
Correlation between insight and internalized stigma in patients with schizophrenia
2012-07-08 02:15:19YingLUXiaopingWANG
上海精神醫(yī)學(xué) 2012年2期
Ying LU, Xiaoping WANG
Correlation between insight and internalized stigma in patients with schizophrenia
Ying LU1,2, Xiaoping WANG1*
Background:The relationship between insight and internalized stigma in patients with schizophrenia is important both for theoretical and practical reasons because of its close association with patients’ willingness to seek (or accept) care for their mental illness.
Objective:To investigate the relationship between insight and internalized stigma in patients with schizophrenia in mainland China.
Methods:65 inpatients and 27 outpatients with schizophrenia who had a median duration of four years of illness completed Chinese versions of two self-report questionnaires—the Internalized Stigma of Mental Illness (ISMI) scale and the Modified Consumer Experiences of Stigma Questionnaire (MCESQ). The patients were also assessed by senior psychiatrists using the Scale for Assessment of Positive Symptoms (SAPS) and the Scale for Assessment of Negative Symptoms (SANS). Patients were divided into those with and without insight into their illness based on the score of the insight item on the Chinese version of the Brief Psychiatric Rating Scale.
Results:49 patients were classified as having insight and 43 classified as lacking insight. Compared to patients with insight, those without insight had a significantly shorter duration of illness, were more likely to be inpatients, and (at trend level only) had more prominent positive and negative symptoms. The ‘a(chǎn)lienation’ subscale score of the ISMI was significantly higher in patients with insight but none of the remaining six subscales in the two instruments were different between the two groups and only 4 of the 48 separate items in the two scales were significantly different between the groups. Logistic regression analysis found no relationship between lack of insight and the scores of the two self-completion stigma scales or the scores of the two clinician-administered symptom scales.
Conclusion:This study among inpatients and outpatients with schizophrenia in China does not support findings of previous studies that report increased experience of stigma among patients who have better insight. The measures of stigma used in the study need further revision and validation for use in China and studies with a wider spectrum of patients that make more detailed assessments of insight and that follow fluctuations in insight and experiences of stigma over time are needed to clarify the complex relationship between these two phenomena in patients with schizophrenia.
1. Introduction
The concept of stigma, initially proposed by Goffman in 1963, refers to an attribute that is deeply discrediting.[1]Stigma initially meant a brand, the mark that identifies persons with immoral character. Since the 1990s, stigma related to mental disorders has been extensively studied in Western countries. The stigmatization of mental illness is common among the general population, psychiatric patients, and their families. These negative attitudes are primarily based on the belief that psychiatric patients are prone to impulsive acts of violence and are incompetent because of their decreased capabilities.[2,3]Such negative attitudes label psychiatric patients and isolate them from society. Because of the existence of stigma, patients often decrease their expectations about their potential achievements and regard themselves as losers.[4]Stigma delays care-seeking for psychological problems and increases the difficulties patients with mental illnesses face when trying to re-integrate into society after an acute episode of illness.
Most studies on stigma among psychiatric patients have been conducted in Western countries. The results have often been used by governments and civil societyorganizations in carrying out activities or interventions to reduce stigma. In China, more than half of the subjects included in the limited number of studies about stigma in the mentally ill report various forms of discrimination.[5,6]Some authors have described possible reasons for mental disorder-related stigma and possible countermeasures.[7,8]However, few Chinese researchers have separately studied stigma among schizophrenic patients using standardized stigma evaluation tools.
Insight in mental illness refers to a patient's understanding and judgment of his disorder. It is an important marker of recovery from some mental disorders, including schizophrenia. Some authors believe patients with insight tend to have higher self-stigma,[9]while other authors do not support this conclusion.[10]In this study we administer standardized stigma evaluation tools to patients with schizophrenia to explore the association between insight and internalized stigma.
2. Methods
2.1 Subjects
The enrollment of subjects in the study is shown in Figure 1. Outpatients and inpatients 17-60 years of age with a DSM-IV diagnosis of schizophrenia who were in an active course of treatment (i.e., not in the residual phase of illness) at the Department of Psychiatry at the Second Xiangya Hospital from January 2010 to March 2010 were potential subjects for the study. Patients with co-morbid mental or physical disorders or who were unable to understand the self-completion questionnaires employed in the study were excluded. Of 103 identified subjects, 8 refused to participate, 2 had co-morbid serious physical illnesses, and 1 only completed part of the self-completion instruments; most patients who refused did so because of concerns regarding confidentiality of the information obtained. Thus 92 subjects (30 outpatients and 62 inpatients) were included in the analysis. There were no significant differences in the age, gender, duration or illness or status (inpatient v. outpatient) between those who did and did not complete the questionnaires.
All subjects and their guardians provided written consent to participate in the study. The study was approved by the ethics review committee of the Second Xiangya Hospital of Central South University.
2.2 Instruments
2.2.1 Demographic data
A questionnaire designed by the authors was used to collect basic demographic data and information about the course of illness: age of the first onset, frequency of hospitalizations, family history, and current status of the disease.
2.2.2 Evaluation of insight
Insight was evaluated using item 19 of the Chinese version of the Brief Psychiatric Rating Scale (BPRS)[11]which reads 'Disorder of insight involving failure to recognize one's own mental illness, psychological symptoms or abnormal words and deeds'. Patients who scored '0' (not present) or '1' (very mild) on the item were classified ashaving insight into their illness while those scoring '2' ('mild') or higher on the item were classified as lacking insight. The reported inter-rater reliability of item 19 is excellent (ICC=0.913).[11]
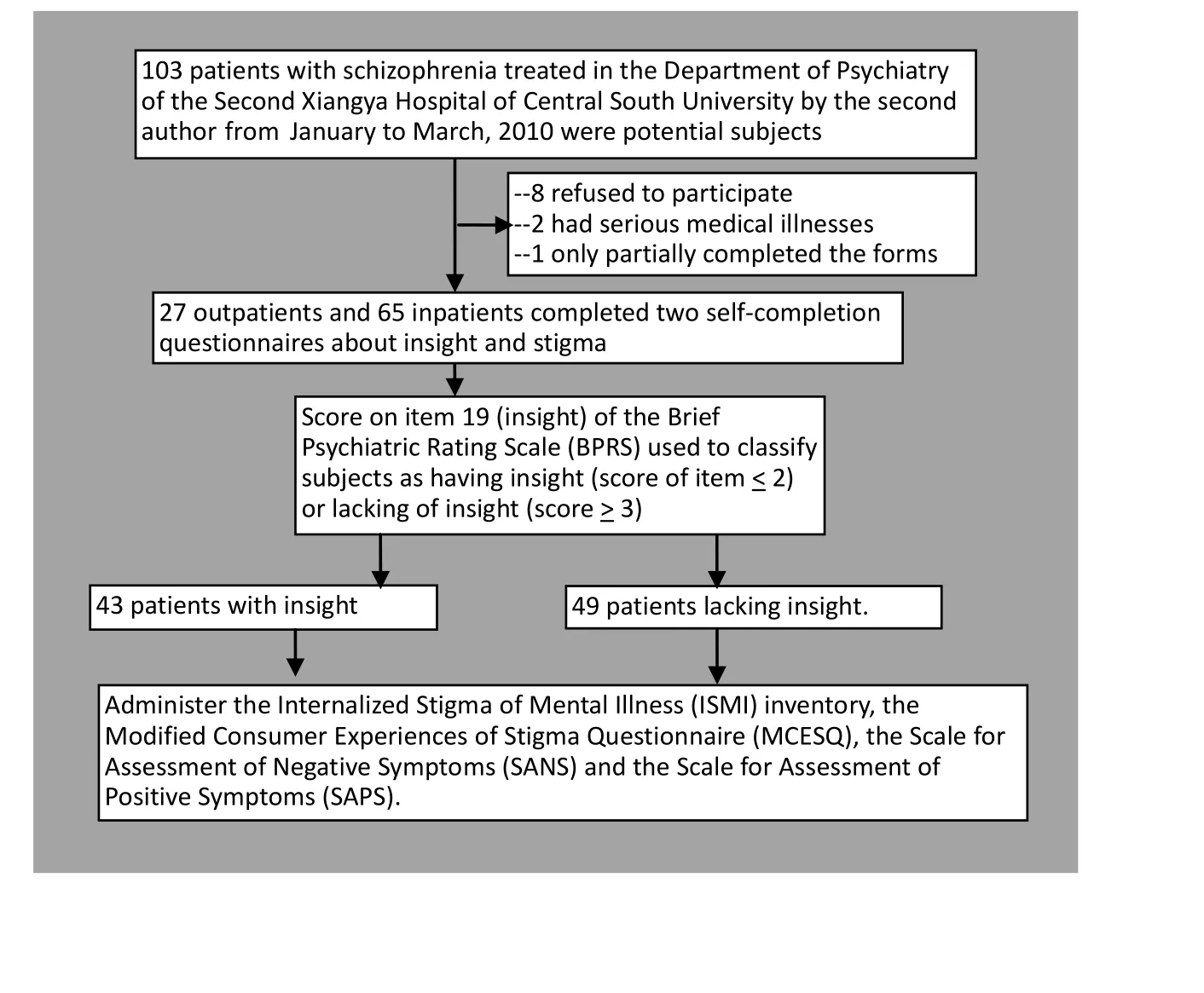
Figure 1. Enrollment and follow-up of subjects
2.2.3 Assessment of stigma
Two self-completion instruments for assessing stigma were translated by the second author. The reliability and validity of the Chinese versions of these instruments have not yet been fully assessed.
The Internalized Stigma of Mental Illness (ISMI) inventory, developed by Ritsher and colleagues in 2003[12]contains 29 items scored on a 4-point Likert scales (1=‘strongly disagree’ to 4=‘strongly agree’) that are assorted into five subscales: alienation (six items reflecting the respondent’s feeling of participation in the society; alpha in current study=0.70), stereotype endorsement (seven items reflecting the respondent's tendency to endorse stereotyped impressions of psychiatric patients, alpha=0.67), discrimination experience (five items reflecting the respondent's experiences of unfair treatment due to other people's discrimination, alpha=0.63), social withdrawal (six items reflecting the respondent’s experience of frequent refusal by others due to his mental disorder, alpha=0.73), and stigma resistance (five items reflecting respondent’s perceived ability to deflect stigma, alpha=0.01). Based on previous studies, four subscales (excluding stigma resistance) are used to calculate the adjusted total score of stigma; in the current study this adjusted total score had good internal consistency (alpha=0.85).
The Modified Consumer Experiences of Stigma Questionnaire (MCESQ), compiled by Wahl and colleagues[13-14]is mainly used to assess respondents' expected sense of mental disorder-related stigma as well as their actual experience of stigma and discrimination. It contains 19 items scored on five point Likert scales (1=never to 5=always) and is divided into two subscales: the Stigma Experiences Scale (with nine items, alpha in current study=0.70) and the Discrimination Experiences Scale (with ten items, alpha in current study=0.50). In the current study the internal consistency of the total 19-item scale is poor (ICC=0.67).
2.2.4 Assessment of psychotic symptoms
Chinese versions of the Scale for the Assessment of Negative Symptoms (SANS) and the Scale for the Assessment of Positive Symptoms (SAPS), developed by Andreasen in 1982,[11]were used for the assessment of negative symptoms and positive symptoms in the participants. The SANS contains 24 items and the SAPS contains 34 items scored on six-point Likert scales (0=not present to 5=severe). The SANS is divided into five subscales: affective blunting; alogia (impoverished thinking); avolition/apathy; anhedonia/asociality; and disturbance of attention. The SAPS is divided into four subscales: hallucinations, delusions, bizarre behavior, and positive formal thought disorder. A high score is interpreted as having prominent negative or positive symptoms. The Chinese versions of the scales have good reliability and validity.[11]
2.3 Research process
SANS, SAPS, BPRS, and insight were assessed simultaneously. The assessments were conducted by two trained doctoral candidates who had good testretest reliability (ICC=0.80-0.95 for SAPS items and 0.80-0.88 for SANS items). The two self-rated scales about stigma were completed by patients immediately after the clinician-conducted evaluations (in the presence of the researcher). After the researchers read the instructions, subjects completed the forms on their own but were free to ask questions if they did not understand specific items. Researchers read the entire questionnaire to six subjects who were unable to understand the instrument because they were semiliterate. On average it took patients 30-40 minutes to complete the two self-completion instruments.
2.4 Statistical methods
All the data were processed using SPSS 17.0 software. Statistical analyses included descriptive statistics, t-tests, chi-square tests, and Mann-Whitney U tests.
3. Results
3.1 Characteristics of the sample
A total of 92 patients completed valid forms. There were 43 patients with a score of two or more on the BPRS insight item and, thus, classified as ‘lacking insight’; the remaining 49 subjects were classified as having insight into their illness. The demographic characteristics of the two groups are shown in Table 1. Compared to patients with insight, those lacking insight had a significantly shorter duration of illness, were more likely to be inpatients, and (at trend level only) had more prominent positive and negative symptoms.
3.2 Comparison of stigma in those with and without insight
Comparison of the mean total scores and mean subscale scores of the two self-completion assessments of stigma (Table 2) between patients with and without insight found that only the alienation subscale score of the ISMI was significantly different; patients with insight reported a greater feeling of alienation than those without insight. There was also a trend finding (p=0.068) of higher internalized stigma on the MCSQ in patients with insight. None of the other subscale scores of theISMI or MCESQ were significantly different between patients with and without insight; but the power of these assessments was under 80% for all except one of the comparisons.
Item-level comparisons of the two groups also found few differences. Only 1 of the 19 items on the MCESQ showed a significant difference: patients without insight were more likely to report being refused a driver’s license or other document because of prior psychiatric treatment (mean [sd] items score, 1.56 [0.85] v. 1.15 [0.46], t=2.82, p=0.006). And only 4 of the 29 items on the ISMI were significantly different: patients with insight were more likely to report feeling inferior to others (2.14 [0.68] v. 1.79 [0.74], t=2.38, p=0.019), more likely to report feeling hopeless because of having a mental illness in the family (2.37 [0.70] v. 2.05 [0.72], t=2.16, p=0.033), more likely to report needing to have others make their decisions for them (2.41 [0.71] v. 2.09 [0.68], t=2.17, p=0.033), and more likely to report restricting their social activities for fear that they be perceived as being strange (2.42 [0.74] v. 2.12 [0.70], t=1.99, p=0.050).
The ranked correlation of the score of BPRS item 19 (on stigma) with the total score of the ISMI was 0.21 (p=0.053) and the correlation of the item with the total MCESQ score was 0.003 (p=0.977).
3.3 Comparison of stigma in those with and without insight
Table 3 shows the results of a logistic regression analysis using lack of insight as the dependent variable and demographic and clinical variables as independent variables. Only the inpatient versus outpatient status of the patient remained statistically significant when all variables were considered in the logistic model: as expected, inpatients were less likely to have insight into their illness than outpatients. The scores on the self-completion scales (MCESQ and ISMI) and on the clinician-administered clinical scales (SAPS and SANS) were not significantly associated with lack of insight as defined by item 19 of the BPRS. Stepwise logistic regression analysis (not shown) had the same result.
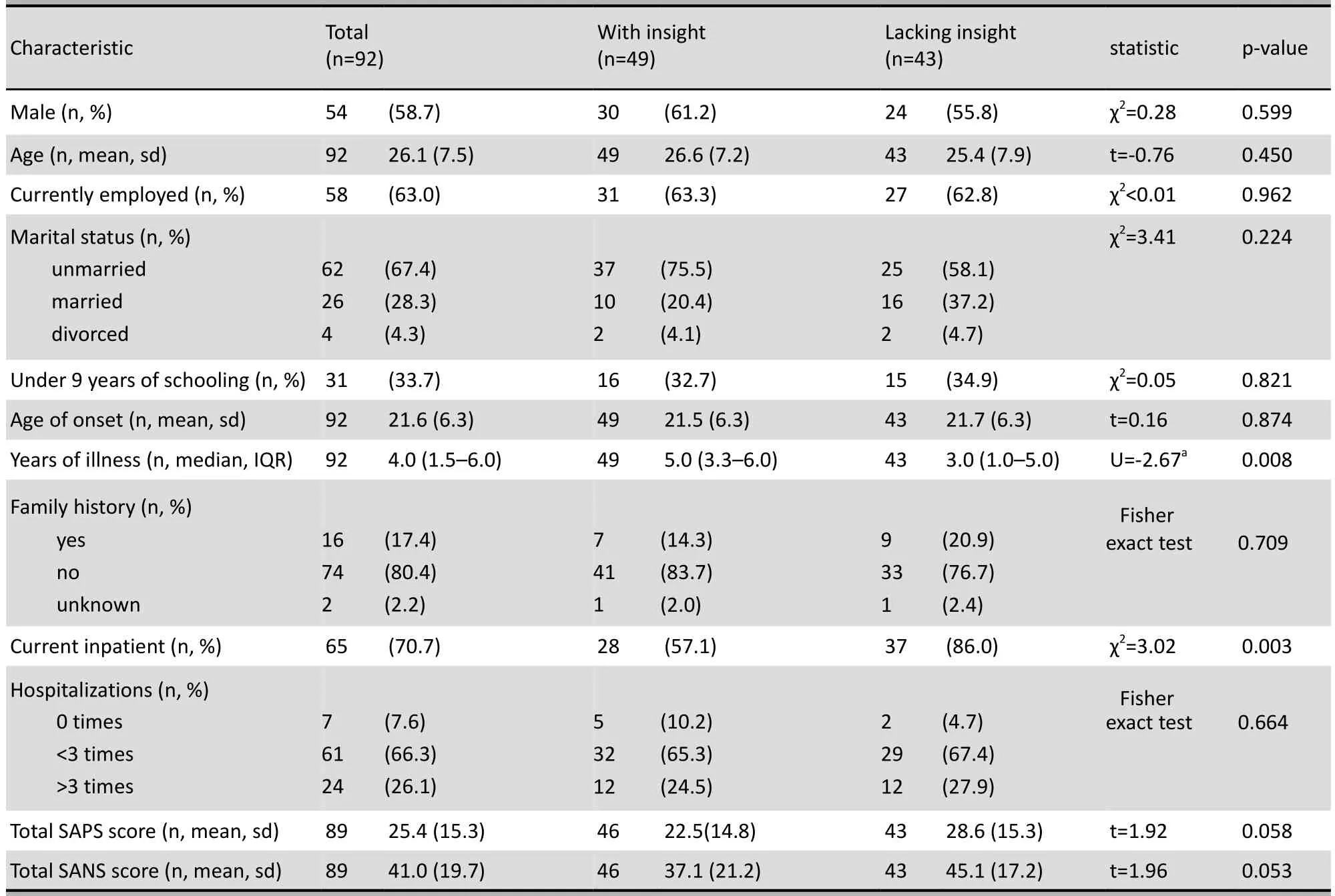
Table 1. Comparison of demographic and clinical data characteristics of patients with schizophrenia with and without insight into their illness
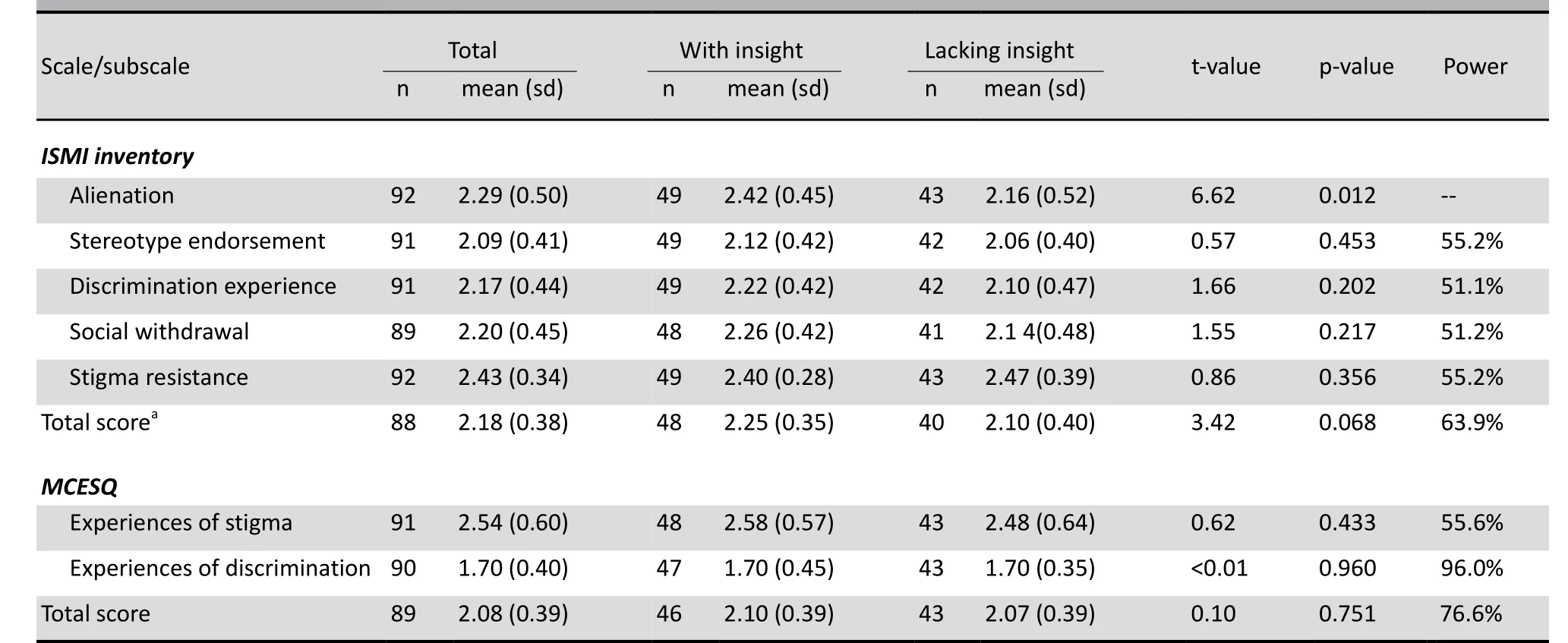
Table 2. Mean (sd) total scores and subscale scores on the Internalized Stigma of Mental Illness (ISMI) inventory and the Modified Consumer Experiences of Stigma Questionnaire (MCESQ) for patients with schizophrenia who do and do not have insight into their illne
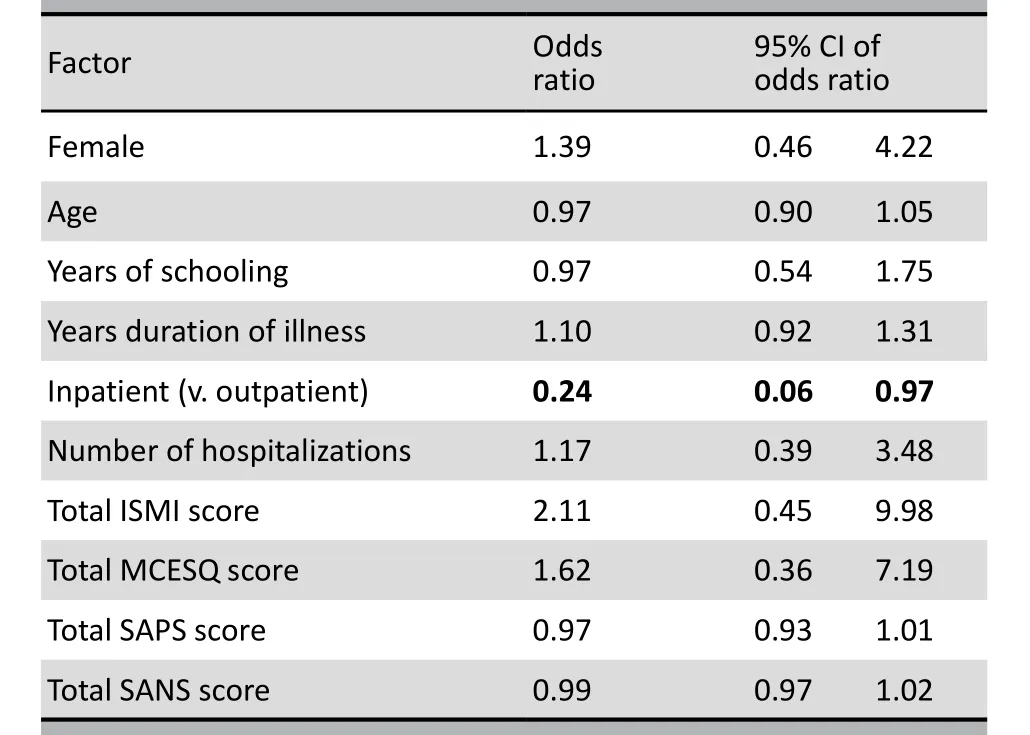
Table 3. Logistic regression of factors associated with having insight into the illness among 92 patients with schizophrenia
4. Discussion
4.1 Main findings
This study among inpatients and outpatients with schizophrenia in China only provided weak support for previous studies that report increased experience of stigma among patients who have better insight.[8]Among the eight subscales of the two self-report instruments used to assess stigma only one (alienation) was significantly more prominent in patients with insight into their illness than in those without insight. And among the 48 individual items in the two scales about stigma considered only five were statistically significant between patients with and without insight into their illness—this is little more than would be expected by chance given the number of items that were being compared. Further studies with a wider spectrum of patients that make more detailed assessments of stigma and insight and that follow fluctuations in insight and experiences of stigma over time are needed to clarify the complex relationship between these two phenomena in patients with schizophrenia.
4.2 Limitations
There are several limitations in this preliminary project. (a) A more detailed evaluation of the reliability and validity of the Chinese versions of the two instruments used to assess stigma in this study (ISMI and MCESQ) is needed and the scales may need to be adapted for use in mainland China. (b) The classification of insight used in this study was based on the score of a single BPRS item so it may not have captured all important aspects of the construct. (c) Insight can change rapidly as a patient’s condition improves or gets worse, whereas stigma is typically experienced over longer periods of time, so longitudinal studies that monitor levels of insight and stigma over time are needed to get a more sensitive evaluation of the relationship of these phenomena. (d) The power of the comparison of subscale scores between patients with and without insight was quite low so the negativefindings may have been due to Type II errors; larger samples will be needed confirm or disprove the significance of the findings. (e) The relatively small sample size also made it impossible to compare the relationship of stigma and insight in important subgroups such as inpatients versus outpatients, firstonset versus chronic patients, males versus females, and so forth. (f) The median duration of illness in the patients included in the study was four years; the relationship between insight and stigma may be different in patients with shorter durations of illness.
4.3 Significance
One of the currently most influential theories of stigma in mental illness is a modified labeling theory proposed by Link and colleagues.[16]According to this theory members of a society internalize stereotyped beliefs about mentally ill individuals (e.g., a burden on society, potentially dangerous, etc.) which are then used to ‘label’ psychiatric patients when they make contact with the health care system. Patients then have to use cognitive and behavioral strategies to deal with these external labels. These strategies include keeping their psychiatric treatment secret, refusing to come into contact with the medical system, and intentional restriction of their social worlds (which may magnify their disability).
Compared with Western countries, the dominant ideology in China for the last 2000 years has been Confucianism which promotes loyal and supportive relationships among family members and a relatively rigid social and interpersonal support network. In this sociocultural setting ‘face’, the status ascribed to a person by those in his or her social network, is an integral component of an individual’s social identity.‘Never lose face’ is a paramount social objective because loss of face inevitably isolates one from the social network. Because of the public's negative stereotypes about mental disorders,[17,18]once a individual is identified as a psychiatric patient the negative information conveyed by such a label will make the patient lose face and, thus, suffer a serious blow to his or her social status and a corresponding decrease in self-esteem.[19]
Previous research from other countries suggests that as a patient with schizophrenia regains insight during the course of treatment there is an increased awareness of the negative social stereotypes associated with their illness and, thus, increased internalized stigma.[4]In the Chinese context this potentially serious loss of face often causes patients and their family members to go to great lengths to keep information about the illness secret (45% of the patients in the current study had done so). It is important that clinicians are aware of this tendency and actively take steps to reduce internalized stigma both in patients and in their family members because this can directly affect adherence to treatment regimens and social re-integration. More research is urgently needed to determine how best to achieve this goal.
Conflict of interest
The authors report no conflict of interest related to this study.
Funding
The study was supported by the Shanghai Key Laboratory of Forensic Medicine (grant number: KF0908).
1. Goffman E. Stigma: notes on the management of spoiled identity.New York: Prentice Hall, 1963:3.
2. Link BG, Phelan M, Bresnhahan M, Stueve A, Pescosolido BA. Public conceptions of mental illness: labels, causes, dangerousness and social distance. Am J Public Health 1999;89 (9): 1328-1333.
3. Phelan JC, Link BG, Stueve A, Pescosolido BA. Public conceptions of mental illness in 1950 and 1996: what is mental illness and is it to be feared? Journal of Health and Social B 2000; 41(2):188-207.
4. Ritsher JB, Phelan JC. Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Res 2004; 129(3): 257-265.
5. Phillips MR, Pearson V, Li FF, Xu MJ, Yang L. Stigma and expressed emotion: a study of people with schizophrenia and their family members in China. Br J Psychiatry 2002;181:488-493.
6. Gao SY, Fei LP, Wang XQ,Xu D,Jia ZM, Gao WC. Experience of stigma among patients with schizophrenia and their family members and attitudes of different groups about this stigma. Chinese Mental Health Journal 2005;19(2):82-85. (in Chinese)
7. Guo QF, Lu SC, Zhang YH. Experience of discrimination and coping styles of schizophrenia patients in the convalescent period. Chinese Journal of Nursing 2010;45(8):677-680. (in Chinese)
8. Liu WQ, Tan LW, Wan F,Wang LF. Social discrimination on patients with mental disorders: Status quo, reasons, and countermeasures. Medicine and Philosophy (Clinical Decisionmaking) 2008; 29(1):69-71. (in Chinese)
9. Mak WWS, Wu CFM. Cognitive insight and causal attribution in the development of self-stigma among individuals with schizophrenia. Psychiatric Serv 2006; 57(12):1800-1802.
10. Lysaker PH, Roe D, Yanos PT. Toward understanding the insight paradox: internalized stigma moderates the association between insight and social functioning, hope, and self-esteem among people with schizophrenia spectrum disorders. Schizophr Bull 2007; 33(1): 192-199.
11. Zhang MY. Handbook of Evaluation Scales in Psychiatry. Changsha: Hunan Science and Technology Press, 2003:81-94, 94-111. (in Chinese)
12. Ritsher,JB, Otilingam PG, Grajales M. Internalized stigma of mental illness: psychometric properties of a new measure. Psychiatry Res 2003; 121(1): 31-49.
13. Wahl OF. Mental health consumers' experience of stigma. Schizophr Bull 1999; 25(3):467-478.
14. Dickerson FB, Sommerville J, Origoni AE, Ringel NB, Parente F. Experiences of stigma among outpatients with schizophrenia. Schizophr Bull 2002; 28(1): 143-155.
15. Phillips MR, Xiong W, Wang RW, Gao YH, Wang XQ, Zhang NP. Reliability and validity of the Chinese versions of the scales for assessment of positive and negative symptoms. Acta Psychiatr Scand 1991; 84(4):364-370.
16. Link BG, Cullen FT, Struening E, Shrout PE, Dohrenwend BP. A modified labeling theory approach to mental disorders: an empirical assessment. Am Sociol Rev 1989; 54(3):400-423.
17. Gao SY, Fei LP. Attitudes about mental illness of different types of respondents in Beijing. Chinese Mental Health Journal 2001;15(2):107-109. (in Chinese)
18. Tsang HWH, Tam PKC, Chan F, Cheung WM. Stigmatizing attitudes towards individuals with mental illness in Hong Kong: implications for their recovery. J Community Psychol 2003;31(4):383-396.
19. Livingston JD, Rossiter KR, Verdun-Jones SN.‘Forensic’labelling: an empirical assessment of its effects on self-stigma for people with severe mental illness. Psychiatry Res 2011;188(1):115-122. doi:10.1016/j.psychres.2011.01.018.
2011-09-08; accepted: 2012-02-08)
10.3969/j.issn.1002-0829.2012.02.004
1Mental Health Institute of the Second Xiangya Hospital, Central South University, Changsha, China
2Forensic Psychiatry Department of Nanjing Brain Hospital, Nanjing Medical University, Nanjing, China
*Correspondence: xiaop6@gmail.com
- 上海精神醫(yī)學(xué)的其它文章
- Latent variable modeling
- Cross-sectional survey of prevalence and personality characteristics of college students with internet addiction in Wenzhou, China
- Symptom severity is more closely associated with social functioning status in inpatients with schizophrenia than cognitive deficits
- Hemispheric dominance during the mental rotation task in patients with schizophrenia
- Case report on clozapine-associated neuroleptic malignant syndrome
- Clozapine is underutilized