
Laryngo-tracheobronchial Amyloidosis: a Case Report and Review of Literature
2014-04-20 01:36:50JingxiaWangShanYangHaihongChenQinyingWangYuyuLuandLiliJiang
Chinese Medical Sciences Journal 2014年1期
Jing-xia Wang, Shan Yang, Hai-hong Chen, Qin-ying Wang, Yu-yu Lu, and Li-li Jiang
Department of Head-neck Otolaryngology, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310003, China
AMYLOIDOSIS is a benign process which can have systemic involvement. Though larynx is the common site of localized amyloidosis in the head and neck region,1it was seldom reported with heterochronous implication of bilateral ventricles. Here we report a case of laryngeal amyloidosis heterochronously localized at bilateral ventricles with tracheobronchial involvement. Combined with our experience we reviewed the literature, and discuss the pertinent managements of this condition.
CASE DESCRIPTION
A 31-year-old man was admitted to the First Affiliated Hospital of Zhejiang University with complaints of a hoarse voice of 3-year’s duration with chronic cough, and intermittent hemoptysis and mild dyspnea currently. He was a non-smoker. Laryngoscopy revealed a large non-ulcerated, red subepithelial mass arising from the right ventricle (Fig. 1). The epiglottis and the epiglottic vallecula appeared normal, both vestibule folds were swelling, the right vocal cord was not visible while the left vocal cord appeared normal. Laboratory test results on admission showed no abnormality in complete blood count, serum electrolytes, creatinine, liver function, albumin, total serum protein, and erythrocyte sedimentation rate. His family history was unremarkable. He had an open surgery for laryngeal amyloidosis in left ventricle, and a flexible bronchoscopic examination 4 years ago. His uncomfortable feeling at that time was similar as at this time: gradually progressive hoarseness and mild dyspnea after exercise. Bronchoscopy revealed diffuse thickening, mucosal friability, and narrowing of the right main bronchus. Biopsy specimen revealed eosinophilic deposits in the submucosa with apple-green birefringence on Congo red stain, a finding characteristic of amyloid. A computed tomography (CT) scan at chest was arranged upon this admission, the result demonstrated circumferential wall thickening with calcifications as well as luminal narrowing at the right main bronchus (Fig. 2). Being with no dyspnea, he was suggested to stay in hospital for observation of his bronchial lesion.
The patient was scheduled for a local mass excision by laser through staged laryngoscopy under general anes- thesia. Histopathological examination revealed amorphous deposits of eosinophilic, acellular, and homogenous material within the subepithelial stroma, a finding characteristic of laryngeal amyloidosis.
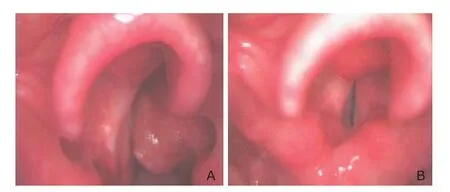
Figure 1. Pre-operative laryngoscopic image shows a mass of amyloid on the right ventricle (A), and the laryngoscopic examination 18 months after operation shows no evidence of recurrence (B).
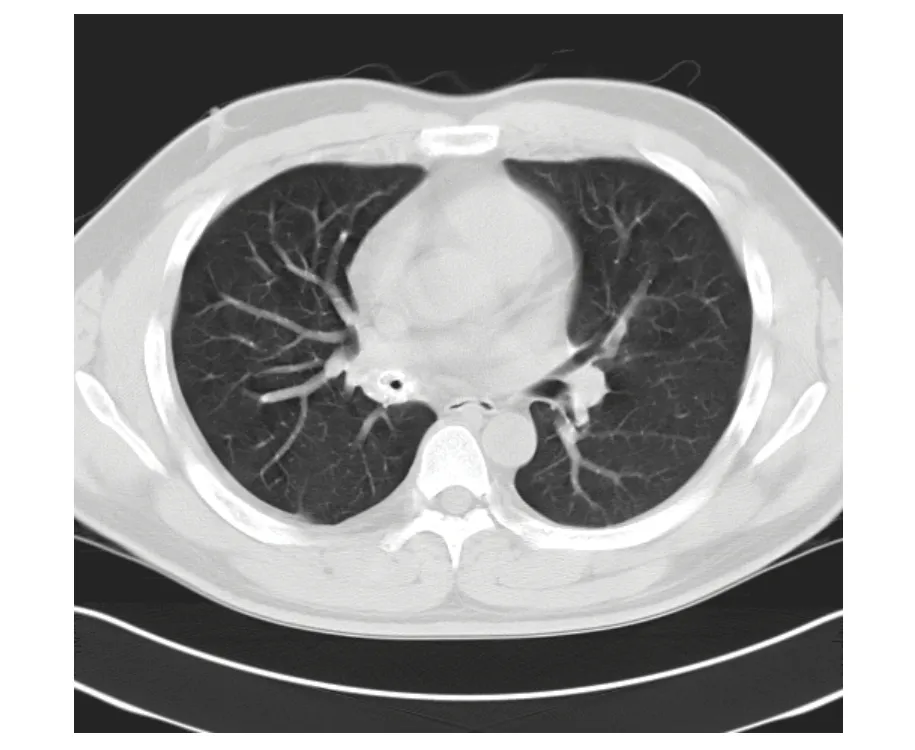
Figure 2. Chest computed tomography scan reveals circumferential thickening with partial calcification of the right main bronchus.
The post-operative recovery was uneventful, and the patient was discharged the day after operation. During the 6-year’s follow-up, his voice improved greatly. No recurrence was noted although there was some swelling of the right ventricular band (Fig. 1). Chest CT re-examination indicated that the bronchial lesion was almost stable. Sometimes the patient suffered from recurrent cough, especially when having caught a cold. Medication including corticosteroids and antibiotics were prescribed to alleviate his symptoms when suffering from respiratory infection.
DISCUSSION
Amyloidosis is a condition characterized by extracellular accumulation of proteinaceous material in the tissue. Its precise etiology still remains unclear. It may affect multiple organs, of which the commonest site is the larynx, bronchus, and kidneys.2,3
A definite diagnosis of amyloidosis depends on obtaining a tissue biopsy and demonstration of amyloid by appropriate stains. CT or magnetic resonance imaging (MRI) may be helpful in mapping lesions, which may be more extensive than they appear in laryngoscopy. In CT examination, amyloidosis is demonstrated as a marked thickening of the laryngeal soft tissue with high density. The signals characteristic of amyloid on MRI resemble those of skeletal muscles. This may be an important differentiating point because muscle is an easy frame of reference, and tumors do not appear in this manner on MRI images. Tracheobronchial amyloidosis on CT images appears as circumferential wall thickening with calcifications as well as luminal narrowing at various levels of the tracheobronchial tree, as was observed in the patient of this case.
Treatment for extensive benign laryngeal disease can be challenging. As it is a benign disease process, consideration must be given to function preservation and ultimate influence on voice. The main treatment of choice is surgical excision with function preservation. In the case of diffuse submucosal deposits, repeated excisions are often necessary to restore the airway and conserve the voice, especially for amyloidosis of the true vocal cords. It is interesting that the voice can be normal or nearly normal with the amyloid visible on the undersurface of even both vocal cords if the upper margin is 2 to 3 mm below the free edge;4on the other hand, visible residual amyloid on the undersurface of the true vocal cords may regrow very slowly, so in order to conserve voice after operation, it is sometimes unnecessary to conduct a complete removal of true vocal cord amyloid, a second resection at the same or opposite side may be based on voice quality. Now advances in laser technology have made staged endoscopic excision an effective option in extensive lesion. In the present case, the lesion was excised with laser through staged laryngoscopy under general anesthesia. After 6-year’s follow-up, the patient recovered well from the operation and was satisfied with the result of this approach for a well preserved voice.
For pulmonary amyloidosis, there have been no established effective treatments up to now. Management largely depends on the severity of symptoms. To patients who have no or mild symptoms, simply observation is the best choice, just as in this case. To patients who have remarkable symptoms, options of treatment include bronchoscopic resection with laser technique,5,6bronchoscopic dilatation and stenting,7,8and external beam radiation.9,10In the patient of this case, CT scan showed a 2-cm-long circumferential narrowing at the right main bronchus, it will be suitable to give him a stenting when necessary.
In conclusion, although amyloidosis is a benign lesion, there are currently no curative treatments for it, especially for systemic amyloidosis. The main goal in the manage- ment of such patients is symptoms alleviation or resolution, conservative surgical excision with function preservation remains the treatment of choice.
1. Kennedy TL, Patel NM. Surgical management of localized amyloidosis. Laryngoscope 2000; 110: 918-23.
2. Passerotti GH, Caniello M, Hachiya A, et al. Multiple-sited amyloidosis in the upper aerodigestive tract: case report and literature review. Braz J Otorhinolaryngol 2008; 74:462-6.
3. Said SM, Sethi S, Valeri AM, et al. Renal amyloidosis: origin and clinicopathologic correlations of 474 recent cases. Clin J Am Soc Nephrol 2013; 8:1515-23.
4. Dedo HH, Izdebski K. Laryngeal amyloidosis in 10 patients. Laryngoscope 2004; 114: 1742-6.
5. Madden BP, Lee M, Paruchuru P. Successful treatment of endobronchial amyloidosis using Nd: YAG laser therapy as an alternative to lobectomy. Monaldi Arch Chest Dis 2001; 56: 27-9.
6. Ding L, Li W, Wang K, et al. Primary tracheobronchial amyloidosis in China: analysis of 64 cases and a review of literature. J Huazhong Univ Sci Technolog Med Sci 2010; 30: 599-603.
7. Yang S, Chia SY, Chuah KL, et al. Tracheobronchial amyloidosis treated with rigid bronchoscopy and stenting. Surg Endosc 2003; 17: 658-9.
8. Hanon S, De Keukeleire T, Dieriks B, et al. Primary tracheo- bronchial amyloidosis: a series of 3 cases. Acta Clin Belg 2007; 62: 56-60.
9. Ren S, Ren G. External beam radiation therapy is safe and effective in treating primary pulmonary amyloidosis. Respir Med 2012; 106: 1063-9.
10. Truong MT, Kachnic LA, Grillone GA, et al. Long-term results of conformal radiotherapy for progressive airway amyloidosis. Int J Radiat Oncol Biol Phys 2012; 83: 734-9.
 Chinese Medical Sciences Journal2014年1期
Chinese Medical Sciences Journal2014年1期
- Chinese Medical Sciences Journal的其它文章
- Sorafenib in Liver Function Impaired Advanced Hepatocellular Carcinoma
- Isolated Pancreatic Tuberculosis in Non-immunocompromised Patient Treated by Whipple’s Procedure: a Case Report
- Reversible Posterior Leukoencephalopathy Syndrome in Children with Nephrotic Syndrome: a Case Report
- Comparison of the Outcomes of Monopolar and Bipolar Radiofrequency Ablation in Surgical Treatment of Atrial Fibrillation
- Bloodstream Infection with Carbapenem-resistant Klebsiella Pneumoniae and Multidrug-resistant Acinetobacter Baumannii: a Case Report
- Factors Associated with Coronary Artery Disease in Young Population (Age≤40): Analysis with 217 Cases