
Therapeutic effect of different treatment methods on functional anorectal pain
2018-12-13 01:08:06HuaJuanLiZhiJunWeiXiHuaWu
TMR Non-Drug Therapy 2018年4期
Hua-Juan Li,Zhi-Jun Wei,Xi-Hua Wu
1Shenzhen Traditional Chinese Medicine Hospital,Shenzhen,China.2The Fourth Clinical Medical College of Guangzhou University of Chinese Medicine,Shenzhen,China.
Introduction
Functional anorectal pain(FAP)is a nonorganic disorder of the anorectal.Its clinical manifestations are severe,and dull pain of the anus occurs intermittently or frequently.The sensation of pressure in the rectum is likely to increase and is exacerbated by changes in body position.MostpatientswithFAPexperiencedifficultyin defecation,tenesmus,a burning feeling inside the anal canal,and other symptoms.The pathogenesis of FAP is unclear;it can be divided into levator ani syndrome,spasmodic anal pain,and nonspecific anal pain[1].An epidemiological study reported that the morbidity due to FAP is 7.7%and increases yearly[2].FAP is one of the most difficult problems to treat for proctologists.
According to ancient documents,FAP belongs to procto pain disorders in traditional Chinese medicine(TCM).Huangdineijing(B.C.220-211,Han Dynasty)said that the internal organs are closely related to the procto,and feces cannot stay in the gut for a long time.Treatmentofanorectaldiseaseswithenemaand fumigation has been recorded in ancient documents:Shanghanlun(A.D.150-229,late Eastern Han Dynasty)documented the use of pig gallbladder,Fanxieye(Cassia Angustifolia)extract,andclearvinegarasenema solutions;Bencaogangmu(A.D.1578,Ming Dynasty)recorded that flushing the intestines with water and scallion juice could promote smooth fecal excretion.In modern medicine,the drug treatment methods for FAP mainly include nerve blocking,botulinum toxin injections,oralTCM,hipbath,andenema[3-5].Non-drug treatments such as biological feedback,psychotherapy,and acupuncture could enhance the curative effect of drug treatment,suggesting the combination therapy may have more advantages than single treatment[6-8].In this study,the clinical efficacy of oral TCM(Jiaweitiaoqi decoction),electroacupuncture,biofeedback training,and combined treatment of FAP were observed.
Materials and method
General information
A total of 200 patients with FAP were randomly divided into 4 groups,with 50 patients in each group,from June 2015 to September 2018.These 4 groups were treated with oral Jiaweitiaoqi decoction,electroacupuncture at Shu points of the lumbosacral portion,biofeedback training,and a combination of the 3 methods,respectively.The numeric rating scale(NRS),Short Form-36(SF-36)quality of life scale,static pressure of the anal canal,and maximum systolic pressure were recorded in the 4 groups.
Diagnostic criteria
According to the Rome III criteria for gastrointestinal illness,the following symptoms were considered to indicate FAP in this study:(1)chronic or recurrent anorectal pain;(2)pain attack at any time or sustained pain attack lasting at least 20 min/day;(3)absence of other reasons to explain the anorectal pain;and(4)all of the previous symptoms occurring discontinuously or persistently from at least 3 months before the study[9].
Inclusion criteria
(1)The diagnostic criteria of FAP were met;(2)the patient voluntarily participated to receive treatment and signed the informed consent form.
Exclusion criteria
(1)The pain was caused by anorectal parenchymal lesions such as mixed hemorrhoids,anal sinusitis,and perianalabscess;(2)therewasco-occurrenceof cardiovascular,cerebrovascular,hematopoietic system,and other serious diseases,as well as mental diseases;(3)the patient was receiving medical treatment for other diseases while on medication;(4)the female patient was pregnant or a patient had terminal disease;(5)the patient failed to complete the study procedures and observation cycles for other reasons.
Therapeutic methods
(1)Oral Jiaweitiaoqi decoction group.The composition of the Jiaweitiaoqi decoction was as follows:Baishao(Radixpaeoniaealba),30g;Huangqin(Radix scutellariae),9 g;Danggui(Radix angelicae sinensis),10 g;Rougui(Cinnamomum cassia),3 g;Binlang(Areca catechu),10 g;Zhigancao(Radix liquiritiae),10 g;Muxiang(Radix aucklandiae),10 g;Jiudahuang(Radix et rhizoma rhei),3 g;Jinyinhua(Lonicera),20 g;Shengma(Cimicifuga dahurica),10 g;and Niuxi(Achyranthus bidentata blume),10 g.The ingredients were boiled in 200 mL water and the decoction was taken twice in the morning and evening.(2)Electroacupuncture group.The electroacupunctureneedleswereinsertedintothe Dachangshu(BL25),Shenshu(BL23),Ciliao(BL32),andXialiao(BL34)points.Theelectroacupuncture apparatus was linked to the patient and the dilatational wave was chosen,with the intensity appropriate for the patient's comfort level and the needles were kept for 20 min,once a day.(3)Biofeedback training group.The patients followed the guidance of professional physicians,and performed regular inhalation with rectal contraction and exhalation with dilatation,contraction,and dilatation for 5 s each.Each training session lasted for 20 min,once a day.(4)Combination treatment group.All of the above 3 treatment methods were used in combination,with the same protocols.All 4 groups underwent 1 course of treatment for 7 days,and the treatment efficacy was evaluated after 2 courses of treatment.
Treatment assessment
(1)NRS.The NRS provides a range of scores from 0 to 10 and can be used in the assessment of curative effect by comparing the scores before and after treatment.The followingcutoffpointsintheNRShavebeen recommended:no pain(score:0),mild pain(score:1-3),moderate pain(score:4-6),severe pain(score:7-9,including inability to sleep or sleep interruption by pain),and sharp pain(score:10)[10].
(2)SF-36 quality of life score.This scale has a total of 8 dimensions,and each dimension includes 100 scales comprising role-physical,physiological function,vitality,bodily pain,role-emotional,general health,mental health,social function,and others.Among them,the mental health component score(MCS)is the average of social function,vitality,mental health,and role-emotional,whereas the physiological health component score(PCS)is the average of role-physical,physiological function,general health,and bodily pain.MCS and PCS were used ascontrolstandards,andthescorewasdirectly proportional to the life quality.
(3)An anorectal manometer from Medtronic Functional Diagnostic(Denmark)was used.The static pressure and maximum systolic pressure of the anal canal of the 4 groups were recorded before and after treatment.
Statistical methods
In this study,all collected data were statistically analyzed usingtheSPSS20.0statisticalsoftware.The measurement data were denoted as(?x±s).T-test was used for analysis of intergroup differences,and analysis of variance was used for comparison among groups.All test results were evaluated withP<0.05 as a criterion for determining whether there was a significant difference.
Results
Comparison of baseline data
There were 21 male and 29 female patients in the Chinese medicine group,ranging in age from 22 to 71 years,with an average of 32.3±4.2 years.The course of disease was 1-10 years,with an average of 5.4±1.2 years.There were 19 male and 31 female patients in the electroacupuncture group,ranging in age from 20 to 69 years,with an average of 32.8±8.1 years.The course of disease was 0.5-13 years,with an average of 6.7±2.5 years.There were 22 male and 28 female patients in the biofeedback training group,ranging in age from 23 to 69 years,with an average of 35.3±6.2 years.The course of disease was 0.5-9 years,with an average of 4.6±2.1 years.There were 18 male and 32 female patients in the combination treatment group,ranging in age from 25 to 73 years,with an average of 37.5±3.2 years.The course of disease was 1-13 years,with an average of 5.1±3.2 years.There were no statistically significant differences in age,the courses of the disease,and sex distribution among the 4 groups.
Comparison of index results
The observation indices of the 4 groups were all improved compared with those before treatment,with the combination treatment group showing the most obvious improvement.The combination treatment group had lower values than the other 3 groups in the NRS score,anal static pressure,and maximum systolic pressure.In the SF-36 quality of life score,the combination treatment group had higher values than the other 3 groups.The difference was statistically significant(P<0.05)(Tables 1-3).

Table 1 Comparison of NRS scale scores
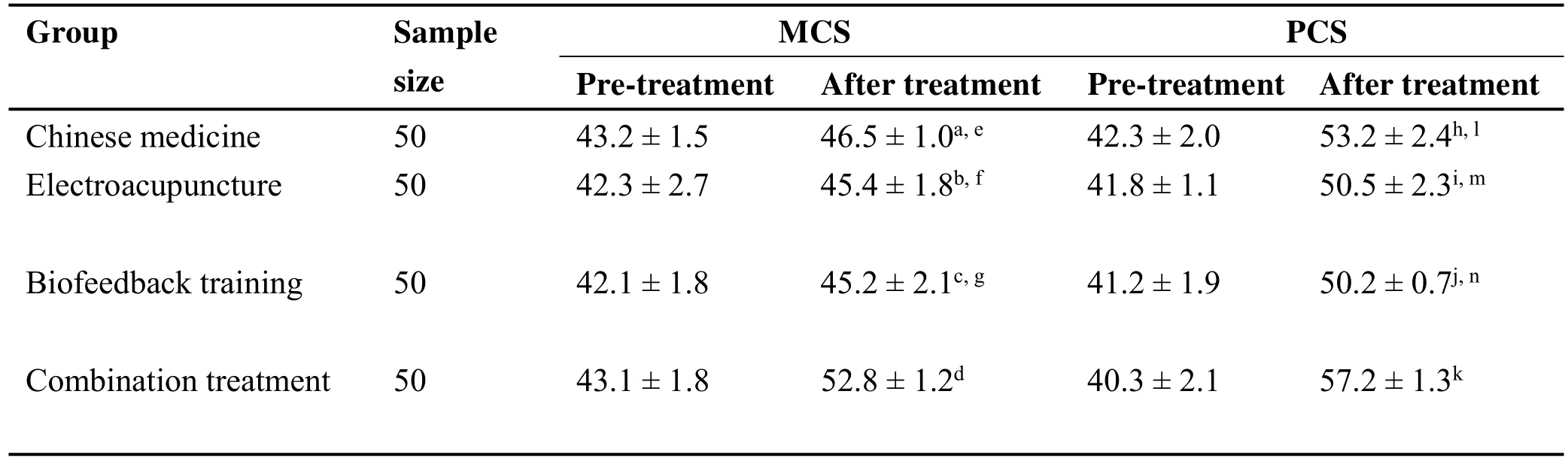
Table 2 Comparison of SF-36 scale scores
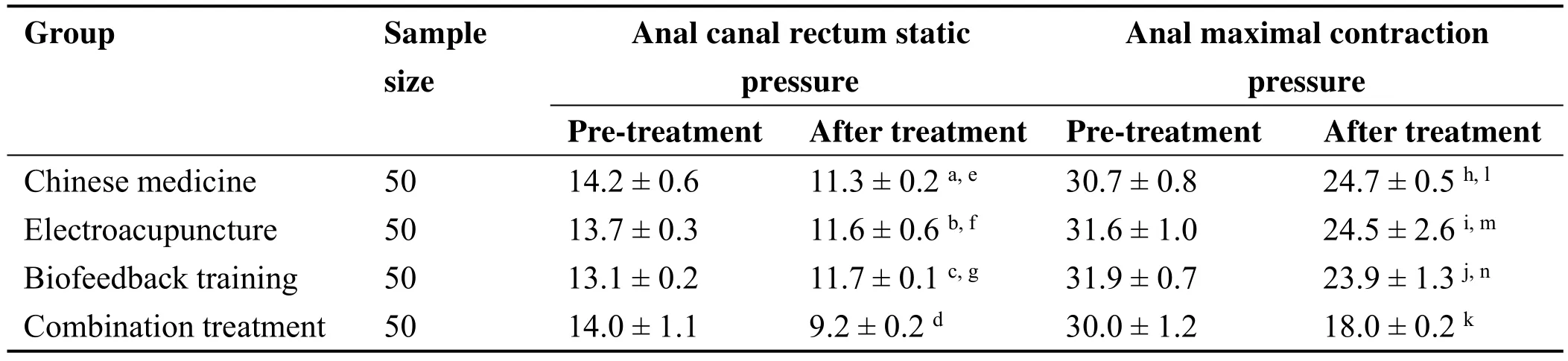
Table 3 Comparison of anal canal rectum static pressure and anal maximal contraction pressure
Discussion
The pathogenesis of FAP is unclear,and most researchers considerthatFAP-relatedpainisassociatedwith excessivecontractionofthepelvicfloormuscle.Increased contraction frequency can cause pelvic floor nerve and blood vessel compression;therefore,the pelvic floor blood flow is blocked,and local hypoxia occurs[12,13].In turn,the pain can increase the psychological burden on patients,form a vicious circle,and gradually aggravate the illness.An effective analgesic treatment could help the patient by reducing anxiety and stress,and is helpful in improving clinical performance and relieving psychological pressure as soon as possible[14].However,because of the long disease course,recurrence easily occurs and there are no specific treatments for FAP at present;oral medication alone and topical medication have not been effective[15,16].Therefore,physical therapy,biofeedback therapy,acupuncture,and other non-drug treatment methods are expected to enhance the efficacy of drug treatment.
Currently,biofeedback is a popular treatment for FAP.The American Academy of Colorectal Surgeons Clinical Guidelines for the diagnosis and treatment of constipation point out that biofeedback is the first-line treatment for pelvic floor dysfunction[17].Chiarioniet al.applied biofeedback,electric stimulation and massage,and warm water bath for the treatment of FAP.Their results showed thatbiofeedbackcouldalleviateFAPbetter[18].Biofeedback can alleviate pain by improving the function of relaxation and contraction as well as the coordination of pelvic floor muscle[19].Biofeedback treatment usually has 3 forms:electrical stimulation,Kegel training,and neuromuscular electrical stimulation.Kegel training has shown better patient compliance than the other 2 forms,and costs less than the others.Studies have also shown that Kegel training is a safe,effective,and convenient method for the treatment of pelvic floor diseases.
A study has shown that FAP is closely related to the channels of meridians of the bladder and the Du meridian,and electroacupuncture has been widely used in the treatment of FAP[28].The large intestine is the back Shu point of the Yangming meridian,which could be used in the treatment of diseases of the large intestine.Ciliao(BL31)and Xialiao(BL34)belong to the category of Baliao points.Suwen(B.C.220-211,Han Dynasty)documented that for lumbago involving the scrotum,acupuncture at the Baliao and Ashi points could lead to pain remission.Shengyuge(A.D.1601,Ming Dynasty)said that a person with lumbago and frequent micturition could be treated using the kidney Shu points on both sides of Du meridian.Modern medical research has shown that the Ciliao(BL31)and Xialiao(BL34)points near the defecation center of the pelvic nerve(S1-S4).The anal shrinkage and the supportive feeling of the perineum via stimulating S4 are similar to those of acupuncture at Ciliao(BL31)andXialiao(BL34).Therefore,acupuncture at the Ciliao(BL31)and Xialiao(BL34)points could regulate the related channels and the status of pelvic floor spasm[4].The L1 segment of afferent nerves under the Shenshu(BL23)points entering spinal cordoverlapwiththeT12-L1segmentofnervi hypogastricusenteringthespinalcord,indicating acupuncture at the Shenshu(BL23)points can treat diseases of the abdominal organs and pelvic cavity[29].Stimulation of the Shu points of the large intestine has a regulating and analgesic effect on autonomic and somatic nervefunctions,achievingtheantispasmodicand analgesiceffects[30].Furthermore,applicationof alternatecondensation-rarefactionwavesduring electroacupuncture can reduce the stress function of the meridian,relieve muscle spasm,and achieve pain relief.
The disease duration of FAP belongs to the Yangming meridian,whichisrichinQiandblood.Jingyuequanshu·Zhongzhang(A.D.1368~1644,Ming Dynasty)said that the block of Qi could result in the occurrence of blood stasis and then lead to these uncomfortable feeling such as pain and sagging distention.Therefore,treatment of FAP focuses on the regulation of Qi and blood.In the prescription of the Jiaweitiaoqi decoction,Shengma(Cimicifugadahurica),Niuxi(Achyranthusbidentatablume),Danggui(Radix angelicae sinensis),Muxiang(Radix aucklandiae),and Binlang(Areca catechu)regulate Qi and blood;and Huangqin(Radix scutellariae)and Jinyinhua(Lonicera)clear away heat and toxic material.Shishimilu(A.D.1600-1700,late Ming and early Qing Dynasty)pointed out that the painful disease belongs to the liver,and considered that the pathogenesis of FAP is stagnation of the liver Qi[20].Baishao(Radix paeoniae alba)smooth the Qi of liver and compatibility with Danggui(Radix angelicae sinensis)and Zhigancao(Radix liquiritiae)can enrich blood and relieve pain.Rougui(Cinnamomum cassia)and Jiudahuang(Radix et rhizoma rhei)regulate the cold and heat.In summary,the characteristic of this decoction is regulation of cold,heat,Qi and blood.Modern pharmacology shows that total glycosides of Baishao(Radix paeoniae alba)can decrease the levels of C-reactive protein,interleukin-6,and interleukin-β,but enhance the secretion of the inflammatory cytokine interleukin-10,consequently inhibiting the inflammatory response[21].Danggui(Radix angelicae sinensis)can play a role in human T lymphocyte activation,induction of interferon activity,and acceleration of interleukin-2 production,as well as provide anti-inflammatory and analgesiceffects[22].Jinyinhua(Lonicera)and Jiudahuang(Radix rhizoma rhei)have anti-inflammatory,anti-bacterial,and anti-ulcer effects[23-25].Huangqin(Radix scutellariae)and Rougui(Cinnamomum cassia)havepharmacologicalactivities,includingantiinflammatory,anti-ulcer,and anti-ischemia/reperfusion injury and immunity regulation activities;they also provide a modern pharmacological basis for the treatment of FAP[26,27].This study applied Chinese medicine,electroacupuncture,biofeedbacktreatment,andthe combination of the 3 methods for the treatment of FAP,andrevealedthatnondrugtherapysuchas electroacupunctureandbiofeedbacktreatmentcould enhance the curative effect of single Chinese medicine on FAP.
Conclusion
These results show that non-drug therapy,including acupuncture and physical exercise,can enhance the clinical efficacy of single Chinese medicine in the treatment of FAP.A combination of Chinese and Western medicines and multidisciplinary diagnosis and treatment should be applied in the clinical setting.It is best not to delay the cure by using a single treatment.
:
1.Rao SSC,Bharucha AE,Chiarion G,et al.Anorectal disorders.Gastroenterology 2016,150:1430.
2.Boyce PM,Talley NJ,Burke C,et al.Epidemiology of the functional gastrointestinal disorders diagnosed accordingtoRomeⅡcriteria:anAustralian population-based study.Internal Med J 2006,36:28-36.
3.JiX,WangJM,HouY.30casesof electroacupuncture combined with Dangguishaoyao powder treated with functional anorectal pain.J Jiangxi University Tradit Chin med 2018,30:59-61.
4.Xue YH.Literature review and clinical study on the randomized controlled trial of acupuncture for the treatment of functional anorectal pain.Nanjing Chin Med 2017.
5.Ye YF,Xu HY.Clinical observation on functional anorectal pain treated by retention enema and fumigation with Sihuangqudu decoction.Chin J Tradit Chin Med 2018,33:1181-1183.
6.Zhang DJ,Lan J,Zong Y,et al.Clinical study on the treatment of chronic anorectal pain by biofeedback combined with psychological intervention.Chin J Integr Tradit Chin Western Med 2015,23:531-533.
7.Yu YD,Yi LH,Yao QY,et al.Efficacy evaluation of electroacupuncture combined with biofeedback in the treatment of functional anorectal pain.China Tradit Chin Med 2016,23:696-697.
8.Chen ZY,Liu CB.Observation of 50 cases of pelvic floorspasmsyndrometreatedbyacupuncture combinedwithbiofeedbacktraining.ChinJ Clinicians 2015,43:43-46.
9.Bharucha AE,Wald A,Enck P,et al.Functional anorectal disorders.Gastroenterology 2006,130:1510-1518.
10.Yan GB.NRS pain digital rating scale.Chin J Joint Surgery 2014,8:410.
11.Zhang Y,Wu YX,Qu B,et al.Application of SF-36 scale in life quality evaluation of medical students.Chin J Health Statistics 2013,30:468-469.
12.Shen BH,Zhao XL,Guo XT.The treatment of functional anorectal pain.Acute disease Chin Tradit Med 2016,25:1740-1742.
13.Baranowski AP,Abrams P,Fall M.Urogenital pain in clinical practice.NewYork:Informa Healthcare USA,Inc,2008.
14.Ding YJ,Ding SQ,Lu T,et al.Analysis of clinical experience in the treatment of anorectal pain.J Jiangsu Tradit Chin Med 2015,47:1-3.
15.Wei ZJ,Wu XH,Wang Y,et al.Clinical observation oftreatingfunctionalanorectalpainby Shengdupingmu decoction.J China Med Pharmacy 2018,8,65-67.
16.GaryKA,AmnaSL,CarolynneJA.Patient characteristics and treatment outcome in functionl anorectal pain.Diseases Colon Rectum 2011,54:870-875.
17.Paquette I,Varam M,Tement C,et al.American society of colon and rectal surgeons clinical practice guideline for the evaluation and management of constipation.Dis Colon Rectum 2016,59:479-492.
18.Chiarioni G,Nardo A,Vantini I,et al.Biofeedback issuperiortoelectrogalvanicstimulationand massage for treatment of levator ani syndrome.Gastroenterology 2010,138:1321-1329.
19.Huang H,Ji LJ,Weng LP.Clinical study on the treatmentoffunctionalanorectalpainby biofeedbackcombinedwithpsychological counseling.J colorectal anal surgery 2014,20:94-96.
20.Zheng CJ,Wang YH.Discussion on the treatment of functional anorectal pain from liver.Hebei J TCM 2014,36:1555-1556.
21.WangXG.Inhibitionofoxidativestressand inflammatoryresponseinatherosclerosisrats.Practical Pharmacy Clinical Remedies 2017,20:140-143.
22.Zhu SQ,Guo S,Qian DW,et al.Study on modern drying and processing methods of angelica sinensis based on multiple functional ingredients.Chin J Tradit Chin Med 2017,42:264-273.
23.Chen JM,Hong CQ.Analysis of pharmacological action of flos lonicerae.Asia-Pacific Tradit Med 2015,11:34-37.
24.Song YL,Wang HM,Ni FY,et al.Study on phenolic acids and their anti-inflammatory activities in flos lonicerae.Chin Herbal Med 2015,46:490-495.
25.Wei JC,Chen Y,Xie Z,et al.Advances in chemical constituents and pharmacodynamics of rhubarb.J China Pharm 2017,28,3569-3574.
26.Wang HY,Yan YL,Chen PP,et al.Study on the screeningofeffectivecomponentsofbaicalin antipyretic and anti-inflammatory effects.J Harbin commercial university 2016,32:542-545.
27.Chen X,Liu C,Ma NH,et al.Advances in chemical composition,pharmacologicalactionand comprehensive application of cinnamon.J China Pharm 2018,29,2581-2584.
28.Cai LQ,Huang H,Chi W,et al.Electroacupuncture was used to treat 35 cases of functional anorectal pain.Chin Acupunc Moxibustion 2016,36:41-42.
29.Lu ZJ.Analysis on the clinical application of Shenshu point.China J Basic Med Tradit Chin Med 2012,18:432-436.
30.Ma WD.Probing into the needling technique and mechanism of Dachang shu point.2011 annual symposium of Chinese acupuncture and moxibustion society,2011.
- TMR Non-Drug Therapy的其它文章
- Fire needle combined with blood-letting therapy for a case of 20-year trigeminal neuralgia
- Clinical observation of the effect of acupuncture on constipation after stroke
- Effects of acupoint embedding combined with clomiphene in patients with polycystic ovary syndrome:a randomized controlled trial
- The role of acupoint embedding combined with clomiphene in the treatment of polycystic ovary syndrome
- A review of the treatment of cerebral palsy in children