
Spindle cell carcinoma of the breast as complex cystic lesion: a case report
2014-03-29 05:27:23MasahiroKitadaSatoshiHayashiYoshinariMatsudaKeiIshibashiKeisukeOikawaNaoyukiMiyokawa
Cancer Biology & Medicine 2014年2期
Masahiro Kitada, Satoshi Hayashi, Yoshinari Matsuda, Kei Ishibashi, Keisuke Oikawa, Naoyuki Miyokawa
1Department of Surgery,
2Department of Clinical Pathology, Asahikawa Medical University, Asahikawa Hokkaido 078-8510, Japan
Spindle cell carcinoma of the breast as complex cystic lesion: a case report
Masahiro Kitada1, Satoshi Hayashi1, Yoshinari Matsuda1, Kei Ishibashi2, Keisuke Oikawa2, Naoyuki Miyokawa2
1Department of Surgery,
2Department of Clinical Pathology, Asahikawa Medical University, Asahikawa Hokkaido 078-8510, Japan
Spindle cell carcinoma of the breast is a rare tumor.is tumor can proliferate rapidly and cause cystic changes because of internal tissue necrosis. We evaluated a 54-year-old woman with right breast lump. Mammography showed a category four mass with a diameter of 2.5 cm. Ultrasonography (US) revealed a complex cystic lesion, and fi ne-needle aspiration (FNA) cytology demonstrated bloody fluid and malignant cells. Partial breast resection and sentinel lymph node biopsy were performed. Immunohistology revealed spindle cells with positive results for cytokeratin (AE1/AE3) and vimentin, partially positive results for s-100, and negative results for desmin and α-actin. The pathological stage was IIA, and biochemical characterization showed that the tumor was triple negative. Six courses of FEC-100 chemotherapy (5-fluorouracil 500 mg/m2, epirubicin 100 mg/m2, and cyclophosphamide 500 mg/m2) were administered. Radiotherapy was performed.is case is discussed with reference to the literature.
Breast cancer; spindle cell carcinoma; cystic lesion
Introduction
Spindle cell carcinoma of the breast is composed of a mixture of sarcomatoid spindle and epithelial adenocarcinoma cells, representing carcinosarcoma. This entity is now classified as a subtype of malignant epithelial tumor. In this relatively rare histological type, rapid proliferation may cause cystic changes because of internal tissue necrosis. In this paper, we report a rare case of spindle cell carcinoma in breast, and this study was approved by the institutional ethics commiee.
Case report
A 54-year-old woman presented to her personal physician and complained the pain on her right breast. She underwent a breast surgery in our hospital. The patient and her family’s medical histories were unremarkable.
The patient was 157 cm tall and weighed 53 kg. Physical examination of the right breast (area C) revealed an elastic hard mass measuring 2.5 cm × 2.5 cm. Margins were distinct, with relatively good mobility and a tumor-nipple distance of 3.2 cm. No axillary or cervical lymph nodes were palpable. Hematological and biochemical blood test results were normal.e levels of tumor markers, such as carcinoembryonic antigen, carbohydrate antigen 15-3, and National Cancer Center-Stomach-439, were within normal limits.
Mammography revealed an indistinct margined hyper dense mass in the right outer portion, which was assessed as Breast Imaging-Reporting and Data System category 4C (Figure 1A: MLO view, Figure 1B: CC view). Breast ultrasonography (US) revealed complex cystic lesion, and the tumor was large with 2.5 cm diameter (Figure 2). Complex cystic lesion on US with blood content on fine-needle aspiration (FNA) cytology revealed malignant cells. Preoperative magnetic resonance imaging (MRI) fi ndings and a T2 weight image revealed an early enhancement image with no intraductal spread (Figure 3). No distant metastases was identified on computed tomography or bone scan. The tumor stage was T2N0M0. Breast-conserving surgery and sentinel lymph node biopsy were performed.
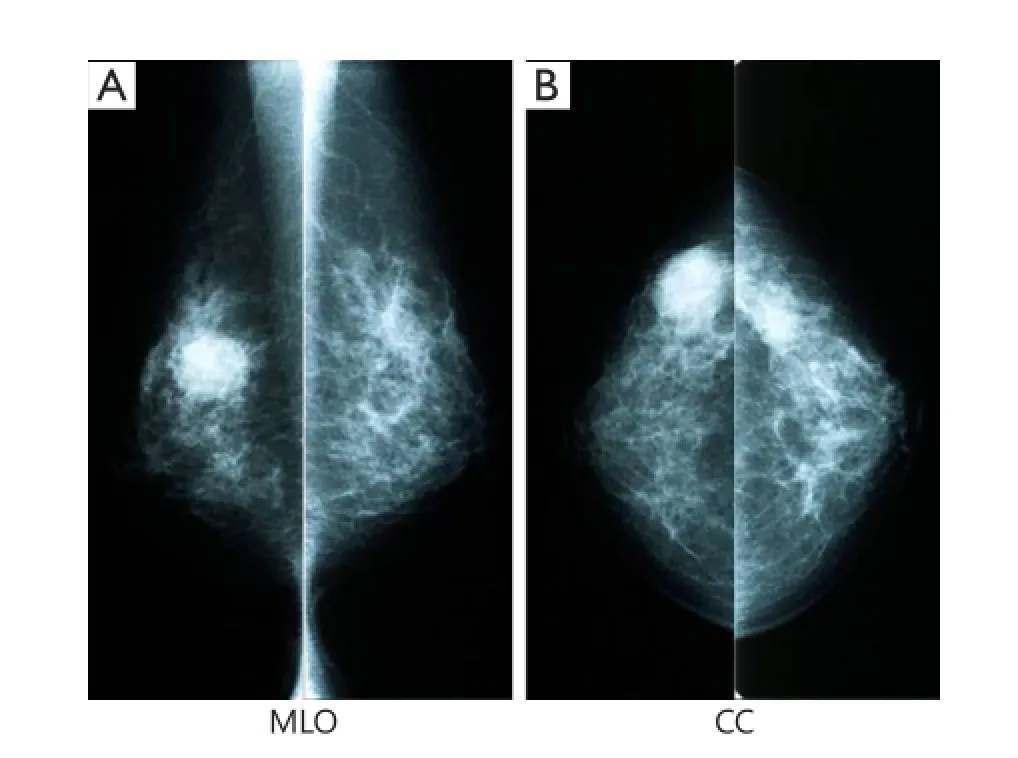
Figure 1 Mammography revealed a round, highly dense 2.5 cm mass with fi ne serrations on the right-middle outside area (A, MLO; B, CC).

Figure 2 Breast US revealed complex cystic lesion, and the tumor was large with 2.5 cm diameter.
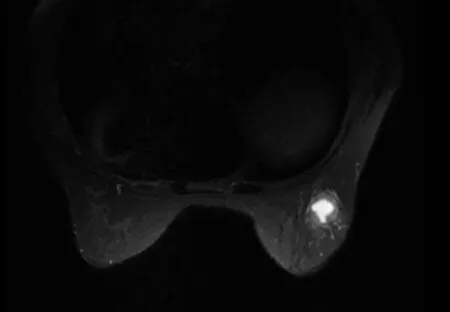
Figure 3 Preopetative breast MRI (T2 weighted image). MRI fi ndings and a T2 weight image revealed an early enhancement image with no intraductal spread. MRI, magnetic resonance imaging.
The results exposed two sentinel lymph nodes and no malignant cell. The tumor measured 2.0 cm in diameter and contained a central cystic area (Figures 4,5). Histopathological examination showed low papillary growth in the cystic cavity surface, which was covered by adenocarcinomatous components associated with some squamous metaplasia. Most of the lesions comprising the cyst wall were a mixture of irregular bundles of spindle-shaped tumor cells and fibrous connective tissue proliferation.e tumor was diagnosed as spindle cell (Figure 6).
Immunostaining of spindle-shaped tumor cells showed positive results for cytokeratin (AE1/AE3) and vimentin (Figures 7,8), partially positive results for s-100, and negative results for desmin and α-actin. The final histopathological diagnosis was spindle cell carcinoma. Histological grade from malignancy was grade III. Lymphatic invasion was negative, whereas blood vessel invasion was positive. Lymph node metastasis was negative, and p-stage I was diagnosed. Estrogen receptor, progesterone receptor, and human epidermal growth factor receptor type 2 (HER2), which showed negative resultsby biochemical tests, were called triple negative type in subtype classification. The postoperative course was uneventful. The patient received six courses of FEC-100 chemotherapy. Radiotherapy included simultaneous integrated boost enforced 60 Gy (2 Gy/day) to the residual breast tissue. Aer 24 months of postoperation, no recurrence has been detected.
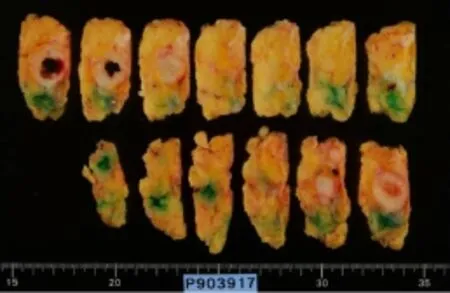
Figure 4 Resected specimen of cut surface; the tumor measured 2.0 cm in diameter and contained a central cystic area.
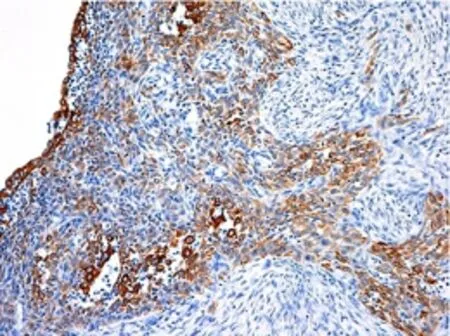
Figure 7 Immunohistological findings of the positive staining for cytokeratin (AE1/AE3) (H&E staining ×100).
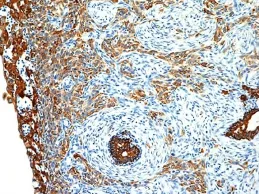
Figure 8 Immunohistological findings of the positive staining for vimentin (H&E staining ×100).
Discussion
Spindle cell carcinoma of the breast is a rare histological carcinoma, accounting for approximately 0.08% of all breast cancers1. Together with squamous cell carcinoma and carcinoma with osseous and chondroid metaplasia, this entity is classified as a metaplastic carcinoma2. The tumor comprises spindleshaped cells with a sarcomatoid appearance, representing carcinosarcoma. In the present case, some tumor cell nests with epithelial features and areas of squamous metaplasia were observed.e sarcomatoid component is de fi ned as a component by which epithelial cancer cells assume a spindle shape. In our hospital, which has been operating for over 10 years, only 3 (0.024%) of 1,280 breast cancer surgery cases have involved spindle cell carcinoma.
At the time of initial diagnosis, numerous spindle cell carcinomas tend to be large and localized, with histopathological examination often showing well-defined margins or a partially nodular appearance3.e image view of spindle cell carcinoma reveals a large size and nonspeci fi c shadow, clear of the boundary around on mammography, and high signal intensity on T2 MRI images4. On breast US, the cystic change is not rare, these cysts are not true cysts with a capsule, but rather result from internal degeneration and necrosis because of relatively rapid tumor proliferation.
Breast-conserving surgery is often difficult because of the large tumor size in numerous patients5. A report has indicated that the tumor average diameter is 4 cm6. Lymph node metastasis is less common than other breast cancers6,7. In the present case, breast-conserving surgery is possible when minimal peripheral invasion or intraductal spread is present.
Histopathological examination revealed spindle-shaped sarcomatoid cell proliferation and a distinct area of epithelial cancer cells. In the sarcomatoid component, epithelial characteristics were decreased; therefore, immunostaining revealed a mixture of areas positive for epithelial marker cytokeratin and mesenchymal marker vimentin. Many of the tumors discussed above are histological grade from malignancy grade III, but the prognosis may be poor even in grade I8. This finding is largely attributable to biochemical characteristics on the tumor, such as the high negative rates of hormone receptors and HER2/neu protein6,9. Given this triplenegative status exhibited in many cases, hormone and moleculartargeted therapies are oen ine ff ective. Treatment therefore usually consists of chemotherapy. However, no specific chemotherapyregimens has been devised for metaplastic carcinoma, including spindle cell carcinoma. As spindle cell carcinoma shows sarcomatoid features, the efficacy of chemotherapy is also often uncertain5. Treatment is thus based on protocols for invasive ductal cancer. In our patient, the histopathological diagnosis was T2N0, grade III, triple-negative; therefore, six courses of FEC-100 were administered. No sign of recurrence has been identi fi ed as of the time of writing, that is, 10-month postoperation. Nevertheless, careful follow-up observation will be required.
Conclusion
We reported rare spindle cell carcinoma in breast presenting as complex cystic lesion with blood content at FNA. Enforced breast-conserving surgery and sentinel lymph node biopsy were performed.
Con fl ict of interest statement
No potential con fl icts of interest are disclosed.
1. Okushiba S, Minagawa H, Shimizu M, Ambo Y, Kaji M, Omi M, et al. A case of spindle cell carcinoma of the breast--long survival achieved by multiple surgical treatment. Breast Cancer 2001;8:238-242.
2. Tavassoli FA, Devilee P. eds. World Health Organization Classi fi cation of tumors. Pathology and Genetics of Tumors of the Breast and Female Genital Organs. Lyon: IARC Press, 2003;38-39.
3. Sneige N, Yaziji H, Mandavilli SR, Perez ER, Ordonez NG, Gown AM, et al. Loe-grade ( fi bromatous-like) spindle cell carcinomaof the breast. Am J Surg Pathol 2001;25:1009-1016.
4. Choi BB, Shu KS. Metaplastic carcinoma of the breast: multimodality imaging and histopathologic assessment. Acta Radiol 2012;53:5-11.
5. Pezzi CM, Patel-Parekh L, Cole K, Franko J, Klimberg VS, Bland K. Characteristics and treatment of metaplastic breast cancer: analysis of 892 cases from the National Cancer Data Base. Ann Surg Oncol 2007;14:166-173.
6. Carter MR, Hornick JL, Lester S, Fletcher CD. Spindle cell (sarcomatoid) carcinoma of the breast: a clinicopathologic and immunohistochemical analysis of 29 cases. Am J Surg Pathol 2006;30:300-309.
7. Higa J, Yamamoto H, Kaneshiro T, Nakachi A, Teruya T. A case of spindle cell carcinoma of the breast with a review of 35 cases reported in Japan between 2004 and 2006. Jpn J Breast Cancer 2007;22:340-343.
8. Khan HN, Wyld L, Dunne B, Lee AH, Pinder SE, Evans AJ, et al. Spindle cell carcomatoid of the breast: a case series of e rare histological subtype. Eur J Surg Oncol 2003;29:600-603.
Cite this article as:Kitada M, Hayashi S, Matsuda Y, Ishibashi K, Oikawa K, Miyokawa N. Spindle cell carcinoma of the breast as complex cystic lesion: a case report. Cancer Biol Med 2014;11:130-133. doi: 10.7497/ j.issn.2095-3941.2014.02.008
Masahiro Kitada
E-mail: k1111@asahikawa-med.ac.jp
Received January 30, 2014; accepted March 26, 2014. Available at www.cancerbiomed.org
Copyright ? 2014 by Cancer Biology & Medicine
 Cancer Biology & Medicine2014年2期
Cancer Biology & Medicine2014年2期
- Cancer Biology & Medicine的其它文章
- Polymeric nanocomposites loaded with fluoridated hydroxyapatite Ln3+ (Ln = Eu or Tb)/iron oxide for magnetic targeted cellular imaging
- An unusual case of aggressive systemic mastocytosis mimicking hepatic cirrhosis
- Effects of postmastectomy radiotherapy on prognosis in different tumor stages of breast cancer patients with positive axillary lymph nodes
- Clinico-pathological signi fi cance of extra-nodal spread in special types of breast cancer
- Incidence and mortality of female breast cancer in the Asia-Paci fi c region
- Research progress on the anticarcinogenic actions and mechanisms of ellagic acid