150 mg/dL and 180 mg/dL[19].
Despite these recommendations,some studies have reported results that have different outcomes.For example,the COIITSS study investigators ran a multicenter randomized clinical trial involving 509 adult patients with septic shock,revealing no significant mortality difference in patients with a target BG of 80-110 mg/dL compared to those with a target BG of 150 mg/dL[21].
In many studies,preexisting diabetes mellitus has remained a significant cause for bias in terms of glucose management,as prior studies have shown variability in the response to therapy and different mortality from other patients in the ICU[10].These diabetic patients can develop resistance to glucose fluctuations and can actually benefit from higher BG ranges,avoiding BG variability and hypoglycemic episodes.Mariket al[22]suggested the necessary target BG ranges based on the hemoglobin A1c(referred to commonly as HbA1c; 160-220 mg/dL in patients with HbA1c > 7%,and 140-200 mg/dL in patients with HbA1c < 7%).Table 1 summarizes some of these guidelines and recommendations for critically ill patients.
INSULIN THERAPY IN CRITICALLY ILL PATIENTS AND NEWER TECHNOLOGIES FOR BG MONITORING
Prior to 2001,no randomized controlled trials had assessed specific BG targets among critically ill patients.More recently,a variety of studies have focused on management criteria for BG in critically ill patients via glycemic monitoring,use of IV insulin,and computerized processes.Krinsleyet al[23],in a study of 1600 critically ill patients managed with insulin therapy,reported a 75% reduction in acute kidney injury,19%decrease in the number of patients transfused with packed red blood cells,11%decrease in length of ICU stay,and a drop of 29% in mortality.This study aimed to decrease glucose levels to < 140 mg/dL with IIT.However,in a systematic review and meta-analysis by Mariket al[15]reviewing TGC (80-110 mg/dL) in ICU patients and including seven randomized controlled trials with more than 11000 patients,no reduction was found in 28-d mortality,blood stream infections,or requirement for renal replacement therapy.These investigators concluded that there is no evidence to support the use of IIT in ICU patients.These findings have since been replicated by other studies[3,24].In one such,continuous insulin infusion via central venous catheter led to hypoglycemia[24].
Other studies have shown less of a risk of hypoglycemia.In 2014,Amreinet al[25]conducted a nurse-driven trial with the Space Glucose Control System? involving 40 critically ill patients and utilizing a computer-assisted device combined with an infusion pump for glycemic control.The target values were set at 80-150 mg/dL and it was noted that the adherence to the given insulin dose advised by the computer program was 98.2%; only one severe hypoglycemic episode occurred (0.03% of glucose readings)[25].In a similar study of 210 patients in four different ICUs,monitoring BG was followed by management with a computerized insulin infusion program that had been programmed to a moderate glycemic range of 120-160 mg/dL in surgical ICUs and 140-180 mg/dL in medical ICUs[26].The mean BG was 147 mg/dL in the surgical ICUs and 171 mg/dL in the medical ICUs.Only 17% had one or more glycemic episodes between 60-79 mg/dL and 9.8% < 70 mg/dL[26].
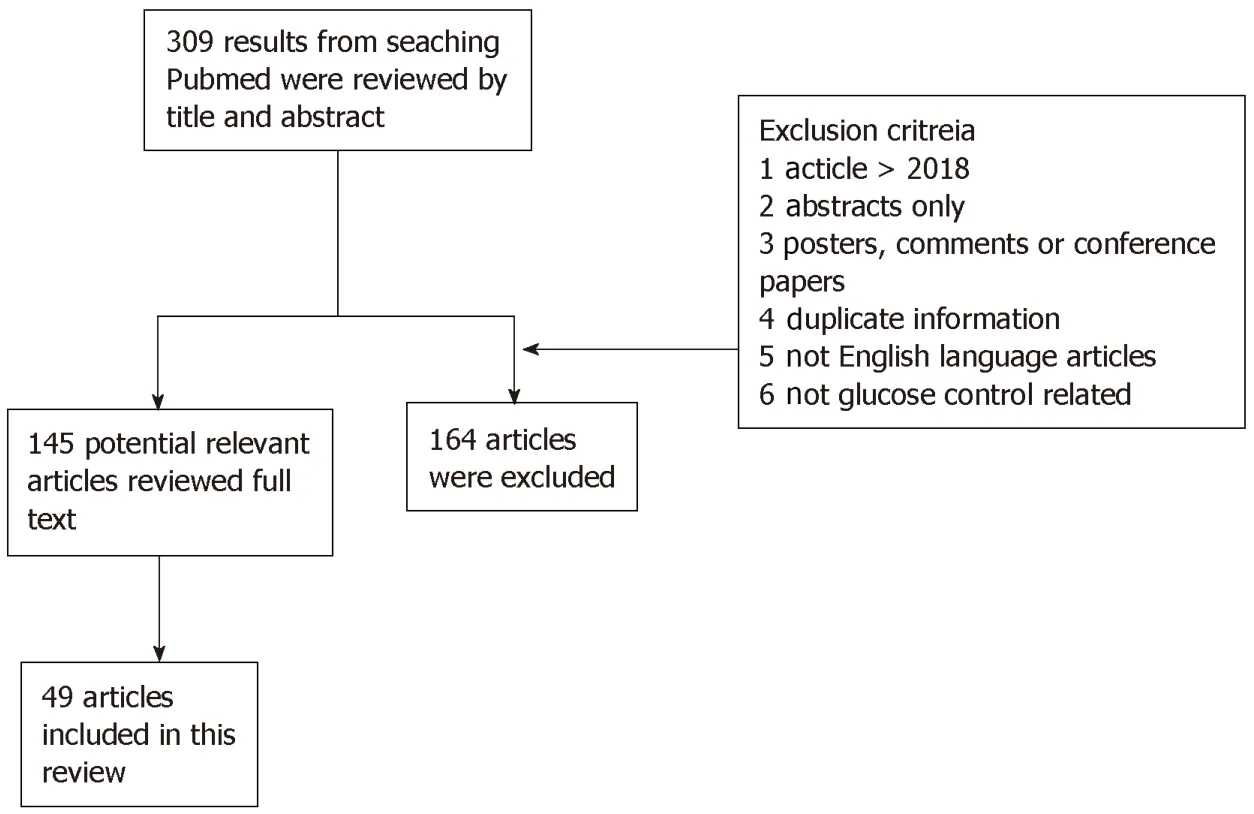
Figure1 Flowchart describing the methodology for this review.
The Food and Drug Administration (commonly known as the FDA),in 2014,recommended that the use of point-of-care (POC) BG monitors were not suitable for critically ill patients[27].In addition,the Centers for Medicare and Medicaid Services indicated that “off-label” use of such glucometers in the ICU could be subject to citations and fines during site evaluations[28].The main reasons for the FDA and Centers for Medicare and Medicaid Services concerns was that ICU patients are unstable and that might cause erroneous BG readings.
In general,POC glucose monitors cost less,require smaller blood samples,and provide almost instant results.For years,they have been the preferred bedside glucose monitoring devices for glycemic management[29].In a study of a large academic hospital,POC showed significant accuracy[30].Results from glycemic POC paired to results of central laboratory testing of samples drawn no more than 60 min and passed the FDA's 98% criteria[30].
New software incorporating current guidelines may be just as beneficial for glycemia control[31].Some studies have used the Clinical Notification System that relies on specific criteria and notifies nursing staff of imminent hypoglycemia and persistent hyperglycemia,defined as two consecutive readings > 150 mg/dL[32,33].The sensitivity and specificity of this system are excellent,being 98.1% and 99.1%respectively[32,33].
Continuous BG monitoring is now available[34-36].In a single-center study comparing the benefits of continuous with intermittent glucose monitoring,a peripheral venous catheter was inserted with the GlucoClear? probe[35].These monitors were flushed with heparin,calibrated,and began BG monitoring every 5 min using a glucose oxidase-based method.Target glycemic ranges for this study were between 90-150 mg/dL.The number of patients with BG < 70 mg/dL in continuous versus the intermittent groups was 8/39 (20.5%) and 15/38 (39.5%) respectively.The time spent with BG < 70 mg/dL was calculated with a continuous glucose monitoring device,and resulted in 0.4% + -0.9% versus 1.6%+ -3.4% (P< 0.05) in intermittent glucose monitoring group[35].
In a study by Floweret al[36],utilizing a novel intravascular continuous glucose monitoring with chemical fluorescence sensing mechanism,92.4% (404/437) were in target glycemic control (108-180 mg/dL),with no values < 72 mg/dL.
There are now subcutaneous continuous glucose monitoring sensors in case intravenous access is not available[37].In a small cohort of 14 surgical ICU patients,the Sentrino continuous glucose monitoring glucometer (Medtronic,Dublin,Ireland) was used[38].The study showed that the sensor provided good accuracy,overestimating glycemia by only 1.5 mg/dL[38].
BG CONTROL IN DIABETIC PATIENTS IN THE ICU
The glycemic control protocols vary among different institutions and according to whether the patient has preexisting diabetes mellitus or not.The effects of IIT,for example,have been more noticeable in nondiabetic critical patients[39,40].In one study,the mortality rates for nondiabetic patients undergoing IIT was 36.8%,as compared to40.9% in the control group[39].In addition,when compared to patients with diabetes,the interventional group mortality was 39.6% versus 36.8% in the diabetic group[39].In fact,some authors have also suggested that diabetes may be “protective” in the ICU[40].
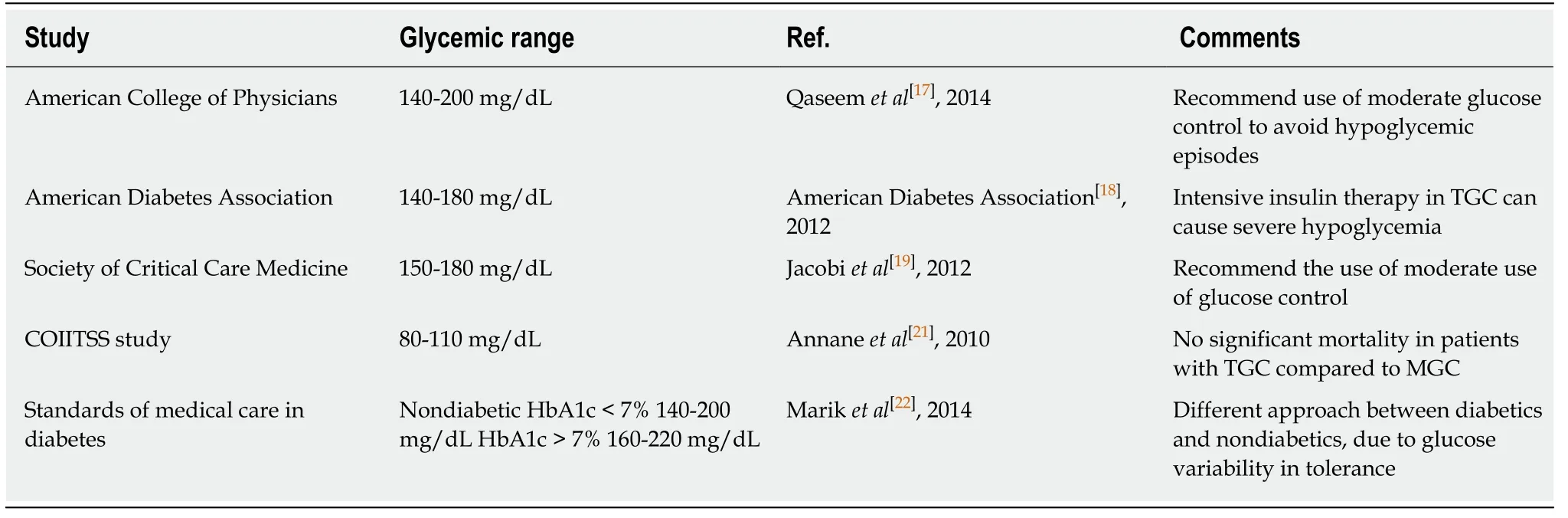
Table1 Glycemic range recommendations
Mortality is lower for the ICU diabetic population when it comes to hyperglycemia and glucose variability,as compared to nondiabetics.However,hypoglycemia and severe hypoglycemia have an equal mortality rate for both types of patients[10,41].In a study evaluating both nondiabetic patients and diabetic patients with tight and moderate glycemic control (80-110 mg/dL and 90-140 mg/dL),nondiabetic mortality was 11.9% in the moderate glycemic control group when compared to 8.1% in the TGC group[42].In contrast,patients with diabetes had a 12.3% mortality with TGC compared to 9.8% for the moderate glycemic control group[42].
COST-EFFECTIVENESS
Cost analysis in the ICU remains an important topic.In one study,an economic analysis reported a cost-saving of 2638 Euros per patient in the group that was treated with intensive glycemic control[43].Some have suggested that blood gas analyzers capable of monitoring continuous BG levels are the best option for accuracy and costsaving,if they are in proximity to the ICU,even when the cost per device is $40000.The single test cost is very similar to a POC meter ($100) and the accuracy is equal to a central laboratory device[44].It is clear that euglycemia and avoidance of hypoglycemia decreases the length of stay in the hospital (from 29 d to 24 d) and has a lower healthcare cost (mean $5847),showing a notable amount of money-saving in 5 d[45].
Another factor to consider when analyzing cost savings is the role of TGC in reducing blood stream infections.Some studies have reported that decreasing 5% of hospital-acquired infections could improve cost savings considerably; in fact,one of these studies showed a cost-saving of $1580 per patient,driven by the decreased length of stay in the ICU[46,47].Such goals can be achieved by attempting to control BG with avoidance of hypoglycemia.
FUTURE APPROACHES
As noted above,dysregulation of glycemia is a significant factor in the poor prognosis of an ICU patient[48].There are other contributing factors that can change the glycemic status,such as age (older),underweight condition,and type of feeding that is managed in the ICU,since these are labile and can create fluctuations in a more noticeable way compared with the rest of the patients.Critical care clinicians may not be fully aware of these findings.Indeed,some survey studies have shown that clinicians vary significantly in how they manage glycemic index in the ICU and very few are aware that hypoglycemia is associated with an increased hospital mortality[49].Educational programs aimed at understanding these important risk factors are needed.The development of professional awareness of current guidelines and introduction of new technologies are the first step for improving patient care outcomes.
We believe that computerized,protocol-driven and continuous BG monitoring will become the standard of care in ICUs across the world.
 World Journal of Meta-Analysis2019年8期
World Journal of Meta-Analysis2019年8期
- World Journal of Meta-Analysis的其它文章
- Antidiabetic agents in patients with hepatic impairment