
Complex hepatic outflow reconstruction in domino liver transplantation
2014-05-04 02:52:32RafaelPinheiroQuirinoLaiCarolaDahrenmollerandJanLerut
Rafael S Pinheiro, Quirino Lai, Carola Dahrenmoller and Jan Lerut
Brussels, Belgium
Complex hepatic outflow reconstruction in domino liver transplantation
Rafael S Pinheiro, Quirino Lai, Carola Dahrenmoller and Jan Lerut
Brussels, Belgium
Domino liver transplantation has been accepted as a safe procedure to further expand the organ donor pool. The most important technical challenge of the procedure resides in restoring a proper hepatic venous allograft outflow in the familial amyloidotic polyneuropathy-liver recipient. To overcome this issue, combined techniques were used to perform an innovative outflow reconstruction. A domino liver transplantation was successfully performed with reconstruction of complex venous outflow. The inferior vena cava sparing hepatectomy technique in the familial amyloidotic polyneuropathy-donor was used to cut the hepatic vein to the liver parenchyma. To overcome this issue the venous outflow tract was reconstructed using a longitudinally opened iliac vein graft from a post-mortem donor to create a new outflow tract using a diamond patch between the right and middle/left hepatic veins.
liver transplantation;
intraoperative;
anatomy;
hepatic vein
Introduction
Domino liver transplantation (DLT) has been introduced in clinical practice in 1997 by Furtado with the aim to expand the liver donor pool.[1]Larger experiences have shown that this procedure, using mostly livers from familial amyloidotic polyneuropathy (FAP) patients, can be safely used not only in older or cancer recipients but also in younger patients presenting with benign diseases.[2]
The most important technical challenges of the procedure reside in the realization of a FAP-liver harvest without harming the FAP-donor and in restoring a proper hepatic venous allograft outflow in the FAP-liver recipient. To overcome this issue, we have combined techniques to perform an innovative outflow reconstruction.
Surgical technique
A successful DLT with complex venous outflow reconstruction was done. The inferier vena cava (IVC) sparing hepatectomy technique in the FAP-donor was used to cut the hepatic veins (HVs) flush to the liver parenchyma. The distance between the right hepatic vein (RHV) and the left hepatic vein (LHV) and median hepatic vein (MHV) was very large. Moreover, the (outside) procurement team of the post-mortem liver allograft implanted in the FAP-donor omitted the procurement of supplementary vascular grafts. To overcome both problems, the venous outflow tract was reconstructed using a longitudinally opened iliac vein graft from another post-mortem donor. A three by one cm, diamond shaped, the patch was sutured to the median borders of the RHV and MHV (Fig. 1). Afterwards, the venous patch graft (2 cm wide) was sutured circumferentially to all three HV orifices including the inlay patch. Finally, the two lateral parts of the iliac vein graft were sutured vertically to each other in order to obtain a nice cylindrical cone having theshape of the suprahepatic IVC cuff (Fig. 2). The newly created outflow tract was anastomosed to the cuff of the MHV and LHV of the recipient. There was no congestion at revascularization, and repetitive Doppler ultrasound examinations showed a normal tri-phasic outflow signal (Fig. 3). The patient was discharged after 20 days, her outcome was excellent and she was doing well 14 months after transplantation. The 12 months protocol biopsy did not show any sign of outflow obstruction.
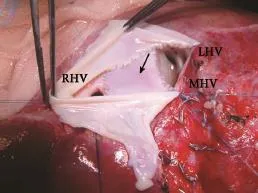
Fig. 1.Outflow reconstruction using a diamond shaped patch (arrow) sutured to the median borders of the RHV and MHV. An iliac venous patch graft (hold by the pick ups) been sutured circumferentially to all three HVs including the interposition patch. RHV: right hepatic vein; MHV: median hepatic vein; LHV: left hepatic vein.
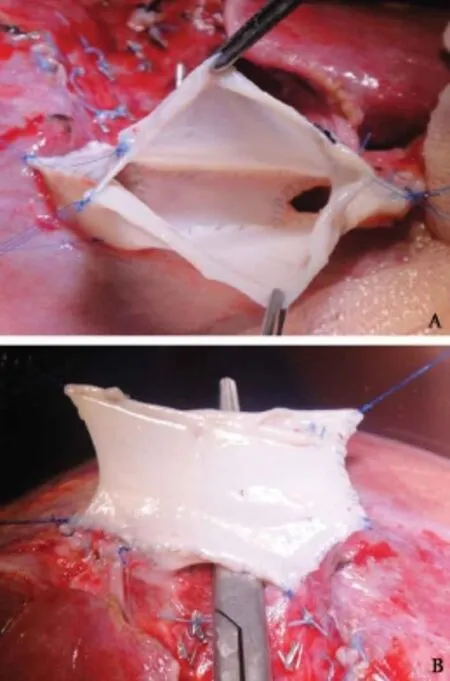
Fig. 2.Complex hepatic venous reconstruction to domino liver transplant recipient.A: Final aspect of the newly created outflow tract shaped as a caval vein;B: Scissors demonstrating the free space between RHV, MHV and LHV.
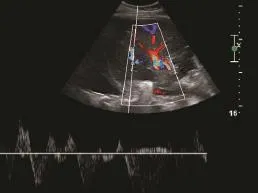
Fig. 3.Doppler ultrasound examination showing a normal tri-phasic outflow signal.
Discussion
With growing experience in the field of living donor liver transplantation (LDLT) and DLT, technical modifications were introduced aiming at enhancing the safety of the FAP-donor and the FAP-liver recipient.[3, 4]Harvesting the FAP-liver without the IVC has nowadays become the procedure of choice as it allows almost always the intervention without the use of veno-venous bypass (VVB). Whilst favoring the FAP-donor, this technique puts the FAP-liver recipient at disadvantage by possibly compromising the venous outflow of allograft. Safe FAP-liver implantation therefore needs a back-table reconstruction of the tract of venous outflow.[5-8]This is usually done by anastomosing all three HV orifices to a free cavo-iliac, cavo-renal or pulmonary bifurcation venous graft. In case of the unavailability of such grafts or in case of HV anomalies, a more complex back-table procedure may be necessary.
This technique for hepatic venous reconstruction may be a life-saver in DLT, especially when vascular allografts originating from the post-mortem donor or the recipient are unavailable.
Contributors:LJ proposed the study. PRS and LQ performed research and wrote the first draft. DC collected and analyzed the data. All authors contributed to the design and interpretation of the study and to further drafts. LJ is the guarantor.
Funding:None.
Ethical approval:Not needed.
Competing interest:No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
1 Garcia JH, de Vasconcelos JB, Costa PE, Coelho GR, Brasil IR, Barros MA, et al. Domino liver transplantation with double piggyback: is this the best technique? A case report. Transplant Proc 2006;38:2968-2970.
2 Wilczek HE, Larsson M, Ericzon BG; FAPWTR. Long-term data from the Familial Amyloidotic Polyneuropathy World Transplant Registry (FAPWTR). Amyloid 2011;18:193-195.
3 Lee SG. Techniques of reconstruction of hepatic veins in living-donor liver transplantation, especially for right hepatic vein and major short hepatic veins of right-lobe graft. J Hepatobiliary Pancreat Surg 2006;13:131-138.
4 Bispo M, Marcelino P, Marques HP, Martins A, Perdigoto R, Aguiar MJ, et al. Domino versus deceased donor liver transplantation: association with early graft function and perioperative bleeding. Liver Transpl 2011;17:270-278.
5 Pacheco-Moreira LF, de Oliveira ME, Balbi E, da Silva AC, Miecznikowski R, de Faria LJ, et al. A new technical option for domino liver transplantation. Liver Transpl 2003;9:632- 633.
6 Padín JM, Pfaffen G, Pérez Fernández I, Sandi M, Ramisch D, Barros Schelotto P, et al. Neo-suprahepatic cava: a case report of a modified technique for domino liver transplantation. Transplant Proc 2011;43:2090-2092.
7 Liu C, Loong CC, Hsia CY, Tsou MY, Tsai HL, Wei CF. Venoplasty of hepatic venous outflow with a venous patch in domino liver transplantation. Liver Transpl 2008;14:1378- 1379.
8 Soin A, Kumaran V, Mohanka R, Mehta N, Mohan N, Nundy S. Bridge venoplasty: a new technique to simplify venous outflow reconstruction in living donor domino liver transplantation. Surgery 2010;148:155-157.
Received November 7, 2012
Accepted after revision July 10, 2013
(Hepatobiliary Pancreat Dis Int 2014;13:98-100)
AuthorAffiliations:Starzl Unit of Abdominal Transplantation, University Hospitals Saint Luc, Université Catholique Louvain UCL Brussels, Belgium (Pinheiro RS); Department of Gastroenterology, S?o Paulo University School of Medicine, S?o Paulo, Brazil (Pinheiro RS, Lai Q, Dahrenmoller C and Lerut J)
Rafael S Pinheiro, MD, Department of Gastroenterology, University of S?o Paulo, Hospital das Clínicas, Rua Dr. Enéas de Carvalho Aguiar, 255, 9° andar - sala 9113/9114, CEP 05403-900 - S?o Paulo - SP, Brazil (Tel: 55-11-26613323; Fax: 55-11-26616250; Email: rsnpinheiro@ gmail.com)
? 2014, Hepatobiliary Pancreat Dis Int. All rights reserved.
10.1016/S1499-3872(14)60014-X
 Hepatobiliary & Pancreatic Diseases International2014年1期
Hepatobiliary & Pancreatic Diseases International2014年1期
- Hepatobiliary & Pancreatic Diseases International的其它文章
- Samaritan donor interchange in living donor liver transplantation
- lntrahepatic Glissonian approach and outflow vascular occlusion during partial hepatectomy
- Novel en-bloc resection of locally advanced hilar cholangiocarcinoma: the Rex recess approach
- KAI1 inhibits lymphangiogenesis and lymphatic metastasis of pancreatic cancer in vivo
- Effect of CD74 on the prognosis of patients with resectable pancreatic cancer
- Blood group type antigens in pancreatic intraductal papillary mucinous neoplasms