
Injury of the arcuate fasciculus in a patient with progressive bulbar palsy
2017-01-21 03:33:18MinCheolChang,HanDoLee,SungHoJang
中國神經再生研究(英文版) 2016年12期
Injury of the arcuate fasciculus in a patient with progressive bulbar palsy
The arcuate fasciculus is the neural tract connecting the two major speech centers (Broca’s and Wernicke’s areas) and plays a critical role in language function (Catani and Mesulam, 2008). Injury of this tract can lead to several types of language impairment, including conduction aphasia, Broca’s aphasia, anomic aphasia, and apraxia of speech (Anderson et al., 1999; Bartha and Benke, 2003; Catani and Mesulam, 2008; Bernal and Ardila, 2009; Kim et al., 2011).
Motor neuron diseases (MNDs) are a group of neurological disorders characterized by progressive degeneration of upper motor neurons originating in the motor and premotor cortex, and lower motor neurons originating in the spinal cord and brain stem. MNDs include primary lateral sclerosis (selectively afecting upper motor neurons), progressive muscular atrophy (exclusively causing damage to lower motor neurons), amyotrophic lateral sclerosis (involving both upper motor neurons and lower motor neurons), and progressive bulbar palsy (primarily involving motor neurons in the brain stem) (Adams et al., 1997). As a result of damage to motor neurons, patients with MNDs present with muscle weakness, atrophy, and fasciculation throughout the body (Adams et al., 1997).
MNDs are known to predominantly affect motor function. However, recent studies have reported accompanying extra-motor manifestations, including aphasia, in patients with MNDs (Caselli et al., 1993, 2004; Tsuchiya et al., 2000; Bak et al., 2001; da Rocha et al., 2007), although the prevalence of the co-occurrence of motor dysfunction and extra-motor symptoms has not been clarifed. The pathogenic mechanisms of aphasia in patients with MNDs have been reported to be the result of atrophy or hypo-perfusion in the fronto-temporal lobe, which has been demonstrated using conventional brain CT/MRI, radionuclide imaging, and post-mortem brain autopsy (Tsuchiya et al., 2000; Bak et al., 2001; Catani et al., 2004; da Rocha et al., 2007). However, these methods are limited in that they cannot demonstrate lesions of neural tracts. By contrast, the recently developed difusion tensor tractography (DTT), which is derived from difusion tensor imaging (DTI), has enabled three-dimensional visualization and detailed estimation of neural tracts (Jang et al., 2013a, b). Several studies have demonstrated the degeneration of neural tracts using DTI, including the corticospinal tract, corpus callosal fbers, and uncinated fasciculus in patients with MNDs (Sage et al., 2007; Hong et al., 2008; Ben Bashat et al., 2011; Sarro et al., 2011; van der Graaf et al., 2011; Zhang et al., 2011). However, little is known about injury of the arcuate fasciculus.
The classic MND is characterized by progressive loss of limb, bulbar, and respiratory muscle function caused by selective degeneration of upper motor neurons and lower motor neurons, sparing the rest of the nervous system (Brooks, 1994). Accordingly, most previous DTI studies on patients with MNDs have focused on the corticospinal tract, demonstrating the correlation of injury of the corticospinal tract with deterioration of motor function (Sage et al., 2007; Hong et al., 2008; Zhang et al., 2011). Regarding aphasia in patients with MNDs, since the study reported by Caselli in 1993, several studies have reported non-fluent aphasia in patients with MNDs (Caselli et al., 1993; Tsuchiya et al., 2000; Bak et al., 2001; Catani et al., 2004; da Rocha et al., 2007). In those previous studies, atrophy and hypo-perfusion in the left fronto-temporal lobe were consistently observed on conventional CT/MRI and radionuclide imaging, respectively (Tsuchiya et al., 2000; Bak et al., 2001; Catani et al., 2004; da Rocha et al., 2007). In addition, in postmortem examination, the most common fndings were atrophy and neuronal loss in the leTh fronto-temporal lobe (Caselli et al., 1993, 2004; Bak et al., 2001; da Rocha et al., 2007). However, so far, no study evaluating the arcuate fasciculus in MND patients with aphasia using DTI has been reported. Therefore, this is the frst study using DTT to demonstrate injury of the leTh arcuate fasciculus in an MND patient.
In the current study, using the confguration and parameters of DTT, we attempted to demonstrate damage of the arcuate fasciculus in a patient with progressive bulbar palsy who presented with Broca’s aphasia.
A 74-year-old right-handed man visited the rehabilitation department of a university hospital for evaluation of language disturbance and dysphasia. He had no family history of neurological disease. Five years ago, the patient had begun to notice slurred speech, which had shown slow deterioration with time. One year ago, he had begun to show dysphagia (coughing during eating or drinking, difculty in chewing and controlling food in the mouth, and drooling of saliva). On neurological examination, he was alert and oriented. He exhibited decreased gag reflex and soft palatal movements, and the jaw jerk refex and tongue fasciculation were observed. In addition, he had mild quadriparesis (4/5 in the right upper and lower extremities and 4+/5 in the left upper and lower extremities on the Medical Research Council Scale (Council, 1976)). The deep tendon refex was signifcantly increased, particularly in the leTh upper and lower extremities. He showed a full score of 30 points on the Mini-Mental Status Examination for evaluation of cognitive function (Han et al., 2008). Conventional brain MRI and electromyography/nerve conduction studies revealed no abnormal findings (Figure 1A). The patient showed dysarthria (articulatory errors at sentence level: 30.1%) on the language function test, and Broca’s aphasia (aphasia quotient: 74%ile, fuency: 61%ile, comprehension: 86%ile, repetition: 71%ile, naming: 86%ile) on the Korean-Western Aphasia Battery (K-WAB) (Kim and Na, 2004). As a result, based on the patient’s history and neurological examination, he was diagnosed as progressive bulbar palsy. This study was approved by our hospital review board.
DTI data were acquired at 5 years aTher symptom onset using a 6-channel head coil on a 1.5 T. Sixty contiguous slices (reconstruction matrix = 192 × 192; feld of view = 240 × 240 mm2; echo time = 76 ms, b = 1,000 mm2/s, number of excitations = 1, thickness = 2.5 mm) were acquired for each of the 32 noncollinear difusion-sensitizing gradients. DTI-Studio soThware was used for reconstruction of the arcuate fasciculus. Based on the method of Nucifora et al. (2005), we placed the region of interest (ROI) for tracking of the arcuate fasciculus (the seed ROI in the posterior parietal area of the superior longitudinal fascicle and the target ROI in the posterior temporal lobe). The seed ROI was shown in green and the target ROI was shown in blue on DTI-based color-coded maps. Termination criteria used for fiber tracking were fractional anisotropy< 0.2 and angle < 60° (Jang and Lee, 2014). On DTT images, the arcuate fasciculus in the right hemisphere of the patient originated from Wernicke’s area, passed through the known arcuate fasciculus pathway, and then entered into Broca’s area (Figure 1B). Also, we recruited an age- and sex-matched normal subject (72 years old, male) with no history of neurological or psychiatric diseases. The DTT of the normal subject showed well-preserved bilateral arcuate fasciculus, passing through its known pathway.
In the current study, using the confguration and parameters of DTT, we found discontinuation of the leTh arcuate fasciculus (in the dominant hemisphere) in a patient with progressive bulbar palsy between Wernicke’s and Broca’s areas, although no remarkable lesions were observed on conventional magnetic resonance images.The injury of the leTh arcuate fasciculus in this patient appeared to coincide with Broca’s aphasia. We recommend evaluation of the arcuate fasciculus using DTT in patients with MNDs who present with aphasia. However, this study has several limitations. First, the diagnosis of progressive bulbar palsy is usually conducted by physical examination and history taking and oThen confused with other types of MND (such as ALS, primary lateral sclerosis, and progressive muscular atrophy), thus accurate diagnosis of progressive bulbar palsy is limited. Second, we could not verify the absenceof other diseases (small size infarction or traumatic axonal injury) which can cause the aphasia or arcuate fasciculus lesions. Third, we obtained DTI data using 1.5 T MRI machine; by contrast, higher tesla MRI machine can show better resolution. Fourth, this is a single case study. Therefore, further studies addressing these limitations are needed.
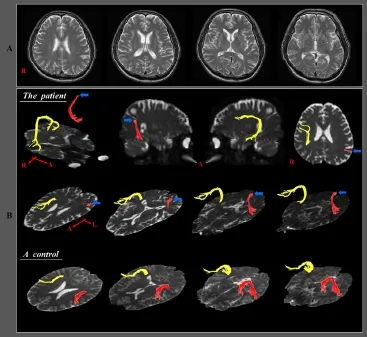
Figure 1 Brain magnetic resonance images and diffusion tensor tractography images of a 74-year-old male patient with progressive bulbar palsy.
This work was supported by the National Research Foundation (NRF) of Korea Grant funded by the Korean Government (MSIP), No. 2015R1A2A2A01004073.
Min Cheol Chang, Han Do Lee, Sung Ho Jang*
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, Daemyungdong, Namgu, Daegu, Republic of Korea
*Correspondence to:Sung Ho Jang, M.D., strokerehab@hanmail.net.
Accepted:2016-10-25
orcid:0000-0001-6383-5505 (Sung Ho Jang)
Adams RD, Victor M, Ropper AH (1997) Degenerative diseases of the nervous system. In: Principles of Neurology, 6th ed. New York: McGraw-Hill, Health Professions Division.
Anderson JM, Gilmore R, Roper S, Crosson B, Bauer RM, Nadeau S, Beversdorf DQ, Cibula J, Rogish M, 3rd, Kortencamp S, Hughes JD, Gonzalez Rothi LJ, Heilman KM (1999) Conduction aphasia and the arcuate fasciculus: A reexamination of the Wernicke-Geschwind model. Brain Lang 70:1-12.
Bak TH, O’Donovan DG, Xuereb JH, Boniface S, Hodges JR (2001) Selective impairment of verb processing associated with pathological changes in Brodmann areas 44 and 45 in the motor neurone disease-dementia-aphasia syndrome. Brain 124:103-120.
Bartha L, Benke T (2003) Acute conduction aphasia: an analysis of 20 cases. Brain Lang 85:93-108.
Ben Bashat D, Artzi M, Tarrasch R, Nefussy B, Drory VE, Aizenstein O (2011) A potential tool for the diagnosis of ALS based on difusion tensor imaging. Amyotroph Lateral Scler 12:398-405.
Bernal B, Ardila A (2009) The role of the arcuate fasciculus in conduction aphasia. Brain 132:2309-2316.
Brooks BR (1994) El Escorial World Federation of Neurology criteria for the diagnosis of amyotrophic lateral sclerosis. Subcommittee on Motor Neuron Diseases/Amyotrophic Lateral Sclerosis of the World Federation of Neurology Research Group on Neuromuscular Diseases and the El Escorial “Clinical limits of amyotrophic lateral sclerosis” workshop contributors. J Neurol Sci 124 Suppl:96-107.
Caselli RJ, Windebank AJ, Petersen RC, Komori T, Parisi JE, Okazaki H, Kokmen E, Iverson R, Dinapoli RP, Graf-Radford NR, Stein SD (1993) Rapidly progressive aphasic dementia and motor neuron disease. Ann Neurol 33:200-207.
Catani M, Mesulam M (2008) The arcuate fasciculus and the disconnection theme in language and aphasia: history and current state. Cortex 44:953-961.
Catani M, Piccirilli M, Geloso MC, Cherubini A, Finali G, Pelliccioli G, Senin U, Mecocci P (2004) Rapidly progressive aphasic dementia with motor neuron disease: a distinctive clinical entity. Dement Geriatr Cogn Disord 17:21-28.
Council MR (1976) Aids to examination of the peripheral nervous system. London: Her Majesty’s Stationery Ofce.
da Rocha AJ, Valerio BC, Buainain RP, Ferraz ME, da Silva CJ, Maia AC, Jr., Andrade VP, Lancellotti CL (2007) Motor neuron disease associated with non-fuent rapidly progressive aphasia: case report and review of the literature. Eur J Neurol 14:971-975.
Han C, Jo SA, Jo I, Kim E, Park MH, Kang Y (2008) An adaptation of the Korean mini-mental state examination (K-MMSE) in elderly Koreans: demographic infuence and population-based norms (the AGE study). Arch Gerontol Geriatr 47:302-310.
Hong YH, Sung JJ, Kim SM, Park KS, Lee KW, Chang KH, Song IC (2008) Difusion tensor tractography-based analysis of the pyramidal tract in patients with amyotrophic lateral sclerosis. J Neuroimaging 18:282-287.
Jang SH, Lee HD (2014) Recovery of injured arcuate fasciculus in the dominant hemisphere in a patient with an intracerebral hemorrhage. Am J Phys Med Rehabil 93:e15-18.
Jang SH, Choi BY, Chang CH, Kim SH, Chang MC (2013a) Prediction of motor outcome based on difusion tensor tractography fndings in thalamic hemorrhage. Int J Neurosci 123:233-239.
Jang SH, Kim SH, Kim OR, Byun WM, Kim MS, Seo JP, Chang MC (2013b) Cingulum injury in patients with difuse axonal injury: a difusion tensor imaging study. Neurosci Lett 543:47-51.
Kim H, Na DL (2004) Normative data on the Korean version of the Western Aphasia Battery. J Clin Exp Neuropsychol 26:1011-1020.
Kim SH, Lee DG, You H, Son SM, Cho YW, Chang MC, Lee J, Jang SH (2011) The clinical application of the arcuate fasciculus for stroke patients with aphasia: a difusion tensor tractography study. NeuroRehabilitation 29:305-310.
Nucifora PG, Verma R, Melhem ER, Gur RE, Gur RC (2005) LeThward asymmetry in relative fber density of the arcuate fasciculus. Neuroreport 16:791-794.
Sage CA, Peeters RR, Gorner A, Robberecht W, Sunaert S (2007) Quantitative diffusion tensor imaging in amyotrophic lateral sclerosis. Neuroimage 34:486-499.
Sarro L, Agosta F, Canu E, Riva N, Prelle A, Copetti M, Riccitelli G, Comi G, Filippi M (2011) Cognitive functions and white matter tract damage in amyotrophic lateral sclerosis: a difusion tensor tractography study. AJNR Am J Neuroradiol 32:1866-1872.
Tsuchiya K, Ozawa E, Fukushima J, Yasui H, Kondo H, Nakano I, Ikeda K (2000) Rapidly progressive aphasia and motor neuron disease: a clinical, radiological, and pathological study of an autopsy case with circumscribed lobar atrophy. Acta Neuropathol 99:81-87.
van der Graaf MM, Sage CA, Caan MWA, Akkerman EM, Lavini C, Majoie CB, Nederveen AJ, Zwinderman AH, Vos F, Brugman F, van den Berg LH, de Rijk MC, van Doorn PA, Van Hecke W, Peeters RR, Robberecht W, Sunaert S, de Visser M (2011) Upper and extra-motoneuron involvement in early motoneuron disease: a difusion tensor imaging study. Brain 134:1211-1228.
Zhang Y, Schuf N, Woolley SC, Chiang GC, Boreta L, Laxamana J, Katz JS, Weiner MW (2011) Progression of white matter degeneration in amyotrophic lateral sclerosis: A diffusion tensor imaging study. Amyotroph Lateral Scler 12:421-429.
10.4103/1673-5374.197149
How to cite this article:Chang MC, Lee HD, Jang SH (2016) Injury of the arcuate fasciculus in a patient with progressive bulbar palsy. Neural Regen Res 11(12):2031-2032.
Open access statement:This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
- 中國神經再生研究(英文版)的其它文章
- Expression changes of nerve cell adhesion molecules L1 and semaphorin 3A aTher peripheral nerve injury
- “Three Methods and Three Points” regulates p38 mitogen-activated protein kinase in the dorsal horn of the spinal cord in a rat model of sciatic nerve injury
- Biodegradable magnesium wire promotes regeneration of compressed sciatic nerves
- Electroacupuncture at Dazhui (GV14) and Mingmen (GV4) protects against spinal cord injury: the role of the Wnt/β-catenin signaling pathway
- Application of a paraplegic gait orthosis in thoracolumbar spinal cord injury
- Fine motor skill training enhances functional plasticity of the corticospinal tract aTher spinal cord injury